Written by The RX Index Editorial Team · Prices verified March 28, 2026 · Sources: Obesity, The Lancet, FDA, The Menopause Society, RAND · Editorial standards · Updated monthly
GLP-1 FOR PERIMENOPAUSE — 2026 COMPLETE GUIDE
Best GLP-1 for Perimenopause
You're eating the same. Moving the same. And your body is changing anyway — especially around the middle. This isn't a willpower problem. Hormonal changes are a major driver, and the research is finally catching up to what you've been living.
Here's the bottom line: No GLP-1 is FDA-approved specifically for perimenopause — these medications are approved for chronic weight management in eligible adults. But the clinical data shows they work just as well during perimenopause as at any other life stage. For most eligible women whose main goal is maximum weight loss and waist reduction, tirzepatide (Zepbound) is the strongest option — perimenopausal women in the SURMOUNT trials lost approximately 23% of body weight, virtually identical to premenopausal women.
But there's more to this decision than just the drug. Which program you choose matters just as much — especially during perimenopause, when hormones, metabolism, birth control, and bone density are all shifting simultaneously. We'll walk through all of it.
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
QUICK REFERENCE — FIND YOUR FIT
| Your situation | Best pick | Why | Est. month-1 cost (cash) |
|---|---|---|---|
| Maximum weight loss + waist reduction | Zepbound (tirzepatide) | Dual GLP-1/GIP mechanism; ~20–23% weight loss in trials | ~$344 (Ro membership + Zepbound vial) |
| Longer track record or established heart disease | Wegovy (semaglutide) | FDA CV-risk-reduction indication; 15+ years of GLP-1 safety data | ~$194 (Ro membership + Wegovy pill) |
| Need HRT + menopause care + weight help | Midi | Menopause-specialist clinicians who coordinate GLP-1 + HRT | ~$416 (visit + medication + shipping) |
| Want FDA-approved + insurance support | Ro | Insurance concierge handles prior authorizations; brand-name Wegovy and Zepbound | From $45 first month (membership; medication separate) |
| Still on oral birth control | Talk to a clinician first | Zepbound can reduce oral contraceptive effectiveness for 4 weeks after dose changes | — |
| Want a women-focused FDA-approved alternative | Hers | Women-branded platform with Wegovy access | ~$188 (Hers membership + Wegovy pill) |
All costs are self-pay/cash estimates. If your insurance covers GLP-1 medications, your out-of-pocket cost may be significantly lower.
What Is the Best GLP-1 for Perimenopause?
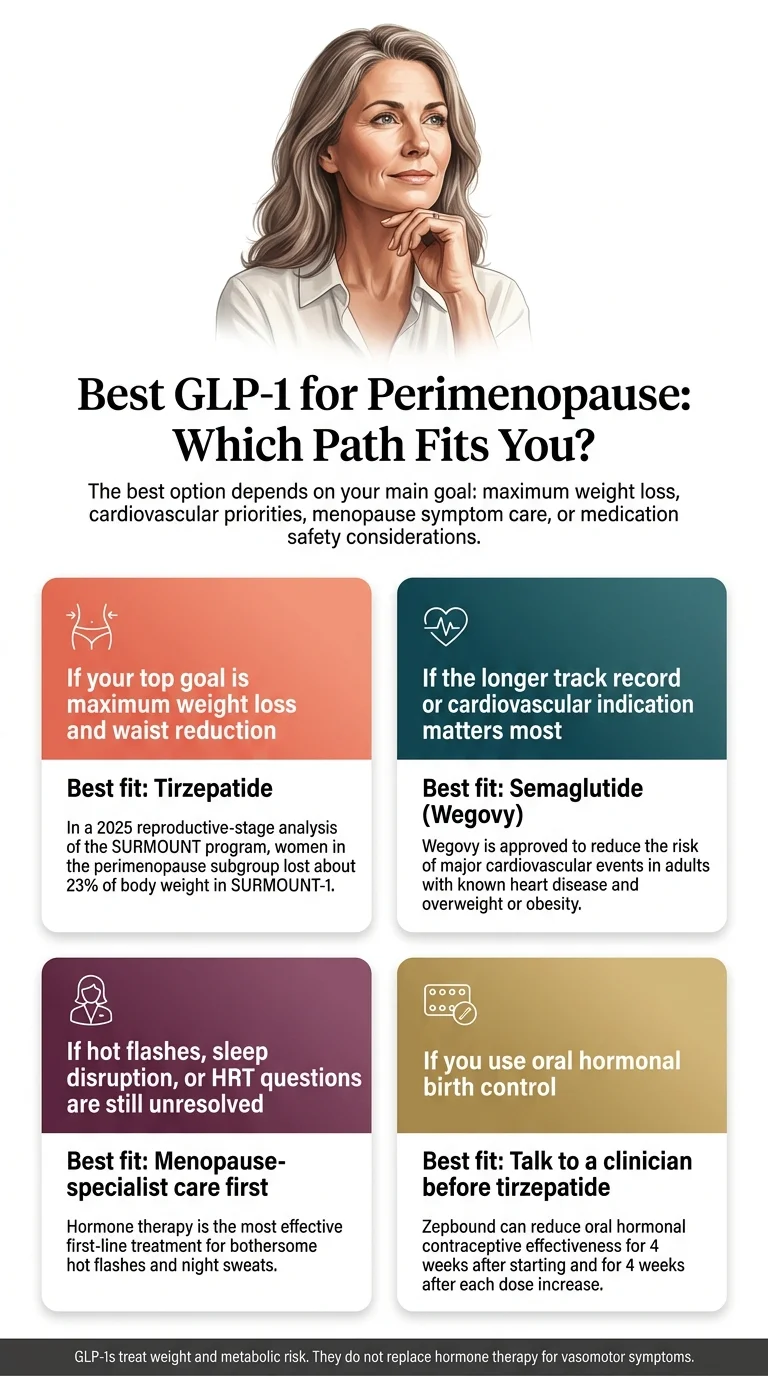
For most eligible women in perimenopause whose main goal is weight loss and waist reduction, tirzepatide (Zepbound) is the strongest option. In the SURMOUNT program's post hoc analysis, perimenopausal women on tirzepatide lost approximately 23% of body weight — virtually identical to premenopausal women.
