By The RX Index Editorial Team · 5 medications compared · BP trial data verified April 9, 2026
Last verified: · Trial data · pricing verified April 9, 2026
Editorial Standards · Affiliate Disclosure · Next audit: May 9, 2026
BEST GLP-1 FOR HIGH BLOOD PRESSURE — 2026 COMPLETE GUIDE
Best GLP-1 for High Blood Pressure
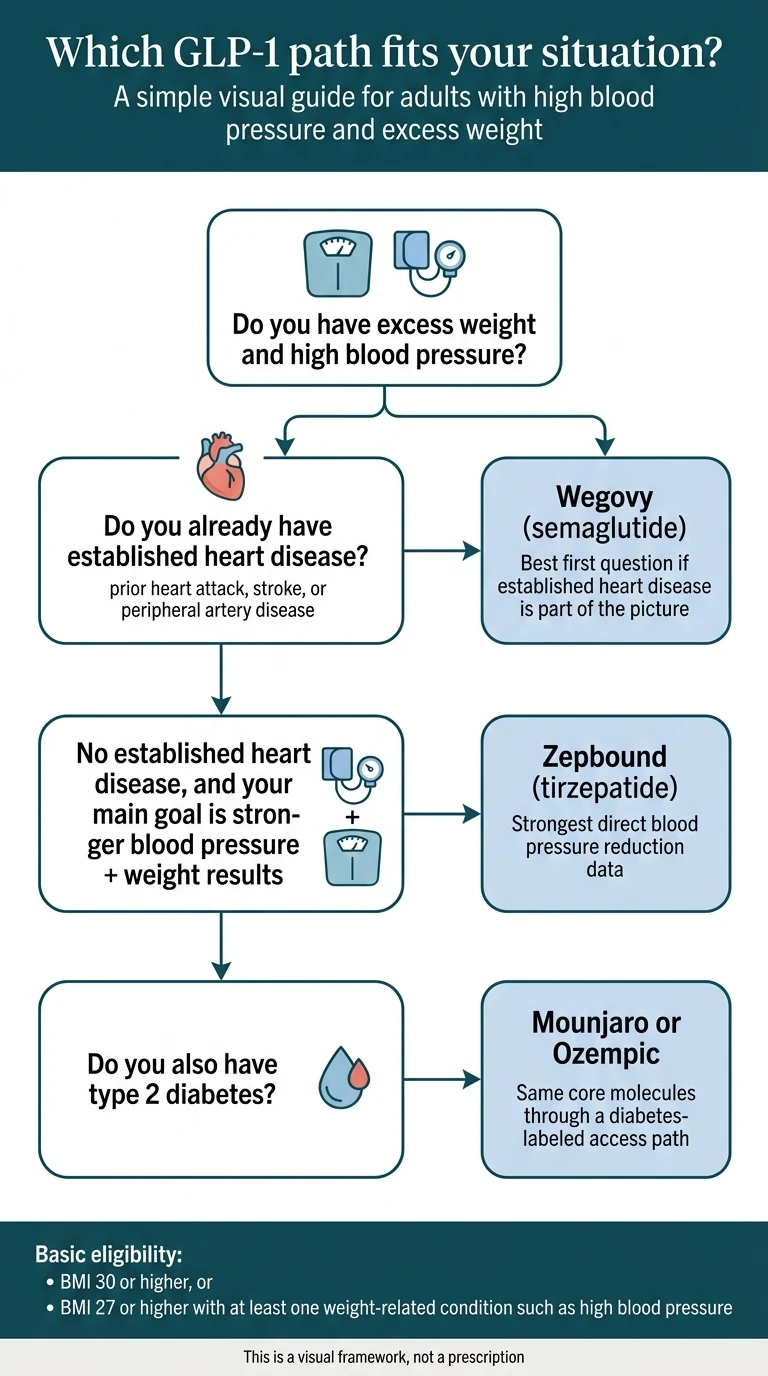
Bottom line: Zepbound (tirzepatide) is the best GLP-1 for high blood pressure for most adults with excess weight. In a 36-week substudy of the SURMOUNT-1 trial, tirzepatide lowered systolic blood pressure by 7.4 to 10.6 mmHg — roughly double what semaglutide achieves. It also produced the most weight loss of any GLP-1 medication tested head-to-head.
