TYPE 2 DIABETES GUIDE — GLP-1 MEDICATIONS
Best GLP-1 for Diabetes: Every Medication Ranked for Blood Sugar, Heart Health & Cost
If you're searching for the best GLP-1 for diabetes, you've probably noticed the internet is full of weight-loss content — and almost none of it is written for people with type 2 diabetes. You need your A1C down. You want to know which medications actually work best for blood sugar, which ones protect your heart and kidneys, what they really cost, and how to get one without a three-week insurance nightmare.
Here's the short answer, then we'll prove it:
Best GLP-1 for diabetes overall: Ozempic (semaglutide injection). The only GLP-1-class medication with FDA-labeled benefits across all three things that matter most in T2D — blood sugar control, cardiovascular risk reduction, and kidney protection.
Best for maximum A1C reduction + weight loss: Mounjaro (tirzepatide). Produced the largest A1C drop of any GLP-1-class drug in head-to-head trials and significantly more weight loss.
Best if needles are a dealbreaker: Oral semaglutide (Rybelsus) is the established pill option for type 2 diabetes. See how it compares to the new Wegovy pill →
Best if insurance decides: The covered FDA-approved medication is almost always the right real-world choice.
By The RX Index Editorial Team · Last verified: March 27, 2026 · FDA labels checked · ADA 2026 Standards reviewed · All pricing verified
Which one fits your situation?
That depends on your A1C, your heart and kidney health, your feelings about injections, and what your insurance will cover.
Take the Free 60-Second GLP-1 Match Quiz →Answer 5 questions about your diabetes and get your personalized medication and access plan.
How Every GLP-1 for Diabetes Compares — At a Glance
Before we get into the details, here's what the clinical data actually shows when you line these medications up side by side. Built from the largest available meta-analysis (BMJ 2024, 76 randomized controlled trials, 39,246 participants), individual trial data, and current FDA prescribing information.
| Medication | Brand | A1C Reduction | Heart Protection | Kidney Protection | Weight Change | Delivery | Self-Pay Snapshot |
|---|---|---|---|---|---|---|---|
| Semaglutide (injection) | Ozempic | Up to 1.8% | ✅ FDA-labeled (SUSTAIN-6) | ✅ FDA-labeled (FLOW) | ~5–10 lb | Weekly injection | $349/mo via NovoCare; $1,027 list |
| Tirzepatide | Mounjaro | Up to 2.1% | Noninferior to dulaglutide (SURPASS-CVOT) | Data pending | ~25–27 lb | Weekly injection | $1,112 list per fill |
| Semaglutide (oral) | Rybelsus | Up to 1.4% | CV benefit shown (SOUL) | Data pending | ~5–7 lb | Daily pill | $997 list; savings card available |
| Dulaglutide | Trulicity | Up to 1.5% | ✅ FDA-labeled (REWIND) | Some benefit | ~5–7 lb | Weekly injection | ~$987 list |
| Liraglutide | Victoza | Up to 1.1% | ✅ FDA-labeled (LEADER) | Some benefit | ~5–7 lb | Daily injection | ~$800–1,400 list |
| Exenatide | Byetta | Up to 0.9% | Neutral | Neutral | ~2–5 lb | Twice-daily injection | ~$700 list |
A1C reduction ranges from FDA prescribing information and BMJ 2024 network meta-analysis. CV/kidney data from labeled trial results. Weight figures from diabetes-specific trial data. Pricing verified from NovoCare, LillyDirect, and manufacturer sites as of March 2026.
Note: Bydureon BCise (extended-release exenatide) was discontinued by AstraZeneca in late 2024. If you see other sites still listing it as a current option, their information is outdated.
Which GLP-1 Is Best for YOUR Diabetes? Find Your Match
Most pages list every medication without telling you which one fits your life. Here are six real patient scenarios and the best-fit medication for each.