If you have established cardiovascular disease and want a medication with an FDA cardiovascular-risk-reduction indication, semaglutide (Wegovy) has the edge.
And if hot flashes, night sweats, or HRT questions are still your bigger concern, the best first step is a menopause-specialist clinician — not a weight-loss prescription. HRT remains the standard treatment for vasomotor symptoms.
Why Perimenopause Changes the Weight Loss Equation (And Why It's Not Your Fault)
During perimenopause — typically starting in your 40s and lasting anywhere from 4 to 8 years — your estrogen levels don't just drop. They fluctuate wildly. And that fluctuation triggers a cascade of metabolic changes that make weight management fundamentally harder than it was even a few years ago.
Your metabolism slows down.
By your 50s, you may need about 200 fewer calories a day than you did in your 30s and 40s just to maintain the same weight. That's roughly the equivalent of a daily snack — gone, without changing anything about your habits.
Your body redistributes fat.
Declining estrogen shifts fat storage from your hips and thighs to your abdomen. This visceral fat wraps around your organs and drives up risk for type 2 diabetes, cardiovascular disease, and fatty liver. It's not cosmetic — it's metabolic.
Insulin resistance increases.
As estrogen declines, your cells become less responsive to insulin. Your body stays in “storage mode” instead of “burn mode.” Blood sugar becomes unstable. Cravings intensify.
You lose muscle.
Perimenopause accelerates sarcopenia — the natural age-related loss of muscle mass. Less muscle means a slower metabolism, which means the weight problem compounds itself.
“Food noise” intensifies.
If you've never heard the term, it describes the constant, intrusive mental chatter about food — what to eat, when to eat, whether you've eaten too much, what you'll eat next. Many perimenopausal women describe this as one of the most maddening symptoms. Many patients report that GLP-1 medications significantly reduce this, though individual experience varies.
A 2025 RAND survey found that women aged 50 to 64 had the highest GLP-1 usage of any demographic — 20% reported current or past use. If any of that sounds familiar, here's what matters most: you are not failing. Your physiology changed. Your tools need to change too.
Do GLP-1s Actually Work for Perimenopause Weight Gain?
Yes — and the clinical evidence supporting their use in this population is stronger than most people realize. The biggest concern women have is: “Will this work for hormonal weight gain, or is my body too different for these drugs?” The answer, based on the best available evidence, is clear.
The SURMOUNT Trial Data
In 2025, researchers from NewYork-Presbyterian and Weill Cornell Medicine published a post hoc analysis of the SURMOUNT clinical trials — the landmark studies for tirzepatide — specifically examining outcomes by reproductive stage: premenopausal, perimenopausal, and postmenopausal.
Tirzepatide produced approximately 20–23% body weight reduction in perimenopausal women — virtually identical to results in premenopausal women. Waist circumference dropped by roughly 20 cm across all reproductive stages.
Between 30% and 52% of women with a starting BMI under 35 reached optimal waist-to-height ratio on tirzepatide. The study's lead author, Dr. Beverly Tchang, stated that clinicians can feel confident recommending these medications to patients with menopause-related weight gain.
Early HRT + GLP-1 Evidence
This is where the research gets particularly interesting for perimenopausal women.
A January 2026 Mayo Clinic study published in The Lancet found that postmenopausal women using both hormone therapy and tirzepatide lost approximately 35% more weight than women on tirzepatide alone in a retrospective cohort analysis. An earlier retrospective study found a similar pattern — women combining HRT with semaglutide lost about 30% more weight than those on semaglutide without HRT.
The proposed mechanism: preclinical data suggest that estrogen may enhance the appetite-suppressing effects of GLP-1. HRT may also improve sleep, boost mood, and increase the likelihood of staying active — all factors in sustainable weight loss.
Important context: These are observational studies, not randomized controlled trials. Randomized trials are underway. The evidence is promising and clinically meaningful, but not yet definitive.
The Research Summary
A 2025 peer-reviewed review concluded that GLP-1 receptor agonists are the most effective pharmacologic option for weight loss and can be a valuable tool for peri- and postmenopausal women — while noting that more research is needed on ideal use and long-term risk-benefit profiles in this specific population. The evidence supports using GLP-1s during perimenopause. The key question is which drug and which care path fit your situation best.
Does this sound like what you've been looking for?
Ro offers FDA-approved Wegovy and Zepbound with insurance concierge support and verified cash-pay pricing.
See If You're Eligible on Ro →Tirzepatide vs. Semaglutide for Perimenopause: Which One Should You Choose?
This is the core drug decision, and it's worth getting right.