The one exception: If you already have established cardiovascular disease (prior heart attack, stroke, or peripheral artery disease), Wegovy (semaglutide) is the better first choice. It's the only GLP-1 with an FDA-approved indication to reduce cardiovascular death, heart attack, and stroke in adults with both heart disease and overweight or obesity.
If you don't have established heart disease and your main concern is getting blood pressure down alongside meaningful weight loss, Zepbound is where the strongest evidence points. The rest of this page shows you exactly why, handles every exception that could change the answer, and helps you figure out your best next step.
QUICK ANSWER
🏆 Best overall for blood pressure: Zepbound (tirzepatide) — 7–11 mmHg systolic reduction
❤️ Best if you have established heart disease: Wegovy (semaglutide) — FDA-approved CV risk reduction
💊 Best if you also have type 2 diabetes: Mounjaro (tirzepatide) or Ozempic (semaglutide) — same active ingredients, diabetes-labeled access
Already know which medication fits your situation? Check your eligibility with a licensed telehealth provider below.

Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
What is the best GLP-1 for high blood pressure?
Tirzepatide (the active ingredient in Zepbound and Mounjaro) has the strongest blood pressure reduction data of any GLP-1-class medication studied to date. Semaglutide (Wegovy, Ozempic) comes in second. Every other GLP-1 trails both by a meaningful margin.
We assembled the comparison below from published randomized controlled trial data and peer-reviewed meta-analyses. The table combines BP reduction, weight loss, cardiovascular outcomes status, heart rate effect, and access pathway for every major GLP-1 — a combination we could not find on any single page when we reviewed the top-ranking results for this query (SERP reviewed April 9, 2026).
The RX Index GLP-1 Blood Pressure Comparison (April 2026)
| Medication | Best Verified Systolic BP Reduction | Avg Weight Loss | CV Event Evidence | Heart Rate | Best For | Key Trial |
|---|---|---|---|---|---|---|
| Zepbound (tirzepatide) | −7.4 to −10.6 mmHg | 15–22.5% body weight | Noninferior to dulaglutide for MACE (HR 0.92; SURPASS-CVOT, NEJM Dec 2025) | +2.1 to +5.4 bpm | BP-first + maximum weight loss | SURMOUNT-1 ABPM substudy, Hypertension 2024 |
| Wegovy (semaglutide 2.4 mg) | −4.8 to −5.0 mmHg | ~15% body weight | Yes — 20% MACE reduction vs placebo (SELECT) | +1 to +4 bpm | Established heart disease + obesity | SELECT trial; Kennedy 2024 IPD meta-analysis, Eur Heart J |
| Mounjaro (tirzepatide) | Same as Zepbound (same molecule) | 5.7–12.9 kg (diabetes trials) | Same as Zepbound (SURPASS-CVOT) | +2.1 to +5.4 bpm | T2D + high BP | SURPASS-2, -4, -CVOT |
| Ozempic (semaglutide 1.0 mg) | −2.3 to −3.7 mmHg | ~5–10% body weight | Yes — SUSTAIN-6 (T2D); FDA-approved CKD risk reduction (Jan 2025) | +2 to +3 bpm | T2D + CV risk + CKD | SUSTAIN 1-5; Cui meta-analysis 2023 |
| Saxenda (liraglutide 3.0 mg) | −2 to −6 mmHg | ~5–8% body weight | CV safety demonstrated per FDA label; LEADER: 13% MACE reduction (Victoza 1.8 mg) | +2 to +4 bpm | Daily-dosing preference | SCALE trials; Saxenda FDA label |
Key sources: SURMOUNT-1 ABPM substudy (de Lemos et al., Hypertension, Feb 2024). SURMOUNT-1 72-week stratified analysis (Karkare et al., BMJ Open, Sept 2024): −6.8 mmHg SBP vs placebo, 58% of tirzepatide patients achieved normal BP vs 35.2% placebo. SURPASS-CVOT (Nicholls et al., NEJM, Dec 18, 2025): tirzepatide noninferior to dulaglutide for MACE, HR 0.92, 16% lower all-cause mortality. SELECT trial (Lincoff et al., NEJM, 2023).
