GLP-1 MEDICATIONS FOR WOMEN — 2026 GUIDE
Best GLP-1 for Women in 2026: Which Medication Fits Your Body, Budget, and Life Stage?
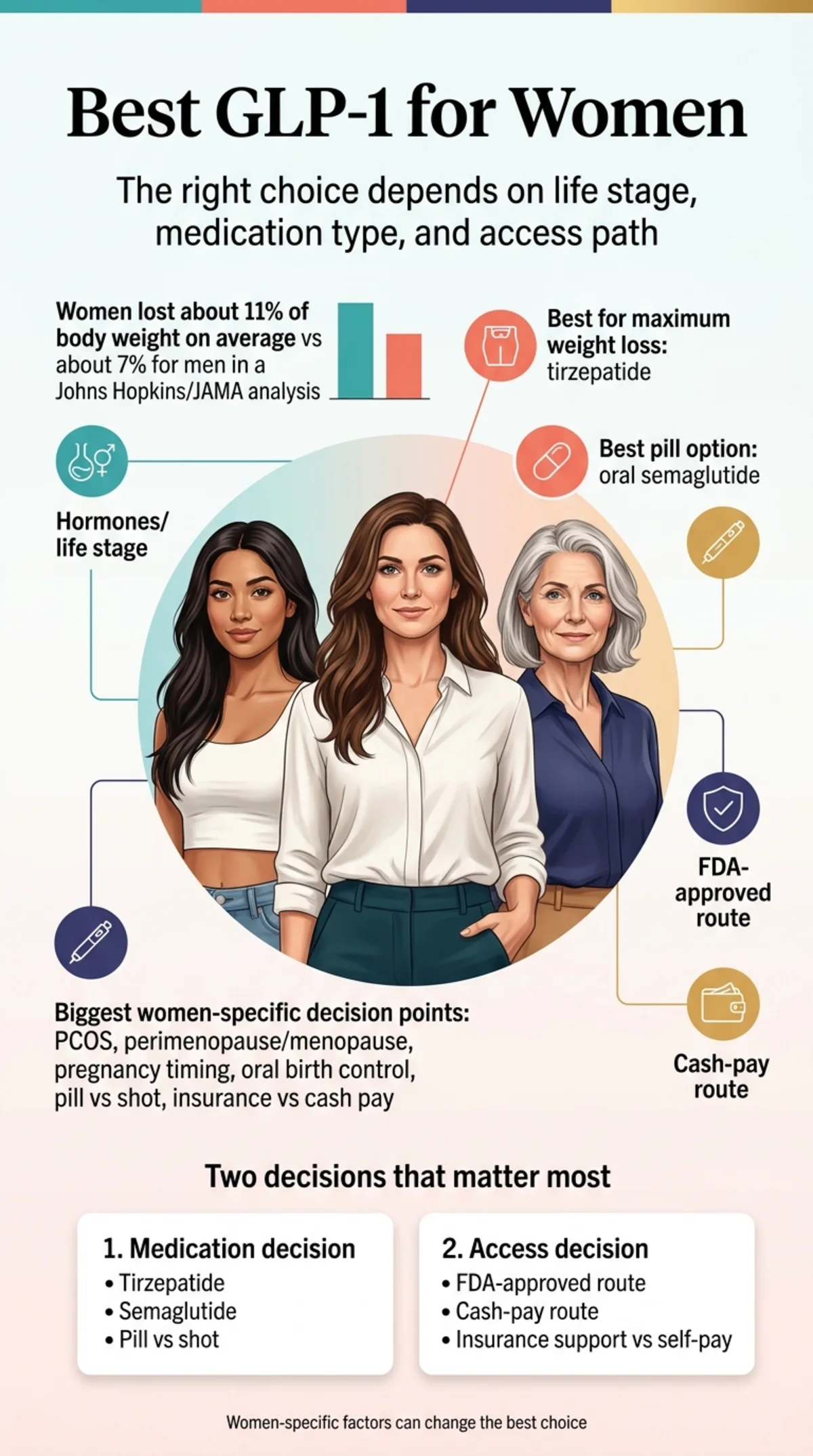
If you're searching for the best GLP-1 for women, here's the short answer — then we'll show you exactly how the right choice changes based on your hormones, your age, and your budget.
In the sex-specific analysis within a 2026 Johns Hopkins / JAMA Internal Medicine meta-analysis, women across six clinical trials lost an average of 10.9% of their body weight, compared to 6.8% for men. That's not a marginal difference. Current evidence suggests women may, on average, lose meaningfully more weight on these medications than men.
But “best GLP-1 for women” depends on two separate decisions most guides lump together:
- Which medication — tirzepatide or semaglutide, injection or pill
- Which access route — FDA-approved with insurance support, or cash-pay
We split those apart below because the right answer for a 44-year-old with PCOS and insurance is completely different from a 58-year-old in menopause paying cash. And both are different from a 32-year-old who may want pregnancy in the next year and doesn't want injections.
By The RX Index Editorial Team · Last updated: March 28, 2026 · Pricing verified: March 27, 2026
Sources: Johns Hopkins / JAMA Internal Medicine 2026 meta-analysis; SURMOUNT trials; STEP trials; FDA prescribing information; British Menopause Society guidelines
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
The Bottom Line — Which Medication Wins?
| Your Situation | Best Medication | Why |
|---|---|---|
| Maximum weight loss | Tirzepatide (Zepbound) | Strongest clinical results — up to 22.5% body weight loss |
| PCOS or insulin resistance | Tirzepatide (Zepbound/Mounjaro) | Dual GLP-1 + GIP mechanism targets insulin resistance directly |
| Menopause or perimenopause | Semaglutide or tirzepatide | Both effective across all reproductive stages |
| Want a pill, not a shot | Wegovy pill (oral semaglutide) | Only FDA-approved daily GLP-1 pill for weight loss |
| Over 50 or 60 | Semaglutide (Wegovy) | Proven cardiovascular protection + longest weight-management track record |
| May want pregnancy soon | Read safety section first → | Timing and washout periods matter — discuss with your OB/GYN |
The Bottom Line — Which Access Route Wins?
| Your Priority | Best Provider | Starting Cost |
|---|---|---|
| FDA-approved + insurance help | Ro | Wegovy pill from ~$194/mo (medication + membership); Zepbound from ~$344/mo |
| Cash-pay, medication included | MEDVi | Semaglutide injections from $179 first mo, $299 refills |
| Women-first pill experience | Hers | Wegovy pill from ~$188/mo (medication + membership) |
Ro membership: $45 first month, then $145/mo. Medication separate. Wegovy pill cash-pay starts at $149/mo for introductory doses via Novo Nordisk offer through Aug 2026. Hers membership: $39 first month, then $149/mo. Medication separate. MEDVi: medication included in price, no separate membership. All pricing verified March 2026.