| Factor | Zepbound (tirzepatide) | Wegovy (semaglutide) |
|---|---|---|
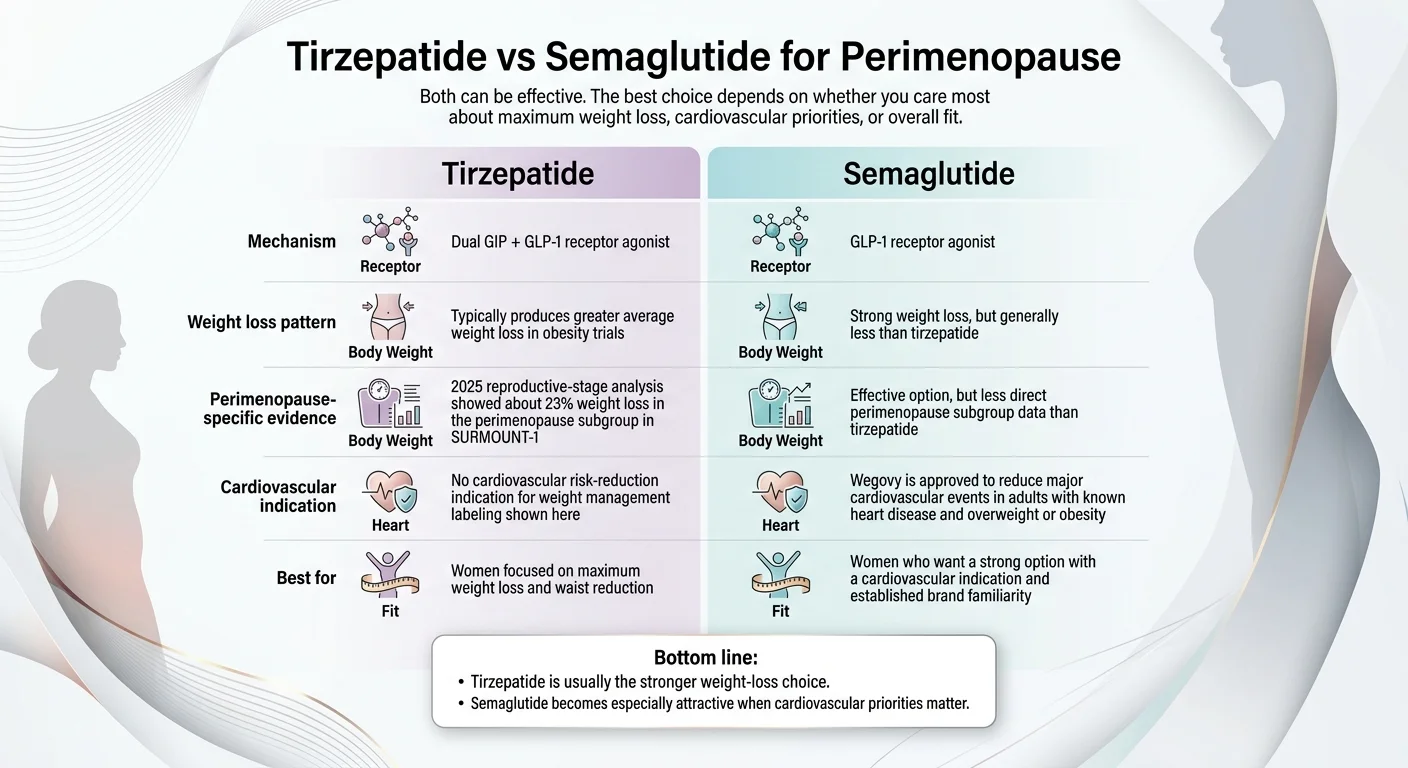
| How it works | Dual GLP-1 + GIP receptor agonist | GLP-1 receptor agonist only |
| Avg. weight loss (trials) | ~20–22% of body weight | ~15% of body weight |
| Perimenopause evidence | SURMOUNT subgroup: ~23% in perimenopausal women | Effective across menopausal stages; less perimenopause-specific subgroup data |
| HRT combination data | Retrospective: ~35% more weight loss with HRT | Retrospective: ~30% more weight loss with HRT |
| Insulin resistance impact | Stronger (dual mechanism) | Strong |
| CV-risk-reduction indication | Not yet | Yes — for adults with established heart disease + overweight/obesity |
| FDA-approved for weight loss | Yes (as Zepbound) | Yes (as Wegovy) |
| Oral option | Not yet available | Yes — Wegovy pill is the only FDA-approved weight-loss GLP-1 available as a pill |
| Insurance coverage (2026) | Growing but still variable | More widely covered |
| Common side effects | GI (nausea, constipation, diarrhea) — generally mild, improve with time | Similar GI profile |
Mounjaro is the diabetes brand for tirzepatide; Ozempic is the diabetes brand for semaglutide. This page uses the weight-management brand names — Zepbound and Wegovy — because that's the relevant indication.
When Zepbound Wins
Choose Zepbound when your primary goal is maximum weight and waist reduction — and especially if insulin resistance is a significant factor. In a head-to-head trial (SURMOUNT-5), tirzepatide outperformed semaglutide for both weight loss and waist reduction. The dual-action mechanism — targeting both GLP-1 and GIP receptors — appears particularly well-suited for the metabolic disruption that occurs during perimenopause, when insulin resistance worsens and visceral fat accumulates.
When Wegovy Wins
Choose Wegovy when you want the longer safety track record, when cardiovascular risk reduction matters, or when insurance coverage is the deciding factor. Wegovy carries an FDA cardiovascular-risk-reduction indication for adults with established heart disease and overweight/obesity. It has broader insurance coverage in 2026 and is the only FDA-approved weight-loss GLP-1 available as a daily pill — a real consideration if you prefer oral medication over weekly injections.
Our Take
For most perimenopausal women, Zepbound is the stronger pharmacologic choice when cost and access aren't barriers. But Wegovy is excellent, more accessible, and has cardiovascular benefits that matter as you age. You genuinely cannot go wrong with either. The real question isn't which drug is 5% better in a clinical trial. It's which path gets you started, keeps you going, and fits your life.
Compare current Zepbound and Wegovy options through Ro's insurance concierge — one platform covers both.
Compare Options on Ro →Best GLP-1 by Your Situation
This is where generic advice fails. Your best GLP-1 path depends on factors most pages never address. Find yourself below.
If your main goal is maximum weight loss and waist reduction
Pick: Zepbound (tirzepatide)
The SURMOUNT trial data is clear — tirzepatide produces the largest reductions in both body weight and waist circumference across all reproductive stages. For perimenopausal women dealing with the specific pattern of visceral fat accumulation driven by declining estrogen and rising insulin resistance, tirzepatide's dual mechanism is the closest pharmacologic match to what's actually happening in your body.
If you have established cardiovascular disease
Pick: Wegovy (semaglutide)
Wegovy has FDA approval for both chronic weight management and cardiovascular risk reduction in adults with established heart disease and overweight/obesity. If cardiovascular risk is a primary concern, semaglutide's outcome data from the SELECT trial gives it a meaningful edge.
If you still need HRT or symptom help alongside weight care
Pick: Midi — menopause-specialist care first
If hot flashes, sleep disruption, brain fog, or hormone questions are still unresolved, the best program isn't the cheapest telehealth prescriber. It's the one that can manage menopause and weight together.