Why those numbers matter more than you think
A sustained 5 mmHg drop in systolic blood pressure reduces your risk of heart attack and stroke by approximately 10%, according to a meta-analysis in The Lancet. Tirzepatide's 7–11 mmHg reduction approaches what you'd get from adding a new blood pressure medication to your regimen — while simultaneously producing 15–22% body weight loss.
Is Zepbound or Wegovy better if you have high blood pressure?
For most readers — adults with excess weight whose primary concern is high blood pressure — Zepbound is the stronger choice based on the available BP data. But one detail can flip the answer entirely: whether you already have established cardiovascular disease.
Why Zepbound wins the BP-first question
The SURMOUNT-1 ambulatory blood pressure monitoring substudy is the single best piece of evidence here. Nearly 600 adults with obesity wore 24-hour BP monitors at baseline and again at 36 weeks. The results, published in Hypertension (February 2024):
- Tirzepatide 5 mg: −7.4 mmHg systolic BP reduction
- Tirzepatide 10 mg: −10.6 mmHg systolic BP reduction
- Tirzepatide 15 mg: −8.0 mmHg systolic BP reduction
These reductions were consistent across daytime and nighttime readings — important because nighttime blood pressure is a stronger predictor of cardiovascular death.
In the 72-week post-hoc analysis (Karkare et al., BMJ Open, 2024), 58% of tirzepatide patients had normal blood pressure at week 72, compared to just 35.2% on placebo. About 68% of the systolic and 71% of the diastolic BP effect was driven by weight loss — and since tirzepatide produces more weight loss than semaglutide head-to-head (SURMOUNT-5: 20.2% vs 13.7% at 72 weeks), the math follows.
Why Wegovy wins if you already have heart disease
Important distinction
Zepbound does not have Wegovy's FDA-approved cardiovascular risk reduction indication. The SURPASS-CVOT trial (Nicholls et al., NEJM, December 2025) showed tirzepatide was noninferior to dulaglutide for cardiovascular events (HR 0.92) — meaningful, but an active-comparator trial, not a placebo-controlled superiority trial.
Wegovy remains the only GLP-1 with an FDA-approved indication specifically to reduce cardiovascular death, heart attack, and stroke in adults with established cardiovascular disease and overweight or obesity. That indication is based on SELECT — 17,604 participants, 20% MACE reduction versus placebo.
Our recommendation: If your cardiologist has raised cardiovascular event reduction as a treatment goal, start the conversation with Wegovy. If your primary concern is blood pressure and weight without established heart disease, the BP data favors Zepbound.
One more thing on Wegovy: Wegovy HD (semaglutide 7.2 mg), FDA-approved March 19, 2026, pushes semaglutide's weight loss ceiling to approximately 21% — narrowing the gap with tirzepatide. Available nationwide as of April 2026 at $399/month self-pay, or $199/month for new patients starting on lower titration doses (through June 30, 2026). BP-specific data for the 7.2 mg dose has not been separately published, but a modestly stronger BP effect than the 2.4 mg dose is plausible given the additional weight loss.
Already have heart disease? → Read our Wegovy for Heart Disease guide
If your main issue is high blood pressure and weight — not existing heart disease — Zepbound is the strongest first option.
Takes about 60 seconds · Free · No commitment
See If You Qualify for Zepbound — Free via RoWhy is Zepbound the best GLP-1 for most people with high blood pressure?
The case rests on three things: the strongest direct BP reduction data, the greatest weight loss, and an FDA approval that explicitly includes hypertension as a qualifying comorbidity.
The blood pressure numbers in context
In the SURMOUNT-1 stratified analysis, tirzepatide's BP-lowering effect was consistent regardless of whether participants had normal blood pressure, elevated blood pressure, or stage 1/stage 2 hypertension at baseline. The drug shifted the entire blood pressure distribution curve leftward, moving people from hypertensive ranges into normal territory.