There is no single GLP-1 that is best for every woman.
The medication with the biggest average weight loss is not automatically the right choice if you're planning pregnancy, rely on oral birth control, need a pill instead of a shot, or can get an FDA-approved option covered by insurance. That's why this page exists.
Do GLP-1 Medications Actually Work Differently for Women?
Yes — and the data is clearer than most people realize.
A March 2026 meta-analysis published in JAMA Internal Medicine, led by Johns Hopkins Bloomberg School of Public Health researchers, analyzed 64 clinical trials involving tens of thousands of patients. In the sex-stratified subset — 19,906 patients across six trials — women lost an average of 10.88% of their starting body weight. Men lost 6.78%. That was a statistically significant difference.
The researchers proposed three possible reasons:
- Estrogen synergy — GLP-1 medications may interact with estrogen in ways that enhance appetite suppression and metabolic effects
- Drug processing differences — Women may metabolize GLP-1 receptor agonists differently than men
- Body weight ratios — Women's lower median body weight means relatively higher drug concentration per dose
Separately, a NewYork-Presbyterian and Weill Cornell Medicine analysis of the SURMOUNT clinical trials found that tirzepatide produced approximately 20% weight reduction in women regardless of reproductive stage — premenopausal, perimenopausal, or postmenopausal.
A Note on Permission
We know many women reading this feel some version of guilt about considering medication for weight loss. You've tried diets. You've tried willpower. You've tried everything your doctor or Instagram suggested.
Here's the medical reality: obesity is a chronic metabolic condition with biological, hormonal, and genetic drivers that dieting alone cannot consistently overcome. GLP-1 medications address those biological mechanisms directly. The same way a person with high blood pressure takes medication and watches their sodium.
No one calls blood pressure medication “cheating.” GLP-1 medications deserve the same framing. The women who have the best outcomes treat these medications as one component of a comprehensive approach — but it's often the component that finally makes the rest of it work.
Which GLP-1 Medication Is Best for Women?
Before we talk about where to get it, let's settle what to get. Wegovy and Zepbound are FDA-approved specifically for chronic weight management. Ozempic and Mounjaro are sometimes prescribed off-label for weight loss.
| Medication | Avg. Loss | Form | Freq. | Women-Specific Note |
|---|---|---|---|---|
| Zepbound Tirzepatide | Up to 22.5% | Injection | Weekly | Can reduce oral contraceptive effectiveness — use backup birth control 4 weeks after starting or dose changes |
| Wegovy (2.4 mg) Semaglutide | ~15% | Injection | Weekly | Longest chronic weight-management track record; FDA-approved for MASH and cardiovascular risk |
| Wegovy HD (7.2 mg) Semaglutide | ~21% | Injection | Weekly | New higher dose approved March 2026; narrows gap with tirzepatide |
| Wegovy pill Oral semaglutide | ~13.6% | Daily pill | Daily | FDA-approved Jan 2026. Not recommended while breastfeeding — pill coating (SNAC) may enter breast milk |
| Mounjaro Tirzepatide | Up to 22.5% | Injection | Weekly | FDA-approved for T2D — same oral contraceptive interaction warning as Zepbound |
| Ozempic Semaglutide 1–2 mg | 10–15% | Injection | Weekly | FDA-approved for T2D — commonly prescribed off-label for weight loss at lower dose than Wegovy |
| Saxenda Liraglutide | 5–8% | Injection | Daily | Older option; generic available 2025; largely being replaced by more effective agents |
Tirzepatide vs. Semaglutide for Women: Which Is Better?