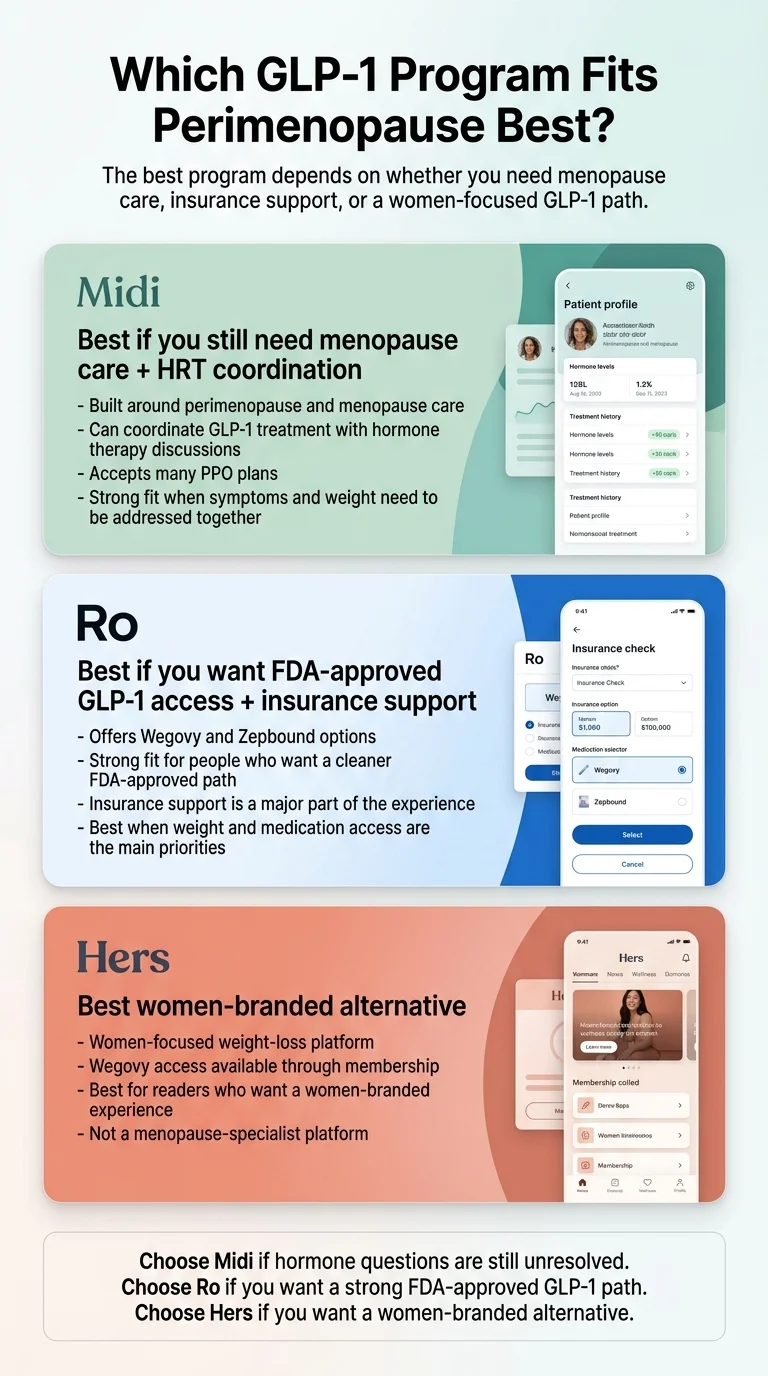
Midi is a menopause-specialist platform available in all 50 states. Their clinicians can evaluate whether HRT, a GLP-1, or both make sense — and coordinate them under one care team. Given the early evidence showing HRT may enhance GLP-1 results, having a clinician who understands both is a real clinical advantage.
If you're cost-conscious and paying cash
Pick: Start with the Wegovy pill through Ro
The Wegovy pill starts at $149/month at the lowest doses — among the most competitive FDA-approved GLP-1 entry points available in 2026. Add Ro's $45 first-month membership ($145/month after), and you have a legitimate, FDA-approved starting point for under $200 in month one.
If you still take oral birth control
Pick: Talk to a clinician before starting Zepbound
This is a section most pages completely ignore, but it matters during perimenopause — a time when pregnancy is still possible.
Birth control warning — tirzepatide only
Zepbound's prescribing information includes a specific warning: oral birth control pills may be less effective for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase. Tirzepatide slows gastric emptying, which can reduce absorption of oral medications — including the pill.
If you rely on oral contraception, discuss backup contraception or a switch to non-oral methods (IUD, patch, ring) with your clinician before starting. Semaglutide does not carry the same specific labeled warning, though any GLP-1 that slows gastric emptying warrants a conversation about oral medication absorption.
And one more thing: HRT is not contraception. During perimenopause, pregnancy is possible until you've gone a full 12 consecutive months without a period.
Best GLP-1 Programs for Perimenopausal Women (Compared)
We evaluated programs on five criteria specific to perimenopause: clinical quality, menopause-specialist access, HRT coordination capability, pricing transparency, and whether they offer FDA-approved medications. We deliberately kept this list short. You don't need 15 options. You need the 3 that actually matter for your situation.
Midi — Best for Perimenopause Care + GLP-1 + HRT Together
Best for: Women who need menopause symptom management and weight care under one roof.
Midi was built for this exact moment in a woman's life. Their clinicians specialize in perimenopause and menopause — not general weight loss — which means they can evaluate your full hormonal picture, not just your BMI. They can prescribe HRT, GLP-1 medications, or both, and coordinate them together.
| Platform fee | PPO accepted; self-pay: $250 initial, $150 follow-up |
| Compounded GLP-1 (not FDA-approved) | From $127.90/mo + $38 refrigerated shipping |
| Coverage | Accepts many PPO plans nationwide |
| Availability | All 50 states |
| HRT coordination | Yes — same clinical team |
What we like: Midi is the only program here that can genuinely function as your menopause care home. If you're juggling hot flashes, sleep issues, mood changes, and weight gain, having one clinical team that sees the whole picture is worth more than saving $30/month on a prescription.