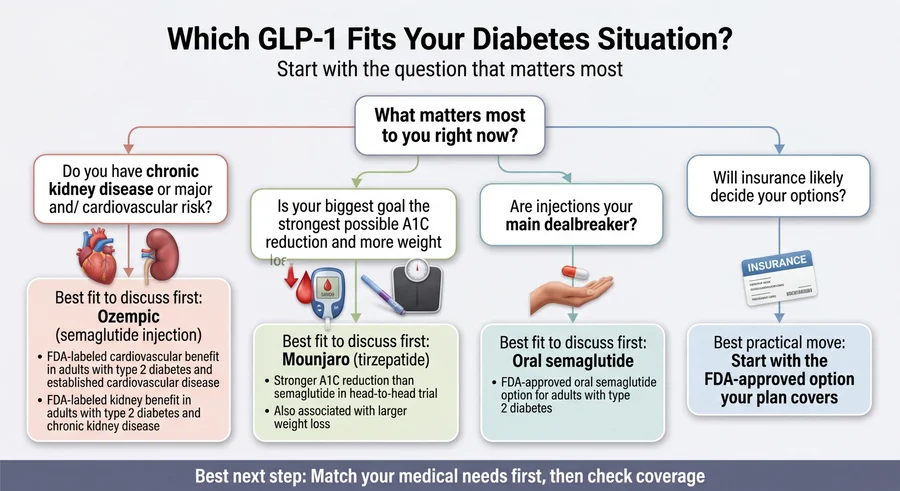
If your A1C is still too high on metformin and you want the strongest overall pick
Best fit: Ozempic (semaglutide injection)
Ozempic is the only GLP-1-class drug with FDA-labeled indications for glycemic control, cardiovascular risk reduction in adults with T2D and established cardiovascular disease, and kidney risk reduction in adults with T2D and chronic kidney disease. That label breadth matters — even if your primary concern right now is blood sugar, heart and kidney complications are the leading causes of serious problems in type 2 diabetes. Ozempic covers more bases from day one than any other option.
The SUSTAIN trials showed A1C reductions of 1.5–1.8%. SUSTAIN-6 demonstrated a 26% relative risk reduction in major adverse cardiovascular events in adults with T2D and established CVD (HR 0.74, 95% CI: 0.58–0.95). The FLOW trial confirmed kidney protection. No other single GLP-1-class product carries all three of those labeled indications.
What to say to your doctor: "My A1C isn't at target on metformin. I'd like to discuss adding a GLP-1 — specifically, could Ozempic make sense given my overall risk profile?"
If your biggest goal is maximum A1C drop and weight loss
Best fit: Mounjaro (tirzepatide)
In the SURPASS-2 head-to-head trial against Ozempic, Mounjaro produced larger A1C reductions (up to 2.1% vs. up to 1.8%) and significantly greater weight loss (~27 lbs vs. ~14 lbs at the highest dose). If your A1C is very high and you also need substantial weight loss, tirzepatide's dual GLP-1/GIP mechanism gives it a real edge.
The honest tradeoff: Mounjaro does not yet have FDA-labeled cardiovascular or kidney indications. SURPASS-CVOT showed noninferior to dulaglutide — but that's not the same as proving superiority over placebo, which is what Ozempic demonstrated in SUSTAIN-6. If you have established heart or kidney disease, Ozempic's evidence is stronger right now.
If you have heart disease or high cardiovascular risk
Best fit: Ozempic (semaglutide injection)
Ozempic's SUSTAIN-6 trial showed a 26% relative risk reduction in MACE (heart attack, stroke, or cardiovascular death) versus placebo in adults with T2D and established CVD. Trulicity (dulaglutide) and Victoza (liraglutide) also carry FDA-labeled MACE-reduction indications (REWIND and LEADER trials) and are solid alternatives if Ozempic isn't accessible. But Ozempic's combined CV-plus-kidney labeling gives it a broader protective profile than any other option.
If you have chronic kidney disease alongside diabetes
Best fit: Ozempic (semaglutide injection)
The FLOW trial specifically studied semaglutide in adults with T2D and CKD. The results led to an FDA-labeled indication to reduce the risk of kidney disease worsening, kidney failure (ESKD), and cardiovascular death in adults with T2D and CKD. Ozempic is the first and currently only GLP-1-class medication with that specific kidney indication — a detail most comparison pages miss entirely, and it matters enormously if your eGFR is declining.