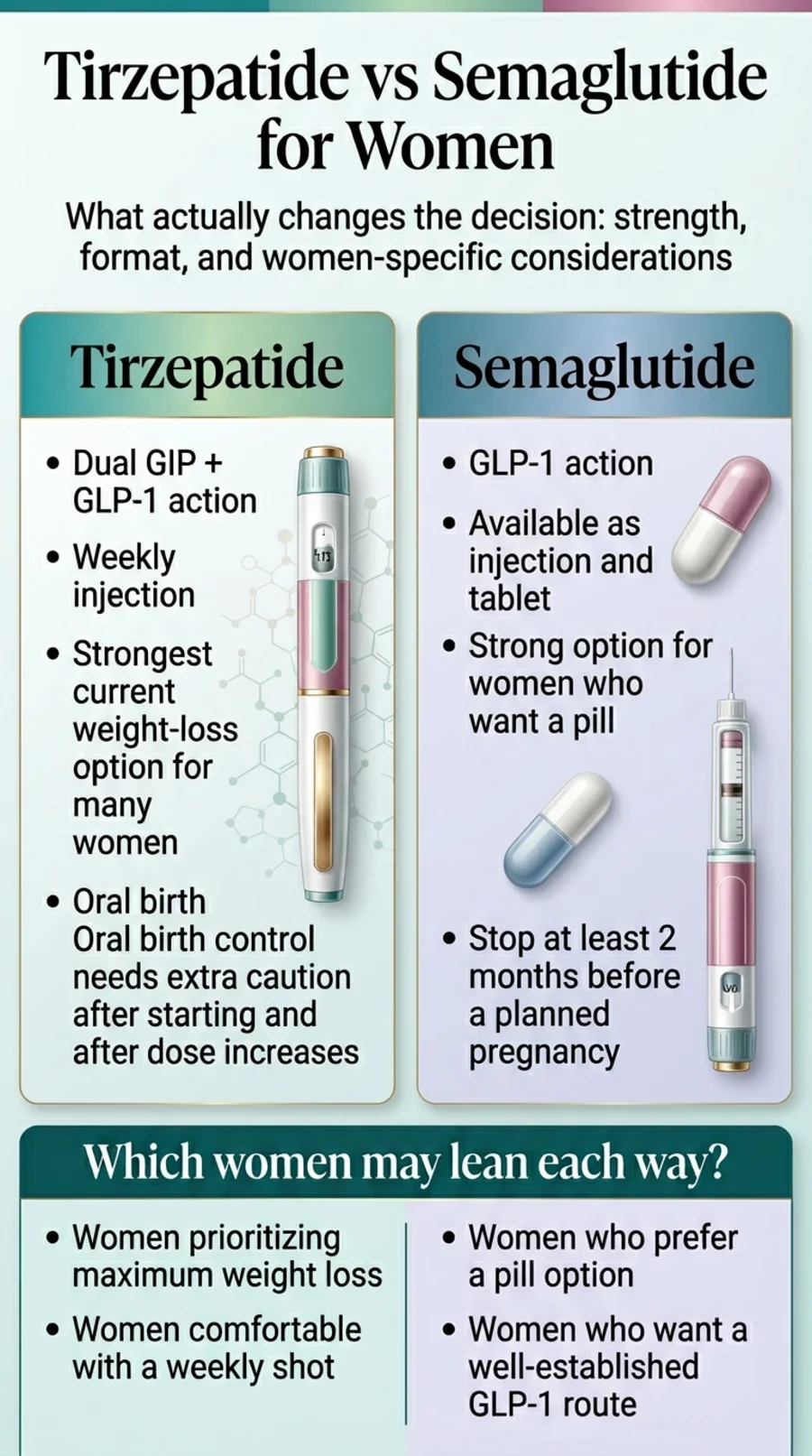
Tirzepatide (Zepbound/Mounjaro) activates two receptors — GLP-1 and GIP — producing stronger appetite suppression and more pronounced metabolic effects. In a 2025 head-to-head trial published in the New England Journal of Medicine, tirzepatide produced significantly greater reductions in body weight and waist circumference over 72 weeks compared to semaglutide at maximum approved doses.
Semaglutide (Wegovy/Ozempic) has a longer chronic weight-management track record, more long-term cardiovascular outcomes data, and is now available as a daily pill. The newer 7.2 mg Wegovy HD dose (approved March 2026) narrows the efficacy gap with tirzepatide considerably, producing approximately 21% weight loss.
Our take
For maximum weight loss, tirzepatide is the strongest current option. For the broadest access — including a daily pill, a longer safety track record, and better insurance coverage — semaglutide (Wegovy) is excellent. Neither is a wrong choice. GI side effects are common with both, particularly during dose escalation, and individual tolerability varies.
What About the Wegovy Pill?

This is a meaningful development for women who've been waiting for a non-injection option. The Wegovy pill (oral semaglutide for weight loss) received FDA approval in December 2025 and launched in January 2026.
You take one pill daily, 30 minutes before eating or drinking anything else. In clinical trials, the pill produced approximately 13.6% body weight loss versus 2% for placebo after 71 weeks. That's somewhat less than injectable Wegovy at maximum dose, but for many women, not having to self-inject weekly is worth that trade-off.
Eli Lilly's oral GLP-1 orforglipron is under FDA review as of March 2026. It's a non-peptide pill that can be taken with food (no 30-minute fasting window), which could change the convenience equation further.
Want to get the Wegovy pill?
GLP-1 Supplements and Patches — Do They Work?
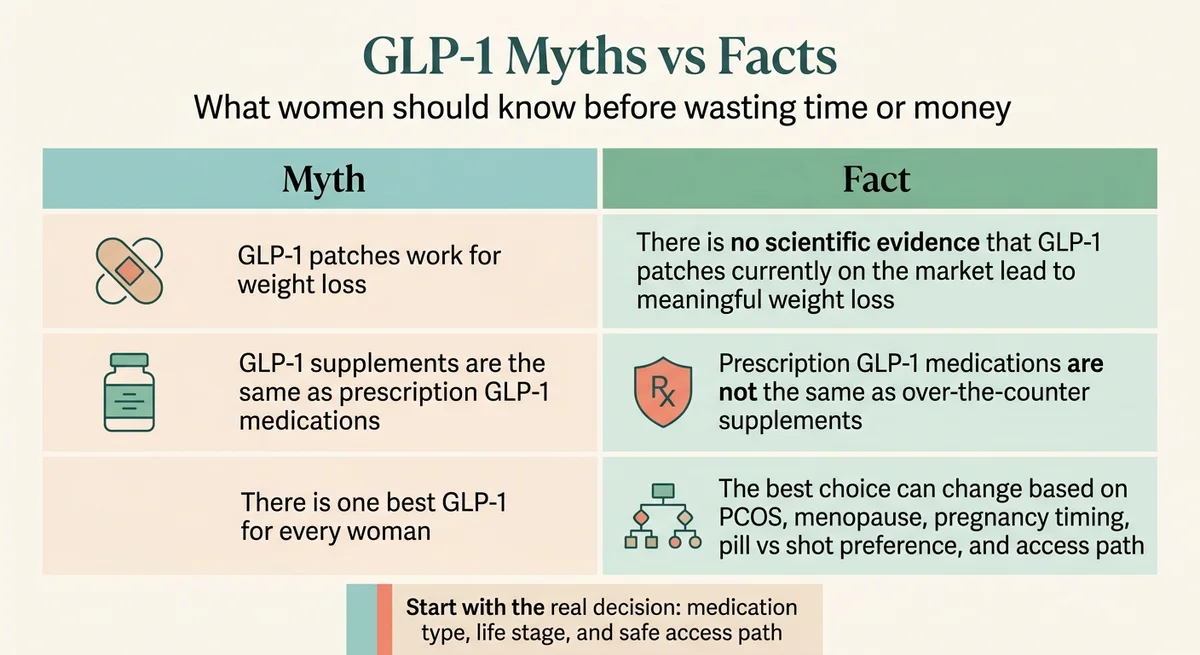
These keep appearing in search results, so let's be direct: no, they do not work. Products marketed as “GLP-1 supplements” are not prescription GLP-1 receptor agonists. There is no scientific evidence that any GLP-1 patch currently sold leads to meaningful weight loss. If you want the benefits that clinical trials consistently show, you need a prescription GLP-1 medication from a licensed provider.