“My clinician is amazing. She prescribed me a GLP-1 for weight loss and HRT. I've lost 20 pounds.” — Midi patient
The honest limitation: Midi is not the fastest “ship me medication tomorrow” option. If you already know exactly what you want and just need a prescription filled, Ro is more streamlined. But for women whose hormone picture is complicated — and whose weight gain is inseparable from their perimenopause — Midi's integrated care team is the right tradeoff.
Check Coverage and Availability with Midi →Ro — Best for FDA-Approved GLP-1s + Insurance Support
Best for: Women who want brand-name Wegovy or Zepbound, insurance concierge, and the cleanest FDA-approved path.
Ro is our top recommendation for straightforward FDA-approved GLP-1 access. Their insurance concierge handles prior authorizations — the single biggest barrier to getting brand-name GLP-1s covered — and they've partnered with Novo Nordisk (for Wegovy) and Eli Lilly (for Zepbound) to offer competitive verified cash-pay prices when insurance doesn't cover it.
| Membership — first month | $45 |
| Membership — ongoing | $145/month |
| Wegovy pill (cash, starting dose) | From $149/month |
| Wegovy pen (cash, first 2 months) | $199/month (through Mar 31, 2026) |
| Wegovy pen (cash, higher doses) | $349/month |
| Zepbound vials (cash, starting dose) | From $299/month |
| Zepbound vials (cash, higher doses) | $449/month with manufacturer offer |
Medication costs are separate from membership. If insured, your cost will be a copay determined by your plan.
What we like: Ro provides monthly provider check-ins, unlimited messaging with your care team, and insurance concierge at no extra charge. Many women describe the “food noise” quieting down — the constant mental chatter about eating finally becoming manageable. For women in perimenopause who've been battling escalating cravings for months or years, that mental shift is often described as the most transformative part.
The honest limitation: Ro is not a menopause specialist. They won't prescribe HRT, evaluate your estrogen levels, or help you sort out whether hot flashes should be treated before or alongside weight loss. If your hormone picture is complicated, start with Midi or your own menopause-informed clinician. But if weight and metabolic health are your primary concerns and you want the most reliable path to FDA-approved GLP-1 medication with genuine insurance support, Ro is the clear winner.
See Ro Pricing and Check Eligibility →Hers — Best Women-Branded FDA-Approved Alternative
Best for: Women who want a women-focused platform and FDA-approved GLP-1 access with a lower first-month membership.
Hers has positioned itself as a women's health platform that includes weight management. Their membership starts at $39 for the first month ($149/month ongoing — slightly higher than Ro's $145/month), and they offer Wegovy starting at $149/month for the pill. Hers is not a perimenopause specialist any more than Ro is. Consider it if you prefer the women-branded experience, but it's not a substitute for menopause-specific care.
Compare Hers Pricing →A note on compounded GLP-1 providers
We intentionally did not feature a compounded-first provider as a primary pick for this page. The FDA resolved the semaglutide shortage in February 2025 and the tirzepatide shortage in late 2024. In March 2026, the FDA issued approximately 30 warning letters to telehealth companies over false or misleading compounded GLP-1 marketing. For this audience — perimenopausal women dealing with bodies already in flux — we believe the FDA-approved path is the stronger starting recommendation. The price gap has narrowed significantly in 2026.
Can You Take a GLP-1 and HRT Together?
Yes — and for many perimenopausal women, early evidence suggests the combination may produce better weight-loss outcomes than GLP-1 alone.
Observational data is consistent: retrospective studies show stronger weight-loss results in women using both hormone therapy and GLP-1 medications. The January 2026 Mayo Clinic study found approximately 35% greater weight loss in the tirzepatide + HRT group. An earlier study showed about 30% greater weight loss with semaglutide + HRT.
The proposed mechanism makes biological sense. HRT addresses the hormonal foundation — restoring estrogen, improving sleep, stabilizing mood, and supporting muscle preservation. GLP-1s address the metabolic disruption — reducing appetite, improving insulin sensitivity, and targeting visceral fat. They work on different but complementary pathways.
One clinical nuance most pages miss
The British Menopause Society's 2025 guidance on incretin-based therapies notes that if a woman is using oral estrogen-based HRT, switching to transdermal estrogen (patch or gel) may need discussion. GLP-1s slow gastric emptying, which could affect absorption of oral medications — including oral progestogen and oral estrogen. This is the kind of detail a menopause-specialist clinician can navigate. A general telehealth prescriber may not catch it.
If you're in perimenopause and considering a GLP-1, the question of HRT should be part of the same conversation, not a separate one.
Need a clinician who can coordinate both GLP-1 and HRT? Midi's menopause-specialist team handles exactly this.
Check Midi Availability →What GLP-1s Will — and Will Not — Fix in Perimenopause
We're going to be straight with you because you deserve accuracy, not hype.