The researchers concluded that “pharmacological treatment of obesity with tirzepatide may be a novel strategy to help prevent or control hypertension.”
Why weight loss matters even if you only care about blood pressure
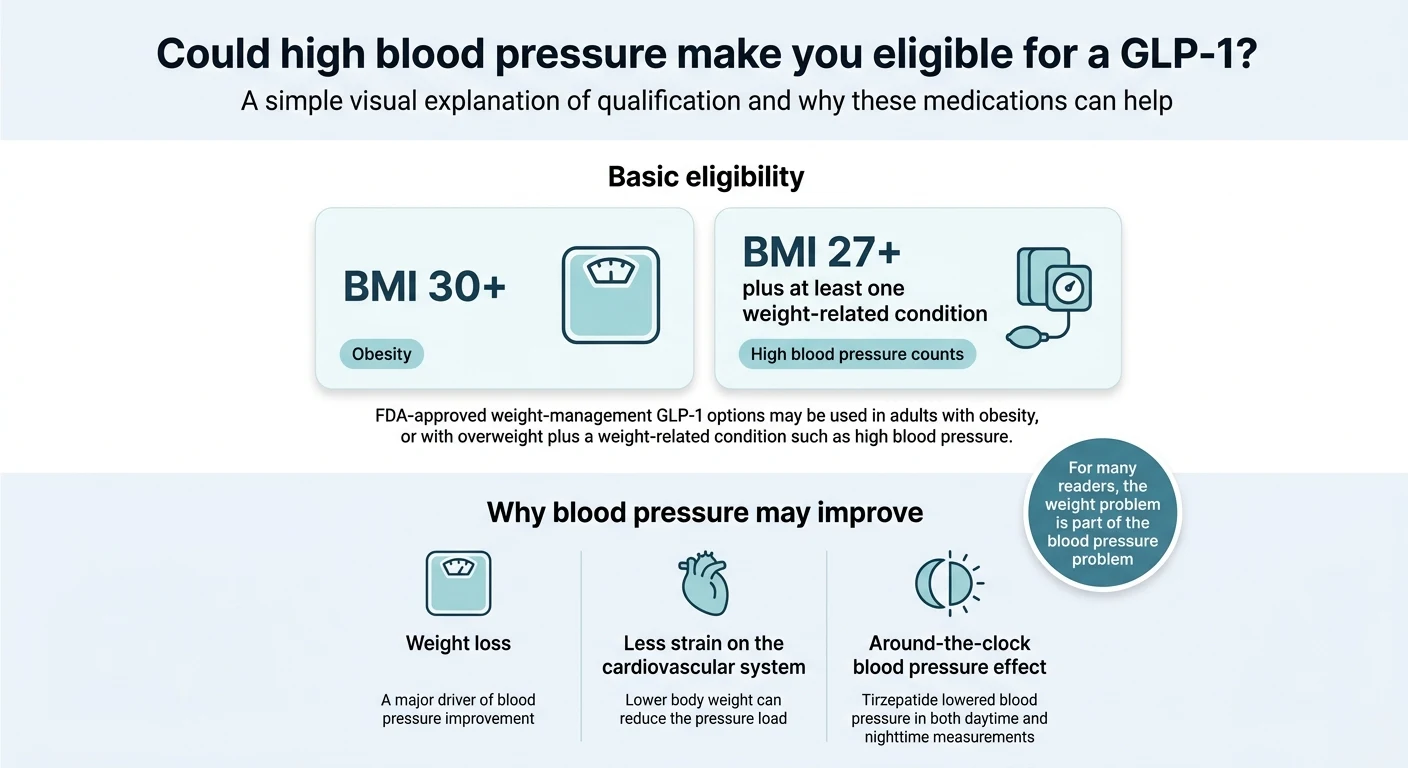
About 65–78% of primary hypertension cases are caused by excess body weight, according to estimates cited in the American Journal of Hypertension (2025). Obesity is the single most significant modifiable risk factor for resistant hypertension, with 56–91% of resistant hypertension patients classified as overweight or obese (Lancet eClinicalMedicine, 2024).