Check your eligibility for FDA-approved GLP-1 medications
Check Eligibility at Ro →Best GLP-1 for Women with PCOS
If you have polycystic ovary syndrome, your relationship with GLP-1 medications is different from the general population — and it may be especially beneficial.
PCOS affects roughly 10% of women of reproductive age, and at its core, it's driven by insulin resistance. About 70–75% of women with PCOS have elevated insulin levels, which drive androgen excess, irregular cycles, weight gain, and fertility challenges.
GLP-1 receptor agonists are not FDA-approved specifically for PCOS, but growing off-label evidence suggests they can help women with PCOS reduce weight, waist size, triglycerides, and total testosterone levels. Prescriptions for GLP-1 medications among women with PCOS have surged more than sevenfold since 2021 as clinicians recognize their value for this population.
If you have PCOS, you already know the standard advice: “lose weight and your symptoms will improve.” What nobody acknowledged for years is that PCOS makes weight loss biologically harder — the insulin resistance that drives PCOS also makes your body exceptionally efficient at storing fat and resistant to releasing it. GLP-1 medications break that cycle by directly targeting insulin signaling and appetite regulation.
Which medication for PCOS?
Tirzepatide's dual GLP-1/GIP mechanism makes it particularly promising because GIP is independently involved in fat metabolism and insulin signaling. Most published PCOS-specific data currently uses semaglutide or liraglutide, and both show benefits. Discuss the options with your prescribing clinician.
If you're trying to conceive
GLP-1 medications should be stopped before pregnancy. Semaglutide: at least 2 months before a planned pregnancy. Tirzepatide: plan timing carefully with your prescriber. GLP-1s can actually improve your chances of conceiving by improving ovulation and metabolic function, but they need to be out of your system first.
If you're on oral birth control
Tirzepatide (Zepbound/Mounjaro) can reduce oral contraceptive effectiveness per the prescribing label. Use a non-oral backup method for 4 weeks after starting and after each dose increase.
Best GLP-1 for Women in Perimenopause and Menopause
If you're in your 40s or 50s and the weight gain feels like it came out of nowhere — even though nothing in your routine changed — you're not imagining it.
When estrogen levels decline during perimenopause and menopause, several things happen simultaneously: insulin resistance increases, fat storage shifts to the abdomen, metabolic rate drops, muscle mass declines, and sleep disruption raises cortisol levels that promote belly fat storage.
RAND survey data found the highest GLP-1 use among women ages 50 to 64 — and the clinical evidence supports that decision. The NewYork-Presbyterian SURMOUNT analysis confirmed tirzepatide works equally well in premenopausal, perimenopausal, and postmenopausal women, producing approximately 20% body weight reduction across all groups.
“I don't recognize my own body anymore.”
— A description many perimenopausal women use. That's not dramatics — it's an accurate account of what happens when the metabolic system that kept your weight stable for 20 years recalibrates without your consent.
GLP-1 + Hormone Therapy: A Combination Worth Discussing
An observational 2024 study published in Menopause found that postmenopausal women on both semaglutide and hormone replacement therapy (HRT) lost more weight than women on semaglutide alone, at every checkpoint through 12 months.
This is an association worth discussing with your provider, not a proven superior protocol — but the biological logic is sound. HRT can reduce visceral fat, improve sleep, and increase activity levels. GLP-1 medications handle appetite and metabolic signaling. Together, they address multiple root causes of menopausal weight gain.
One interaction to know
GLP-1 medications slow gastric emptying, which can affect absorption of oral medications — including oral HRT. If you take oral estrogen, the British Menopause Society recommends considering transdermal HRT (patches or gels) to avoid potential absorption issues. Combined patches or an IUD for progestogen are unaffected.
For the GLP-1 component: both tirzepatide and semaglutide are effective for menopause weight gain
Explore Your GLP-1 Options at Ro →Best GLP-1 for Women Over 40
“Over 40” is not the decision driver — your metabolic history, hormonal status, and fertility plans matter more than the number. That said, this is the decade where many women first notice their previous strategies stop working. Insulin sensitivity declines naturally with age, and muscle mass drops 3–8% per decade after 30.
GLP-1 medications are effective for women in their 40s. The key additions at this age:
- Strength training becomes non-negotiable. Research shows 25–40% of weight lost on GLP-1 medications can be lean mass. In your 40s, you can't afford to lose muscle you'll need in your 60s.
- Protein targets go up. Aim for roughly 1.0–1.5 grams per kilogram of your body weight daily, with higher targets for those doing resistance training.
- If you're considering pregnancy, read the pregnancy section before starting any GLP-1.
What we'd tell a friend turning 40: Start a strength training habit before or alongside the medication — not after you've already lost 30 pounds and feel weaker. The women who maintain results long-term are the ones who built muscle during the weight-loss phase.
Best GLP-1 for Women Over 50
At 50, most women are in perimenopause or recently entered menopause. The GLP-1 choice is the same as the menopause section above, with two additions.
Cardiovascular benefit
GLP-1 medications — particularly semaglutide — have demonstrated significant cardiovascular protection, reducing heart attack and stroke risk independent of weight loss. For women over 50, this isn't a side benefit — for some women, the heart protection alone justifies treatment.
Insurance is worth checking
Women over 50 often have documented comorbidities (hypertension, high cholesterol, prediabetes) that strengthen the insurance case. Ro's insurance concierge checks for you at no extra cost.