GLP-1s will likely help with:
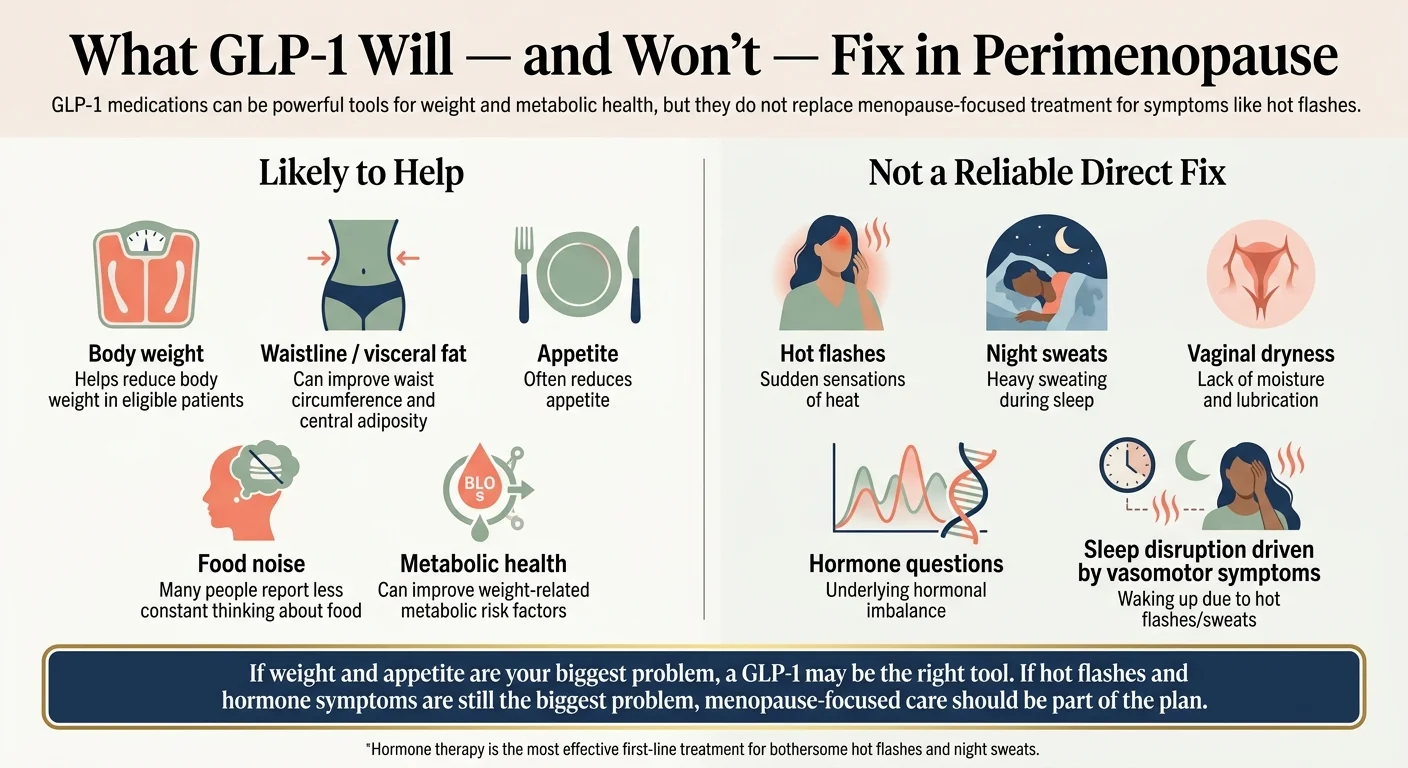
- ✓Weight loss (15–22% of body weight in clinical trials, regardless of menopausal status)
- ✓Waist circumference reduction and visceral fat loss
- ✓Appetite reduction and “food noise” — the constant mental chatter about food
- ✓Insulin sensitivity improvement
- ✓Metabolic markers: blood sugar, blood pressure, cholesterol
- ✓Cardiovascular risk (Wegovy specifically carries an FDA indication for eligible adults)
- ✓The feeling of “being stuck” — many women describe their body finally responding again
GLP-1s will NOT reliably fix:
- ✗Hot flashes and night sweats (HRT is the standard treatment)
- ✗Vaginal dryness or genitourinary symptoms
- ✗Brain fog (some women report improvement, but not an established benefit)
- ✗Mood swings and anxiety (mixed data — not guaranteed)
- ✗Sleep disturbance driven by vasomotor symptoms
The honest reframe: If your biggest pain is 2 a.m. hot flashes, drenching night sweats, and mood disruption — start with menopause care. HRT is the evidence-based first-line treatment for vasomotor symptoms, and it may also set the stage for better GLP-1 results down the road.
If your biggest pain is the scale, the waistline, the cravings, and the metabolic shift that came with perimenopause — a GLP-1 is the most effective pharmacologic tool available for weight management, and the evidence specifically supports its use in your demographic.
Side Effects, Muscle Loss, and Hair: What Perimenopausal Women Need to Know
GLP-1s have a well-characterized side effect profile, and most effects are manageable. But perimenopause adds specific considerations.
Standard GI Side Effects
Nausea, constipation, diarrhea, and reduced appetite are the most common. They're typically worst when you first start or when your dose increases, and they generally improve within a few weeks. Slow dose titration — starting low and increasing gradually — significantly reduces severity.
Practical tips: eat slowly, choose smaller meals, increase fiber gradually, stay hydrated even when you don't feel thirsty (GLP-1s can blunt thirst signals), and avoid carbonated beverages.
The Muscle Loss Problem
This is the concern most specific to perimenopausal women, and it's legitimate. GLP-1s cause weight loss of both fat and muscle. During perimenopause, you're already losing muscle mass due to declining estrogen and age-related sarcopenia. The compounding effect is real: losing muscle while on a GLP-1 can leave you thinner but metabolically weaker — and more vulnerable to frailty as you age.
The mitigation protocol — supported by menopause and obesity specialists:
- •Protein: Aim for about 1.0–1.2 grams per kilogram of body weight per day — the range recommended by The Menopause Society for preserving muscle mass in midlife. Many perimenopausal women are under-eating protein, and GLP-1s can further reduce appetite. Make every meal count.
- •Resistance training: At least 2–3 sessions per week. This is not optional during GLP-1 treatment in perimenopause. It is the single most protective action you can take.
- •HRT consideration: The retrospective data suggests HRT may help preserve lean mass during weight loss. Another reason the GLP-1 + HRT conversation should happen together.
Hair Thinning
Many perimenopausal women already notice hair changes from declining estrogen and progesterone. Rapid weight loss from any cause — including GLP-1s — can trigger additional hair shedding (telogen effluvium). This is usually temporary and reverses as your body adjusts, but it can be distressing.
Ensure adequate iron, B vitamins, zinc, and protein. If hair loss is significant or persistent, consult a dermatologist. This is a manageable side effect, not a reason to avoid treatment — but it's worth knowing about in advance.
Who Should Not Use GLP-1s
Contraindications
- Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2)
- History of pancreatitis — discuss the risks carefully with your clinician
- Pregnancy or planned pregnancy: Wegovy's label requires stopping at least 2 months before a planned pregnancy; Zepbound's label warns it may harm an unborn baby
During perimenopause, pregnancy is still possible until you have completed a full year without a period. If you're on a GLP-1 and not using reliable contraception, discuss this with your provider.
FDA-Approved vs. Compounded GLP-1s in 2026: What Changed
The landscape shifted significantly, and what was true in 2024 may not be true now.