If you absolutely will not do injections
Best fit: Oral semaglutide (Rybelsus)
Rybelsus is the FDA-approved oral GLP-1 for type 2 diabetes. It works — A1C reductions of up to 1.4% — but delivers less reduction than the injection version, partly because pill absorption is lower. The SOUL cardiovascular outcomes trial showed that oral semaglutide also reduced MACE risk in adults with T2D at elevated cardiovascular risk, which meaningfully strengthens the oral option for the right patient.
The practical reality: Take Rybelsus first thing in the morning on an empty stomach with no more than 4 ounces of water, then wait 30 minutes before eating, drinking, or taking other medications. That routine is fine for some people and genuinely difficult for others. Be honest with yourself about whether you'll follow it consistently.
If cost is your biggest barrier
Best fit: It depends on your insurance
Your insurance is significantly more likely to cover a GLP-1 when prescribed for type 2 diabetes than for weight loss. Most commercial plans cover Ozempic and Mounjaro for T2D with prior authorization. Once approved, manufacturer savings cards can bring your copay to as low as $25/month (Novo Nordisk and Lilly savings programs, commercially insured patients only — not applicable to Medicare/Medicaid).
If you don't have insurance or your plan won't cover it, we break down every cost scenario in the pricing section below.
Does one of these profiles sound like your situation?
Take the 60-Second GLP-1 Match Quiz — Get Your Personalized Plan →Why Ozempic Is the Best Overall GLP-1 for Most People With Diabetes
Ozempic (semaglutide injection) offers the best overall balance of blood sugar control, cardiovascular protection, kidney protection, tolerability, and access for adults with type 2 diabetes. It is not the single most powerful A1C reducer — Mounjaro beats it there — but it is the only GLP-1-class medication with FDA-labeled benefits across all three pillars of diabetes management: glycemic control (SUSTAIN trials), cardiovascular protection (SUSTAIN-6), and kidney protection (FLOW).
The honest downside — and why it doesn't change our recommendation
Ozempic does not lower A1C as much as Mounjaro at the highest doses. In the SURPASS-2 head-to-head trial, tirzepatide at 15mg reduced A1C by approximately 2.1% compared to semaglutide 1mg at approximately 1.8%. If your A1C is 10% and your endocrinologist wants the most aggressive reduction possible, Mounjaro may be the better clinical fit.
But most adults with T2D who need a GLP-1 don't only need blood sugar lowering. They need protection against the complications that actually kill people with diabetes — heart attacks, strokes, kidney failure. And on that front, Ozempic has labeled data that Mounjaro doesn't yet have.
If maximum A1C drop is your top priority and you don't have existing heart or kidney disease, Mounjaro is the stronger choice — and we recommend it. See our Mounjaro section below for the full clinical breakdown.
What the FDA label actually says
- Glycemic control: Indicated as an adjunct to diet and exercise to improve glycemic control in adults with T2D
- Cardiovascular: Indicated to reduce the risk of major adverse cardiovascular events (CV death, nonfatal MI, or nonfatal stroke) in adults with T2D and established cardiovascular disease
- Kidney: Indicated to reduce the risk of kidney disease worsening, kidney failure (ESKD), and cardiovascular death in adults with T2D and chronic kidney disease
That triple indication is unique among GLP-1-class medications.
Best for
Adults with T2D who want the strongest evidence-backed overall treatment — especially those with cardiovascular risk factors or kidney concerns.
Not the best pick if
Your single overriding priority is maximum A1C reduction and maximum weight loss, and you have no cardiovascular or kidney disease concerns. In that specific scenario, Mounjaro is stronger.
Ready to find out if Ozempic is covered on your plan?
Ro prescribes FDA-approved GLP-1s including Ozempic and Mounjaro. Their insurance concierge fights for coverage and submits prior authorization on your behalf.
Check GLP-1 Eligibility Through Ro →$45 for the first month. Medication cost separate. Ro handles insurance paperwork and prior authorization.
Why Mounjaro May Be Better If You Need Maximum A1C Reduction
What SURPASS-2 actually showed
The SURPASS-2 trial directly compared tirzepatide (Mounjaro) against semaglutide (Ozempic) in adults with T2D. At the highest dose, tirzepatide produced:
- A1C reduction of approximately 2.1% (vs. ~1.8% for semaglutide)
- 86–92% of patients reaching an A1C below 7%
- Weight loss of approximately 12.4 kg (~27 lbs) vs. 6.2 kg (~14 lbs) for semaglutide
Those are meaningful differences, particularly for patients with very high starting A1C or significant weight to lose.