Best GLP-1 for Women Over 60
The Johns Hopkins meta-analysis found no clinically significant difference in GLP-1 effectiveness between patients under 65 and those 65 and older. Age alone does not reduce efficacy.
Bone health
Research on fracture risk with GLP-1 medications is mixed and still emerging. Because older women already face higher bone-loss risk, bone health and resistance training deserve extra attention. Weight-bearing exercise, calcium, and vitamin D matter more now.
Muscle preservation is critical
Sarcopenia (age-related muscle loss) accelerates. Resistance training and adequate protein are essential — not optional add-ons.
Slower titration may help
Starting low and increasing gradually reduces side effects, which tend to be more disruptive for older patients.
The Wegovy pill may be more practical
Managing weekly injections alongside multiple other medications can be complex. A daily pill may simplify the routine.
Best medication over 60
Semaglutide (Wegovy pill or injection) for its cardiovascular protection and established safety profile.
Pregnancy, Birth Control, and Breastfeeding: What Every Woman Must Know
This is the section we'd want our own sisters to read before starting.
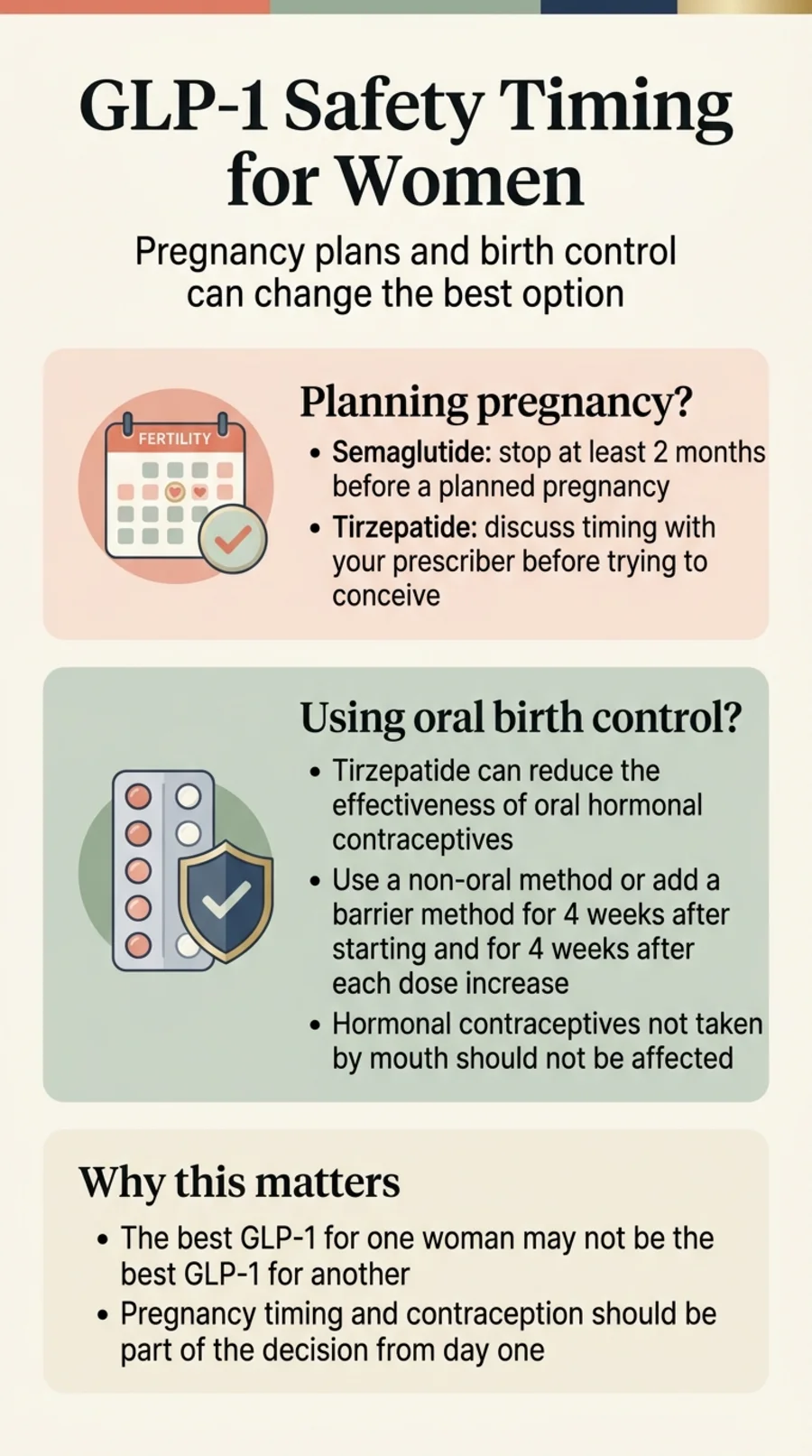
If You May Want to Get Pregnant Soon
GLP-1 medications should be discontinued before a planned pregnancy.
- Semaglutide (Wegovy): The prescribing label recommends stopping at least 2 months before trying to conceive.
- Tirzepatide (Zepbound): Carries a pregnancy warning on its label. The drug's average half-life means it can remain in the body for about 30 days — plan timing carefully with your prescriber, not as a casual rule of thumb.
Animal studies showed developmental abnormalities in fetuses exposed to GLP-1 agonists, though a human study of 168 pregnant women found no increased chance of birth defects. The data is still limited, which is why precaution is standard. GLP-1 medications can actually improve fertility, especially in women with PCOS — weight loss improves ovulation, and improved insulin sensitivity addresses a core driver of PCOS-related infertility.
If You're on Oral Birth Control
Tirzepatide specifically
Tirzepatide can reduce oral contraceptive effectiveness. The Zepbound prescribing label states that oral contraceptives may work less effectively after initiation and dose increases.
What to do: Use a non-oral backup method (condom, IUD, implant, patch) for 4 weeks after starting tirzepatide and 4 weeks after each dose increase.
If You're Postpartum or Breastfeeding
Injectable semaglutide
LactMed reports no detectable semaglutide in breast milk samples. However, data remains limited — discuss with your OB/GYN or pediatric clinician.