- →The shortages ended. The FDA resolved the semaglutide shortage in February 2025. The tirzepatide shortage ended in late 2024.
- →FDA enforcement increased. In February 2026, the FDA announced new action against non-FDA-approved GLP-1 drugs. In March 2026, the agency issued approximately 30 warning letters to telehealth companies over false or misleading compounded GLP-1 marketing.
- →The price gap has narrowed. With the Wegovy pill at $149/month and manufacturer cash-pay programs through Ro, the cost argument for compounded options is weaker than it was in 2023 or 2024.
Compounded GLP-1s still exist and some are legitimate. But if you choose a compounded route, verify: Is the pharmacy licensed and inspectable? Who actually compounds the medication? And does the company clearly state that compounded medications are not FDA-approved?
For most perimenopausal women making this decision in 2026, FDA-approved medications through verified programs are the cleaner path.
See FDA-Approved Options on Ro →Real Cost in 2026: What You'll Actually Pay
Price is often the deciding factor. Here's what the numbers look like, verified as of late March 2026.
| Program | Platform fee | Medication starting price (cash) | Best for |
|---|---|---|---|
| Ro | $45 first month, then $145/mo | Wegovy pill from $149/mo; Zepbound vials from $299/mo | FDA-approved + insurance support |
| Midi | PPO accepted; self-pay $250 initial visit | Compounded GLP-1 from $127.90/mo + $38 shipping (not FDA-approved) | Menopause care + GLP-1 + HRT |
| Hers | $39 first month, then $149/mo | Wegovy pill from $149/mo | Women-branded FDA-approved |
| Your own doctor | Your copay | Varies by plan and prior authorization | Strong insurance coverage |
What most pages don't tell you
The advertised starting price is almost never the long-term price. Doses increase over time, and higher doses cost more. Budget for the 3–6 month price, not just month one.
Estimated 12-month projections (self-pay, standard dose titration):
- •Ro + Wegovy pill: Roughly $4,000–$5,500 total over 12 months
- •Ro + Zepbound vials: Roughly $5,500–$7,000 total over 12 months
- •Ro + insurance: If covered, your cost could drop to your copay ($25–$100/month typical) plus $145/month membership — potentially $2,000–$3,000/year total
- •Midi (compounded, self-pay): Roughly $2,500–$4,000 total over 12 months including visits
These are modeled estimates based on published pricing and standard titration schedules. Your actual cost will depend on your dose, insurance coverage, manufacturer offers active at the time, and whether you pause or adjust treatment.
Time-sensitive pricing notes
Ro's Wegovy pen intro pricing ($199/month for months 1–2) is listed as valid through March 31, 2026. Lower-dose Wegovy pill pricing at $149/month runs through April 15, 2026. We update this page when pricing changes.
HSA/FSA: GLP-1 medications may be eligible for HSA or FSA reimbursement when prescribed to treat a diagnosed medical condition such as obesity. Check your plan's specific rules.
See your pricing options on Ro before current offers expire.
See Ro Pricing →What Happens If You Stop
Stopping GLP-1 medication often leads to weight regain. Post-study data from tirzepatide trials showed that participants who discontinued regained a significant portion of the weight they'd lost, along with worsening of cardiometabolic markers. The Menopause Society notes that anti-obesity medications generally require long-term use because discontinuation frequently leads to regain.
The part that matters most for perimenopausal women: the weight that returns tends to come back as fat rather than muscle. That means stopping without a plan can leave you with worse body composition than when you started.
This is not a reason to avoid GLP-1s. It's a reason to choose a program designed for the long haul and to build sustainable habits while the medication gives you a runway.
- →Commit to resistance training and protein from day one, not as an afterthought
- →Choose a program that supports maintenance dosing, not just starter pricing
- →Build the habits — sleep, stress management, whole-food nutrition — that the medication makes easier to establish
- →Discuss long-term strategy with your provider — some women stay on a maintenance dose indefinitely; others taper; some transition off after building a strong lifestyle foundation
Many women find that this reframe takes the pressure off. You're not “cheating” by using medication. You're using a clinically validated tool to create a window — a period of reduced appetite and improved metabolic function — during which you can build the habits, muscle mass, and lifestyle foundation that will serve you for decades. The medication makes the hard things easier. The habits you build while on it are what last.
How We Evaluated These Options
Drug evaluation
We reviewed the SURMOUNT program's post hoc analysis by reproductive stage, the January 2026 Mayo Clinic tirzepatide + HRT retrospective cohort study, the RAND American Life Panel survey, the 2025 peer-reviewed evidence review on GLP-1s in peri/postmenopausal women, and official FDA prescribing information for Wegovy and Zepbound.
Program evaluation
We verified live pricing on official provider websites (Ro, Midi, Hers) as of March 28, 2026.
Compliance
We separated FDA-approved from compounded options throughout. We verified every factual claim against published sources.
Affiliate transparency
We may earn a commission if you sign up through our links. This does not affect which programs we recommend, which drug we call the winner, or what we say about limitations. Our methodology is based on clinical evidence and verified pricing, not commission rates.
Update commitment
We re-verify pricing and availability monthly. The last verified date at the top of this page reflects our most recent check.
Frequently Asked Questions
What is the best GLP-1 for perimenopause weight gain?
Zepbound (tirzepatide) is the strongest option for most eligible perimenopausal women when the primary goal is maximum weight loss and waist reduction. The SURMOUNT trials showed approximately 20–23% body weight loss in perimenopausal women. Wegovy (semaglutide) is the better choice if cardiovascular risk reduction or broader insurance coverage is the priority.
Is tirzepatide better than semaglutide for perimenopause?
For weight loss magnitude, yes — tirzepatide produced greater weight loss and waist reduction in head-to-head trials (SURMOUNT-5). Its dual GLP-1/GIP mechanism may be particularly well-suited to the insulin resistance that worsens during perimenopause. However, semaglutide has a longer track record and broader insurance coverage, and Wegovy carries an FDA cardiovascular-risk-reduction indication for adults with established heart disease and overweight/obesity.