The detail most pages get wrong
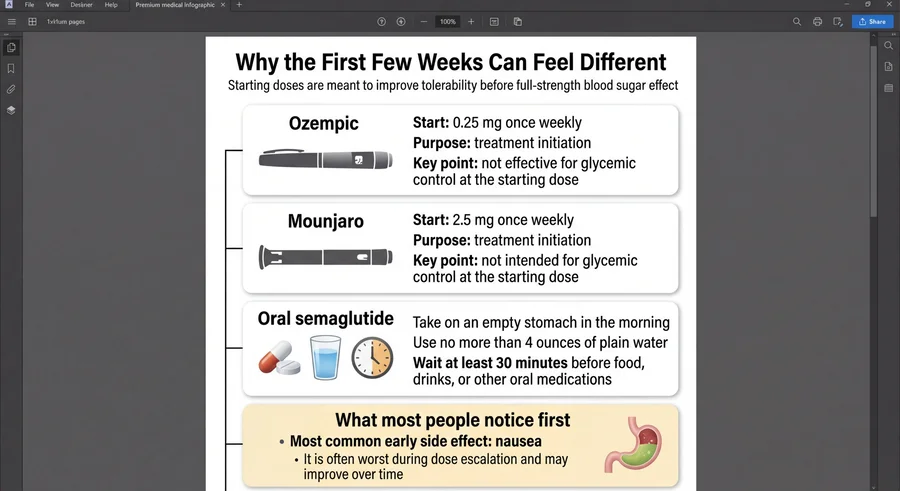
Mounjaro's lowest dose (2.5mg) is a starting dose only — it's not intended for glycemic control. The prescribing information specifies this is an initiation dose to improve GI tolerability during titration. Real therapeutic effect begins at 5mg. If you start Mounjaro and don't see much change in the first month at 2.5mg, that's expected.
Why Mounjaro still isn't the best overall pick for every reader
The SURPASS-CVOT trial showed that tirzepatide was noninferior to dulaglutide for major adverse cardiovascular events. That's an important distinction: "noninferior to an active comparator" is not the same as "proven to reduce cardiovascular events versus placebo," which is what Ozempic demonstrated in SUSTAIN-6 (26% relative risk reduction vs. placebo, HR 0.74). For a patient whose doctor is specifically choosing a GLP-1 because of cardiovascular risk, Ozempic has the more direct proof.
Best for
Adults with T2D whose primary concerns are getting A1C down as aggressively as possible and losing significant weight. Particularly strong if your A1C is above 9%.
Not the best pick if
You have established cardiovascular disease or chronic kidney disease and your doctor is choosing a GLP-1 specifically to protect those organs.
Think Mounjaro might be your best fit?
If your plan covers it, the Mounjaro Savings Card can bring your cost to as little as $25/month for commercially insured patients.
See If Mounjaro Is Covered on Your Plan Through Ro →Is There a GLP-1 Pill for Diabetes? Yes — Here's Who It's Best For
No, you don't have to inject yourself. But the pill option involves real tradeoffs you should understand.
Rybelsus: the established oral option
Rybelsus (oral semaglutide, 7mg and 14mg) has been available since 2019 for type 2 diabetes. It's the same active ingredient as Ozempic but in pill form. A1C reductions reach up to 1.4% — meaningful, but less than the injection. In 2025, the FDA expanded oral semaglutide's labeling to include MACE risk reduction in adults with T2D at elevated cardiovascular risk, based on the SOUL cardiovascular outcomes trial — a significant development that strengthens the oral option.
The daily routine
Take it first thing in the morning with no more than 4 ounces of plain water. Wait at least 30 minutes before eating, drinking anything else, or taking other medications. Skip this step and you're getting a fraction of the intended dose.