Wegovy pill (oral semaglutide)
The prescribing label specifically advises against use during breastfeeding because of SNAC, the absorption enhancer in the tablet coating.
Tirzepatide
The label states it may pass into breast milk. Current guidance is to make an individualized decision with your clinician.
Not sure about timing?
Take Our 60-Second Matching Quiz for Personalized Guidance →FDA-Approved vs. Compounded GLP-1s: What Women Need to Know Before Paying Cash
This section matters because the landscape changed significantly in 2025–2026.
FDA-approved
GLP-1 medications (Wegovy, Zepbound, Saxenda) have gone through the full regulatory review process for safety, effectiveness, and manufacturing quality control.
Compounded
Compounded GLP-1 medications are custom-prepared by compounding pharmacies. They are not FDA-approved. They are not generic versions of brand-name drugs. They have not undergone the same testing. The FDA declared the semaglutide shortage resolved in February 2025 and has since issued warnings and taken enforcement actions against some operations.
Women paying cash for compounded products should understand:
- Compounded GLP-1s are not the same as brand-name medications
- Quality and potency can vary between pharmacies
- The legal landscape is actively evolving
- The FDA has flagged concerns about products that may be counterfeit or contain incorrect doses
We include compounded options in this guide because cost is a genuine barrier for many women. But we will never blur the distinction between FDA-approved and compounded, and neither should your provider.
Best GLP-1 Providers for Women (Compared)
Now that you know which medication fits, here's where to get it. We evaluated providers across pricing, medication access, insurance support, and transparency.
| Ro | MEDVi | Hers | |
|---|---|---|---|
| Best for | FDA-approved + insurance help | Cash-pay, medication included | Women-first branding, pill path |
| FDA-approved meds? | ✅ Wegovy pill, pen, Zepbound | ❌ Compounded only | ✅ Wegovy pill, pen |
| Wegovy pill? | ✅ Yes | ❌ | ✅ Yes |
| Insurance help? | ✅ Insurance concierge | ❌ Cash only | ❌ |
| Membership | $45 first mo, then $145/mo | None — included in med price | $39 first mo, then $149/mo |
| Medication price | Wegovy pill from $149/mo; pen from $199/mo; Zepbound from $299/mo (separate from membership) | Semaglutide from $179 first mo, $299 refills (med included) | Wegovy pill from $149/mo; pen from $199/mo (separate from membership) |
| All 50 states? | ✅ | Most | ❌ Not yet all 50 states |
Ro and Hers medication prices are separate from membership. Novo Nordisk manufacturer offers may reduce Wegovy costs further. Pricing verified March 2026 from official provider pages.
Ro — Best FDA-Approved Access Path for Most Women
Ro is our top recommendation for most women because it offers the widest range of FDA-approved GLP-1 medications, actively helps with insurance navigation, and prescribes the new Wegovy pill.
What Ro does not do is offer the cheapest all-in cash-pay price for compounded medication. But Ro offers something budget-first providers don't: an insurance concierge that can potentially get your FDA-approved GLP-1 covered — which would make it the cheapest option by far. Even partial insurance coverage can reduce your out-of-pocket by hundreds per month.
The Wegovy pill through Ro starts at $149/month for introductory doses via Novo Nordisk manufacturer pricing (through August 2026). Wegovy pen starts at $199/month for the first two fills. Zepbound vials start at $299/month. Membership ($45 first month, then $145/month) is billed separately.
MEDVi — Best Cash-Pay Clinician-Guided Route
MEDVi is our pick for women paying cash who want an all-inclusive price with no separate membership. The semaglutide injection program starts at $179 for the first month and $299 for refills — physician review, plan, guidance, and medication all included.
What MEDVi does not do is offer FDA-approved brand-name medications or insurance billing. If you want Wegovy, Zepbound, or help navigating insurance, Ro is the better fit. Note: MEDVi requires labs after month 2–3 for certain dose increases. Their cancellation policy states no refund except for medical disqualification.
Hers — Best Women-First Pill Path
Hers offers a female-branded experience with clean access to the Wegovy pill (from $149/month) and Wegovy pen (from $199/month). Membership is $39 the first month, then $149/month. GLP-1 medications are not yet available through Hers in all 50 states.
What Hers does not do is provide insurance navigation or the widest geographic coverage. But for women who want a women-first telehealth experience and a straightforward FDA-approved pill path, Hers earns its spot.
Budget Compounded Alternatives
If maximum savings is your priority, both TrimRX and SkinnyRX offer compounded semaglutide and tirzepatide. Both are compounded-only — no FDA-approved medications, no insurance billing. Visit their sites for current pricing. For a full breakdown, see our GLP-1 cost without insurance guide.
GLP-1 Side Effects Women Should Know About
Let's address the side effects you're actually worried about — not the generic bullet list you've seen everywhere else.
The Common Ones (and Why They Usually Get Better)
GI side effects — nausea, diarrhea, constipation, stomach discomfort — are the most common adverse effects across all GLP-1 medications, particularly during dose escalation. Most women report these improve significantly as the body adjusts. Slow titration (starting low and increasing gradually) makes a meaningful difference.
Hair Loss — The Full Truth
Hair thinning (telogen effluvium) is associated with rapid weight loss in general. However, hair loss is also listed as an adverse reaction on Zepbound's prescribing label — so attributing it entirely to “rapid weight loss, not the medication” is an oversimplification.
What helps: adequate protein, not rushing titration faster than your body tolerates, and patience — most hair thinning is temporary and resolves within several months.
Muscle Loss — The One That Matters Most
Research shows 25–40% of total weight lost on GLP-1 medications can be lean mass. For a woman who loses 30 pounds, that could mean 7–12 pounds of muscle — impacting metabolism, bone health, and long-term weight maintenance. A 2025 multi-society advisory specifically flagged muscle and bone loss as key concerns during GLP-1 therapy.