Can you take a GLP-1 and HRT at the same time?
Yes, and early observational data suggests the combination may produce better weight-loss outcomes. A 2026 retrospective study found approximately 35% greater weight loss with tirzepatide + HRT versus tirzepatide alone. This should be managed by a clinician familiar with both therapies. If you use oral HRT, discuss potential absorption interactions with your provider — GLP-1s slow gastric emptying, which can affect oral medications.
Will a GLP-1 help hot flashes or mood swings?
Not reliably. GLP-1s are not approved for or specifically effective at treating vasomotor symptoms (hot flashes, night sweats) or mood disturbances. HRT remains the standard treatment for those symptoms. Some women report indirect improvement, but this is not guaranteed.
Can GLP-1s cause hair loss during perimenopause?
Rapid weight loss from any cause can trigger temporary hair shedding (telogen effluvium). Since perimenopause already affects hair due to hormonal changes, the combined effect can be noticeable. Adequate protein, iron, B vitamins, and zinc help. This is usually temporary and resolves as weight stabilizes.
Will GLP-1s cause muscle loss during perimenopause?
GLP-1s cause loss of both fat and muscle. During perimenopause, when muscle mass is already declining due to estrogen changes and sarcopenia, this is a heightened concern. The mitigation strategy: aim for about 1.0–1.2 g of protein per kg of body weight per day, resistance training 2–3 times per week, and discussion of HRT which may help preserve lean mass.
What if I'm still on oral birth control?
This matters specifically for tirzepatide. Zepbound's prescribing information warns that oral contraceptives may be less effective for 4 weeks after starting and 4 weeks after each dose increase. Discuss backup contraception or switching to a non-oral method with your clinician before starting. Note: HRT is not contraception — during perimenopause, pregnancy is possible until you have completed a full year without a period.
Are compounded GLP-1s still safe now that shortages are over?
Compounding pharmacies can still produce GLP-1s under certain conditions, but FDA scrutiny has increased significantly since shortages ended in 2024–2025. In March 2026, the FDA issued approximately 30 warning letters to telehealth companies over false or misleading compounded GLP-1 marketing. If you choose a compounded route, verify the pharmacy's licensing, compounding practices, and shipping protocols. Compounded medications are not FDA-approved.
How fast do GLP-1s work for perimenopause weight loss?
Most women notice appetite changes and some weight loss within the first 2–4 weeks. Clinically meaningful weight loss (5%+ of body weight) typically occurs within 3–6 months. Maximum results are usually seen at 12–18 months. Perimenopause does not appear to slow the timeline based on available SURMOUNT subgroup data.
What happens if I stop taking a GLP-1?
Weight regain is common after discontinuation, and the regained weight tends to be fat rather than muscle — potentially worsening body composition. Most specialists recommend planning for long-term or maintenance-dose therapy. Building sustainable exercise, nutrition, and sleep habits while on the medication provides the best foundation if you eventually taper or discontinue.
Which provider is best if I want insurance to cover my GLP-1?
Ro. Their insurance concierge team handles prior authorization requests at no extra charge, and they work with both Novo Nordisk (Wegovy) and Eli Lilly (Zepbound) to offer verified cash-pay pricing when insurance doesn't cover it.
Which provider is best if I need menopause-specialist care?
Midi. They are the only program reviewed here built specifically for perimenopause and menopause care, with clinicians trained to evaluate hormones, prescribe HRT, and manage GLP-1 treatment together under one care team.
Sources
- The Menopause Society. Midlife Weight Gain. 2025. menopause.org
- Tchang BG, et al. Body weight reduction in women treated with tirzepatide by reproductive stage: a post hoc analysis from the SURMOUNT program. Obesity. 2025;33(5):851–860. PubMed
- Castaneda R, et al. The role of menopause hormone therapy in modulating tirzepatide-associated weight loss in postmenopausal women. The Lancet Obstetrics, Gynaecology, & Women's Health. 2026;2(2):e118–e128. ScienceDirect
- RAND Corporation. GLP-1 Agonists in Perimenopause: Unique Risks and Potential Opportunities. August 2025. rand.org
- Hurtado MD, et al. Weight loss response to semaglutide in postmenopausal women with and without hormone therapy use. Menopause. 2024;31(4):345–352. PubMed
- British Menopause Society. Use of incretin-based therapies in women using hormone replacement therapy (HRT). 2025. thebms.org.uk
- Mikdachi H, Dunsmoor-Su R. GLP-1 receptor agonists for weight loss for perimenopausal and postmenopausal women. Curr Opin Obstet Gynecol. 2025;37(2):97–101. PubMed
- FDA. Clarification on policies for compounders as national GLP-1 supply stabilizes. 2025. fda.gov
- FDA. FDA intends to take action against non-FDA-approved GLP-1 drugs. February 2026. fda.gov
- Wegovy prescribing information. Novo Nordisk. wegovy.com
- Zepbound prescribing information. Eli Lilly. zepbound.lilly.com
- Ro weight loss pricing. Verified March 28, 2026. ro.co/weight-loss/pricing
- Midi Health. Verified March 28, 2026. joinmidi.com
- SURMOUNT-5 trial. Tirzepatide vs semaglutide head-to-head. PubMed
- Mayo Clinic. Menopause weight gain. mayoclinic.org
Still Not Sure Which GLP-1 Program Is Right for You?
You've read the research. You understand the drugs. You know what fits your situation. If you're ready to act, go with what matches your needs. If you have insurance and want FDA-approved medication, Ro is the most straightforward path. If you need menopause care alongside weight management, Midi is built for this moment.
If you're still weighing options — we built a tool for exactly this moment. Take our free 60-second matching quiz. We'll ask about your insurance status, budget, whether you're on or considering HRT, and your primary concern. Then we'll match you with the specific program and medication path that fits your perimenopause situation. No email required. No sales pitch. Just clarity.
Here's what most pages won't say directly: you have already done the hard part. You recognized that something changed. You researched your options. You read a thorough clinical breakdown instead of settling for a listicle. The weight gain wasn't your choice. But what you do about it is.
This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before starting any medication. GLP-1 medications require a prescription and medical evaluation.