For many people with high blood pressure, the weight is the blood pressure problem. You're not treating two conditions — you're treating one condition that shows up in two ways. Tirzepatide addresses both more aggressively than any other option in this class.
What patients are actually experiencing
A Mayo Clinic Connect member described having their doctor reduce blood pressure medications because the GLP-1 was bringing readings too low. This is consistent with the trial data: in the semaglutide IPD meta-analysis, patients on the active drug were approximately twice as likely to have their BP medications de-escalated.
The sleep apnea connection most pages miss
Obstructive sleep apnea is strongly linked to both obesity and resistant hypertension. On December 20, 2024, the FDA approved Zepbound for moderate-to-severe OSA in adults with obesity — making it the first medication ever approved for that indication. If you snore heavily, wake up tired, or have been told you stop breathing at night, this is another reason Zepbound specifically may be the right GLP-1 for your situation.
Who should NOT default to Zepbound
- Established cardiovascular disease → Wegovy has the FDA-approved CV risk reduction indication.
- Personal or family history of medullary thyroid carcinoma (MTC) or MEN2 → All GLP-1s are contraindicated.
- Severe gastroparesis → GLP-1 medications that slow gastric emptying are not recommended.
- Type 2 diabetes with insurance barriers → Mounjaro (same molecule, diabetes label) may be easier to get covered.
What if you also have type 2 diabetes?
If you have type 2 diabetes alongside high blood pressure, the “best” medication might not change — but the access path probably does.
Mounjaro is the same active molecule as Zepbound (tirzepatide), but it's FDA-approved for type 2 diabetes rather than weight management. For many patients, the diabetes label opens up insurance coverage that the obesity label doesn't. The ACC's 2025 guidance makes this point directly: availability, affordability, and insurance coverage often dictate final agent selection.
Ozempic (semaglutide 1.0 mg) is the diabetes-labeled sibling of Wegovy. And there's a third scenario worth flagging: if you also have chronic kidney disease, Ozempic gained an FDA-approved indication in January 2025 to reduce the risk of worsening kidney disease in adults with T2D and CKD. That's a meaningful differentiator that most comparison pages miss entirely.
Here's how to think about it:
- T2D + high BP, no heart disease or CKD: Mounjaro — same tirzepatide molecule, strongest BP signal, diabetes-benefit access.
- T2D + high BP + established heart disease: Ozempic — semaglutide's cardiovascular outcomes data through a diabetes-coverage pathway.
- T2D + high BP + chronic kidney disease: Ozempic — the dedicated CKD indication makes it the best practical option when all three conditions are present.
- T2D + high BP + maximum weight loss priority: Ask your prescriber about Mounjaro at higher doses (up to 15 mg).
Have type 2 diabetes as your primary condition? → See our dedicated diabetes GLP-1 comparison
How do GLP-1 medications lower blood pressure?
GLP-1 medications reduce blood pressure through at least four overlapping mechanisms. Understanding them explains why some people see dramatic BP drops while others see modest ones.
Weight-mediated vs. weight-independent effects
The SURMOUNT-1 stratified analysis found that weight loss explained 68% of the systolic and 71% of the diastolic blood pressure reduction from tirzepatide. The semaglutide IPD meta-analysis found a similar pattern. That means roughly 30% of the BP benefit comes from something other than weight loss — a meaningful independent effect.
- Weight loss (~70% of the effect). Tirzepatide produces 20–22.5% body weight loss at higher doses. Semaglutide 2.4 mg produces ~15%. Wegovy HD 7.2 mg pushes to ~21%. More weight lost → more blood pressure reduced. Excess adipose tissue drives hypertension through increased sympathetic activity, insulin resistance, RAAS overactivation, and direct mechanical stress.
- Increased sodium excretion (natriuresis). GLP-1 receptors in the kidneys promote sodium excretion through selective suppression of angiotensin II — confirmed in liraglutide research published in Scientific Reports (2024).