This is solvable:
- Resistance training 2–3 times per week — the single most important protective factor
- Protein intake around 1.0–1.5g/kg body weight daily (roughly 70–100g for most women, higher for resistance training)
- Spread protein across all meals
- Don't skip meals even when appetite is low
Bone Health for Women Over 50
Bone and fracture data for GLP-1 medications are mixed and still emerging. Because older women already face higher muscle and bone-loss risk, bone health planning and resistance training deserve extra attention. Practical steps: weight-bearing exercise, adequate calcium and vitamin D, and bone density monitoring if your doctor recommends it.
Who Should NOT Take GLP-1 Medications
- Women who are pregnant or planning pregnancy without proper washout
- Women currently breastfeeding (especially the Wegovy pill — see breastfeeding section)
- Anyone with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2) — this is a labeled contraindication
- Anyone with a history of pancreatitis should discuss risks carefully before starting
- Anyone with severe gastroparesis
This is not a complete list. A licensed clinician should evaluate your full medical history before prescribing. See our full GLP-1 contraindications guide.
The Muscle and Protein Plan Every Woman on a GLP-1 Should Follow
This section is the difference between losing weight and losing weight well. GLP-1 medications reduce appetite — that's how they work. But reduced appetite without intention means reduced protein, which means muscle loss, which means a slower metabolism, which means harder maintenance if you ever stop the medication.
Protein
Aim for roughly 1.0–1.5 grams per kilogram of body weight daily, with the higher end for women doing resistance training or over 50. For most women, this works out to 70–100+ grams per day. Spread it across meals. A protein shake can help on low-appetite days.
Strength training
Two to three sessions per week. This is the single most protective factor against lean mass loss. The more muscle you keep, the better your metabolism works.
Hydration
GLP-1 medications can reduce thirst signals. Set reminders. Aim for at least 64 oz daily.
Supplements to consider
Vitamin D (especially over 40 or in menopause), calcium (postmenopausal women), vitamin B12 (especially if also on metformin for PCOS or diabetes).
What to Expect Your First Month on a GLP-1
Your first weeks will probably feel different than you expected. Here's an honest preview.
Weeks 1–2
You start at the lowest dose. Most women notice reduced appetite within the first few days. Some feel nauseous — usually mild and manageable. You may also notice you think about food less. That "food noise" quieting is one of the most commonly described effects.
Weeks 2–4
Appetite suppression becomes more pronounced. This is where intentional protein intake matters most — it's easy to undereat without realizing it. Plan your meals even when you're not hungry.
Dose increases (monthly)
Most protocols increase dose monthly until you reach a target level. Side effects often resurface briefly with each increase, then settle. If a dose level is intolerable, your provider can slow the titration.
The biggest first-month mistake
Treating the medication as standalone and skipping protein and strength training. The medication creates the caloric deficit. What you do with that deficit determines whether the weight loss is healthy long-term.
A realistic mindset: This is not a 30-day transformation. The clinical trial results everyone quotes (15–22% body weight loss) happened over 68–88 weeks. Give yourself that same timeline. Women who set 12-month expectations rather than 30-day goals stick with it longer and ultimately lose more weight.
What Real Women Say About GLP-1s
Roughly half of GLP-1 users discontinue within the first year — often due to cost, side effects, or inadequate support. The women who succeed tend to pair medication with protein, strength training, and realistic expectations.
The women who do well describe something specific that no other weight-loss approach gave them: freedom from food noise.
“It's about the mental real estate that's been freed up in my brain, because I'm no longer thinking about food all the time.”
— 48-year-old perimenopausal woman (via Midi Health)
“Many of my patients with PCOS report feeling like a ‘normal’ person does in regard to hunger and cravings.”
— PCOS nutrition specialist (via pcosnutrition.com)
“Since I started HRT and semaglutide, my mood improved. I feel much calmer. After losing weight, everything is more comfortable.”
— Postmenopausal woman (via Midi Health)
The Weight Regain Question — Addressed Honestly
Most people who stop GLP-1 medications regain a significant portion of the weight they lost. This is not personal failure — it's biology. When you stop the medication, the biological drivers of weight gain return.
This reality has led most obesity medicine specialists to view GLP-1 therapy as long-term management for many patients. Some women use them at full dose for a period, then transition to a lower maintenance dose. The key: build the foundation while on the medication. Strength training, protein, sleep, stress management. The women who maintain the most weight after stopping are the ones who used the medication as a platform for change, not a substitute.
Find the right long-term plan for you
Take the Free 60-Second GLP-1 Matching Quiz →How We Ranked These GLP-1 Medications and Providers
Medication rankings are based on published clinical trial data (STEP, SURMOUNT, OASIS trials), FDA prescribing labels, peer-reviewed meta-analyses (JAMA Internal Medicine, The Lancet, NEJM), and women-specific sub-analyses where available.
Provider rankings are based on: medication path clarity, pricing transparency, insurance support, women-specific fit, pill availability, follow-up quality, cancel friction, and verification of official provider pages.
We verify provider pricing monthly by visiting official pricing pages directly. Citations reference FDA labels, PubMed, and institutional research from Johns Hopkins, NewYork-Presbyterian/Weill Cornell, RAND, and the British Menopause Society.
Frequently Asked Questions
Which GLP-1 is best for women overall?
For maximum weight loss, tirzepatide (Zepbound) has the strongest clinical data. For the broadest access — including a daily pill option and insurance support — semaglutide (Wegovy) through Ro is the most practical path for most women.
Do women lose more weight on GLP-1s than men?
In the sex-stratified analysis within a 2026 Johns Hopkins and JAMA Internal Medicine meta-analysis, women lost an average of 10.9% of body weight versus 6.8% for men across six trials. The researchers attributed this to estrogen interactions, metabolic processing differences, and body weight ratios.
What is the best GLP-1 for women with PCOS?
Both tirzepatide and semaglutide show benefits for PCOS used off-label. Tirzepatide's dual GLP-1 and GIP mechanism is particularly promising for insulin resistance, which is central to PCOS. Read our full PCOS guide for details.
What is the best GLP-1 for women in menopause?
Both tirzepatide and semaglutide are effective in postmenopausal women. An observational study found combining semaglutide with HRT may enhance results. The Wegovy pill is a convenient non-injection option for women managing multiple medications.
What is the best GLP-1 for women over 60?
Efficacy does not appear to decline with age. Semaglutide (Wegovy) offers proven cardiovascular protection and an established safety profile for older women. Prioritize strength training and bone health monitoring.
Is tirzepatide or semaglutide better for women?
Tirzepatide produces more weight loss in head-to-head trials. Semaglutide has a longer weight-management track record, now comes as a daily pill, and is more likely to be covered by insurance. GI side effects are common with both.
Is there a GLP-1 pill for weight loss?
Yes. The Wegovy pill (oral semaglutide) received FDA approval in December 2025 and launched in January 2026. You take one tablet daily, 30 minutes before eating or drinking. It produced approximately 13.6% body weight loss in trials.
Does Zepbound affect birth control?
Yes. Per the Zepbound prescribing label, tirzepatide can reduce oral contraceptive effectiveness. Use a non-oral backup method such as a condom, IUD, implant, or patch for 4 weeks after starting tirzepatide and after each dose increase.
Can I take a GLP-1 if I may want pregnancy soon?
You can use a GLP-1 to reach a healthier metabolic state, but must stop before trying to conceive. Semaglutide: stop at least 2 months before a planned pregnancy per the prescribing label. Tirzepatide: discuss timing with your OB-GYN.
Are compounded GLP-1s FDA-approved?
No. Compounded GLP-1 medications are prepared by compounding pharmacies and have not undergone FDA review for safety, effectiveness, or quality control. They are not generic versions of brand-name drugs. The FDA has taken enforcement actions against some compounding operations.
What happens when you stop GLP-1 medication?
Most people regain a significant portion of weight after discontinuing because the biological drivers of weight gain return. Many obesity medicine specialists view GLP-1 therapy as long-term management. Building muscle and healthy habits during treatment improves maintenance if and when you stop.
What GLP-1 has the least side effects?
GI side effects — nausea, constipation, diarrhea — are common across all GLP-1 agents, especially during dose escalation. Individual tolerability varies. Slow titration and working closely with your provider on dose adjustments is the best strategy.
Do GLP-1 supplements or patches work?
No. Products marketed as GLP-1 supplements are not prescription GLP-1 receptor agonists and have not been shown to produce meaningful weight loss. No GLP-1 patch currently sold has scientific evidence of meaningful efficacy.
What is the best GLP-1 provider without insurance?
MEDVi offers compounded semaglutide starting at $179 per month with medication included. Ro offers the Wegovy pill from $149 per month for introductory doses via Novo Nordisk manufacturer pricing through August 2026, plus a membership fee.
How much do GLP-1 medications actually cost?
Brand-name GLP-1s run $900 to $1,350 per month at full retail. In 2026, manufacturer offers include Wegovy pill from $149 per month for introductory doses through August 2026, and Zepbound KwikPens from $299 per month through December 2026. Compounded alternatives start around $179 per month. Insurance copays vary significantly.
Still Not Sure Which GLP-1 Program Is Right for You?
Step 1: Pick your medication path
- Want maximum weight loss? → Tirzepatide (Zepbound)
- Want a pill? → Wegovy pill
- Have PCOS? → Either works — tirzepatide may have an edge for insulin resistance
- May want pregnancy soon? → Talk to your OB/GYN first
Step 2: Pick your access route
- Have insurance (or willing to check)? → Ro
- Paying cash, want FDA-approved? → Ro (Wegovy pill from $149/mo + membership)
- Paying cash, open to compounded? → MEDVi (from $179/mo, medication included)
- Want a women-branded experience? → Hers
Step 3: Take action
The biggest difference between women who succeed with GLP-1 therapy and those who don't is usually fit and follow-through — the right medication path, the right support, and a plan you can actually stay on.
Sources
- McCracken E, et al. “Sex differences in response to glucagon-like peptide-1 receptor agonists.” JAMA Internal Medicine. March 2026. 19,906 patients across six sex-stratified trials; women −10.88%, men −6.78%.
- NewYork-Presbyterian / Weill Cornell Medicine. Analysis of SURMOUNT trials: tirzepatide produced ~20% body weight reduction in women regardless of reproductive stage. 2025.
- FDA Prescribing Information — Zepbound (tirzepatide). Oral contraceptive interaction; pregnancy warning. accessdata.fda.gov
- FDA Prescribing Information — Wegovy (semaglutide 2.4 mg). Pregnancy: discontinue 2 months before planned pregnancy.
- FDA Prescribing Information — Wegovy pill (oral semaglutide 17 mg / 50 mg). Approved December 2025. SNAC breastfeeding warning.
- SURMOUNT-1 trial: Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” NEJM. 2022. Up to 22.5% mean weight loss.
- STEP-1 trial: Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” NEJM. 2021. ~14.9% mean body weight loss.
- SURMOUNT-OSA trial: Malhotra A, et al. “Tirzepatide for the Treatment of Obstructive Sleep Apnea and Obesity.” NEJM. 2024.
- Fong A, et al. Observational study: semaglutide + HRT vs. semaglutide alone in postmenopausal women. Menopause. 2024. Greater weight loss at all timepoints through 12 months.
- RAND Corporation. Survey data on GLP-1 use by age and sex in the United States, 2024.
- LactMed Database. Semaglutide breastfeeding data. National Library of Medicine. Accessed March 2026.
- British Menopause Society. “GLP-1 receptor agonists and HRT: guidance on drug interactions.” 2024. thebms.org.uk
- Ro, MEDVi, Hers. Official provider pricing pages. Verified March 2026.
This page is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before starting any medication. GLP-1 medications require a prescription and are not appropriate for all patients. Individual results vary. Last updated: March 27, 2026 · Provider pricing last verified: March 27, 2026.
Affiliate disclosure: Some links on this page are affiliate links. We may earn a commission if you start a program through our link. This does not affect our rankings or recommendations. Ro is our top pick because we believe it's the strongest overall option for most women. We also recommend MEDVi, Hers, and alternatives where they genuinely fit better.