- Improved blood vessel function. GLP-1 receptor activation improves endothelial function, reduces vascular inflammation, and promotes mild vasodilation.
- RAAS modulation. GLP-1 medications modulate the renin-angiotensin-aldosterone system by lowering angiotensin II levels — the same system targeted by ACE inhibitors and ARBs, approached from a different angle.
What about the heart rate increase?
Every GLP-1 increases resting heart rate slightly — about 2 to 5 bpm on average. Tirzepatide at 15 mg showed +5.4 bpm. Despite this, the blood pressure reduction + weight loss + anti-inflammatory effects more than compensate. The ACC review stated: “Even this relatively small drop in BP — that of about a half medication — can result in considerable overall improvement in cardiovascular risk.”
Can you take a GLP-1 with blood pressure medication?
Yes. GLP-1 medications are generally safe alongside ACE inhibitors, ARBs, calcium channel blockers, beta-blockers, and diuretics.
What frequently happens is the opposite of what people expect: patients on GLP-1s often need less blood pressure medication, not more.
In the semaglutide IPD meta-analysis (Kennedy et al., 2024), 10.9% of patients on semaglutide had their BP medications de-escalated vs 5.2% on placebo. Among patients with resistant hypertension, 26.9% on semaglutide had BP meds reduced vs 3% on placebo.
Watch for: lightheadedness, dizziness when standing, nausea, fatigue — signs your current BP medications may be too strong now. If you're also taking a diuretic, the combined fluid loss from GLP-1 side effects can amplify this.
Home monitoring checklist
- Get a validated home BP monitor before starting
- Check at the same time daily (morning, before medications)
- Log readings in a notebook or app
- Contact your prescriber if systolic consistently drops below 100 mmHg or you feel dizzy
- Never stop or reduce BP medications on your own
Can GLP-1 medications help resistant hypertension?
Resistant hypertension — blood pressure above target despite three or more medications including a diuretic — affects roughly 10–30% of people with hypertension. Obesity is the single most significant modifiable risk factor, with 56–91% of resistant hypertension patients classified as overweight or obese.
No clinical trial has tested GLP-1 medications for resistant hypertension as a primary endpoint. But the signal is hard to ignore: in the semaglutide IPD meta-analysis, 26.9% of patients with apparent resistant hypertension had their BP medications reduced on semaglutide, versus 3% on placebo. The Lancet eClinicalMedicine (2024) specifically proposed GLP-1-based therapies as a treatment strategy for this population.
If you have resistant hypertension plus excess weight, a GLP-1 addresses the one thing your current pills cannot: the obesity driving the resistance.
Dealing with resistant hypertension?
A licensed provider can evaluate your full medication picture and determine if a GLP-1 fits your situation.
Start With a Licensed Provider — Free Eligibility CheckWhat does a GLP-1 for high blood pressure actually cost in 2026?
Most pages get vague here. Here are the actual numbers.
Zepbound (tirzepatide) — LillyDirect self-pay pricing
| Dose | Standard Price | Self Pay Journey Program |
|---|---|---|
| 2.5 mg (starting) | $299/mo | $299/mo |
| 5 mg | $399/mo | $399/mo |
| 7.5 mg | $499/mo | $449/mo (refill within 45 days) |
| 10 mg | $699/mo | $449/mo (refill within 45 days) |
| 12.5 mg | $699/mo | $449/mo (refill within 45 days) |
| 15 mg | $699/mo | $449/mo (refill within 45 days) |
Source: Lilly Self Pay Journey Program, effective Feb 23, 2026. Single-dose vial pricing. KwikPen starts at $299/mo. With commercial insurance + Savings Card: as low as $25/mo.
Wegovy (semaglutide) — NovoCare self-pay pricing
| Dose | Self-Pay Price |
|---|---|
| 0.25 mg, 0.5 mg (titration) | $199/mo (new patient offer through June 30, 2026) |
| 1 mg, 1.7 mg, 2.4 mg | $349/mo |
| 7.2 mg (Wegovy HD) | $399/mo |
Source: NovoCare, April 2026. With commercial insurance + Savings Card: as low as $25/mo.
Medicare and government beneficiaries
Both Lilly's and Novo's savings cards exclude government beneficiaries (Medicare, Medicaid, Tricare). Medicare Part D generally does not cover weight-loss medications, though coverage pathways are evolving. You can still use LillyDirect self-pay at cash prices. A Medicare GLP-1 Bridge program for Zepbound KwikPen is expected mid-2026.
Related: How to Get Insurance to Cover GLP-1 Medications · GLP-1 Cost Without Insurance
What about compounded GLP-1s for high blood pressure?
The regulatory landscape shifted significantly in early 2026.
Compounded GLP-1 medications are versions of semaglutide or tirzepatide prepared by compounding pharmacies. They are not FDA-approved as finished products. The FDA states that unapproved compounded GLP-1 versions “do not go through FDA review for safety, effectiveness, and quality” and should generally only be used when “a patient's medical need cannot be met by an FDA-approved drug.”
In February and March 2026, the FDA issued warning letters to more than 30 telehealth companies for marketing violations related to compounded GLP-1 products — specifically for language implying FDA approval or describing compounded products as equivalent to brand-name drugs.
What this means for you: The clinical trial data throughout this page was generated using brand-name FDA-approved medications. If blood pressure and cardiovascular protection are your primary concerns, starting with the FDA-approved pathway gives you the closest match to the published evidence. If cost is the barrier, note that FDA-approved options now start at $199/month (Wegovy titration) and $299/month (Zepbound 2.5 mg).
How fast do GLP-1 medications lower blood pressure?
Blood pressure typically begins declining within 2 to 4 weeks of starting a GLP-1. Here's the timeline from clinical data:
Weeks 1–4
Initial BP reduction begins. The dominant direction across all major trials is sustained BP reduction from week one onward.
Weeks 4–24
The most rapid decline, driven by accelerating weight loss and natriuretic effects reaching steady state.
Weeks 24–72
Blood pressure stabilizes at a new, lower baseline. In SURMOUNT-1, tirzepatide's BP effect plateaued around week 24 and remained stable through week 72. The effect was consistent day and night.
If you stop
Blood pressure tends to return toward baseline as weight is regained.
How we ranked the best GLP-1 for high blood pressure
Our criteria, in order of priority:
- Direct BP reduction data — systolic BP reduction in randomized controlled trials
- Cardiovascular outcomes evidence — demonstrated reduction in heart attacks, strokes, or CV death
- Weight loss efficacy — drives ~70% of the BP effect
- Diabetes, CKD, and sleep apnea fit — relevant comorbidity benefits
- Safety boundaries — contraindications, heart rate, GI tolerability
- Real-world access — self-pay pricing, insurance, formulations
We did not use advertising relationships, commission rates, or provider partnerships as ranking factors. Every data point is sourced to a specific trial or meta-analysis cited on this page.
Frequently asked questions
Which GLP-1 lowers blood pressure the most?↓
Is Zepbound or Wegovy better for high blood pressure?↓
Does Ozempic lower blood pressure?↓
Can GLP-1 drugs replace blood pressure medication?↓
Do GLP-1 medications increase heart rate?↓
How long until a GLP-1 lowers blood pressure?↓
Can GLP-1 medications help resistant hypertension?↓
What if I want a pill instead of a shot?↓
What if I have chronic kidney disease too?↓
Who should NOT use a GLP-1 for blood pressure?↓
Still not sure which GLP-1 program is right for you?
Our free 60-second matching quiz narrows your best-fit path based on blood pressure, heart history, diabetes, kidney health, sleep apnea, and budget.
Related Guides
The RX Index is an independent comparison resource for GLP-1 telehealth providers. This page contains affiliate links — if you use them, we may earn a commission at no additional cost to you. This never influences our rankings or recommendations, which are based on published clinical evidence. This content is for informational purposes only and does not constitute medical advice. Always consult your healthcare provider before starting or changing any medication. Provider pricing and availability subject to change — verify directly before enrolling.