Who should choose the pill:
- People with genuine needle phobia or strong injection aversion
- People who want to try a GLP-1 before committing to injections
- People whose insurance covers oral semaglutide but not Ozempic injection
Who should reconsider:
- People who take morning medications that can't wait 30 minutes
- People with irregular morning routines (shift workers, travelers)
- People who want maximum efficacy — the injection delivers more drug
What's on the horizon: orforglipron
Eli Lilly's orforglipron — a once-daily oral GLP-1 without food-timing restrictions — is under FDA review for an obesity indication (PDUFA April 10, 2026). Lilly plans to submit separately for type 2 diabetes later in 2026. In diabetes-specific trials (ACHIEVE-3), orforglipron outperformed oral semaglutide on both A1C (2.2% vs. 1.4%) and weight loss, without Rybelsus's complex dosing rules. It isn't available yet for diabetes, but we'll update this page when it is.
Trulicity, Victoza, and Other GLP-1 Options That Still Matter
Not every patient needs the newest, most powerful option. Here's where the older medications still earn their place.
Trulicity (dulaglutide): the easiest weekly pen
Trulicity has been a workhorse diabetes GLP-1 since 2014. A1C reduction up to 1.5%, FDA-labeled cardiovascular benefit from REWIND, and its pre-filled pen is widely considered the most user-friendly injection device in the class. If your doctor recommends Trulicity and your insurance covers it well, it's a proven choice.
Victoza (liraglutide): older, daily, but still relevant
Victoza established that GLP-1s could protect the heart (LEADER trial, 2016). It's a daily injection — less convenient than weekly options — and its A1C reduction (~1.1%) is lower than the newer drugs. But it has a long safety track record. If it's working for you, there's no automatic reason to switch.
What's been discontinued
Bydureon BCise (extended-release exenatide) was discontinued by AstraZeneca in late 2024. Byetta (immediate-release exenatide, twice daily) is technically still available but rarely prescribed for new starts. If another website is still recommending Bydureon BCise, their information is outdated.
GLP-1 Side Effects: Which One Is Easiest to Tolerate?
Nausea is the most common side effect across the entire GLP-1 class — and it's also the most manageable. For the vast majority of people, nausea is worst during dose escalation (the first 4–8 weeks) and significantly improves or disappears once you reach your maintenance dose.
| Side Effect | Mounjaro | Ozempic | Rybelsus | Trulicity | Victoza |
|---|---|---|---|---|---|
| Nausea | 12–18% | 15–20% | 12–16% | 12–21% | ~28% |
| Diarrhea | 12–17% | 8–10% | 5–9% | 8–12% | ~10% |
| Vomiting | 4–9% | 5–9% | 4–8% | 5–12% | ~6% |
| Constipation | 5–7% | 3–5% | 3–4% | 3–5% | ~10% |
| Discontinued due to GI | 3–7% | 4–5% | 2–4% | 1–6% | ~5% |
Source: FDA prescribing information for each medication. Ranges reflect different doses and trial populations.
Bottom line: Only 3–7% of patients across the class discontinue due to GI side effects. That means over 93% of people tolerate these medications well enough to continue. Mounjaro at lower doses tends to be best-tolerated; Victoza (liraglutide) tends to produce the most nausea because of daily dosing.
What helps
Eat smaller meals. Avoid greasy or heavy foods, especially early on. Stay hydrated. Titrate slowly — don't rush to the full dose. Most patients who push through the first month find that side effects fade substantially.
Rare but serious side effects
All GLP-1 receptor agonists carry a boxed warning: in rodent studies, semaglutide and related drugs caused thyroid C-cell tumors. It is unknown whether these drugs cause medullary thyroid carcinoma in humans. GLP-1s are contraindicated if you have a personal or family history of MTC or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Pancreatitis and gallbladder events have been reported. See our full GLP-1 contraindications guide.
How Much Does the Best GLP-1 for Diabetes Cost in 2026?
Cost is where the rubber meets the road. Let's cut through the confusion.
Scenario 1: You have commercial insurance and a T2D diagnosis
This is the scenario most people don't realize applies to them — and it's the best one. Most commercial insurance plans cover Ozempic and Mounjaro when prescribed for type 2 diabetes. Coverage for diabetes is significantly more accessible than for weight loss alone. Your doctor needs to document: (1) T2D diagnosis, (2) current A1C above target, and (3) that metformin alone isn't sufficient.
Once approved, manufacturer savings cards bring your copay to as low as $25/month for both Ozempic (Novo Nordisk savings card) and Mounjaro (Lilly savings card). These cards work for commercially insured patients only — not Medicare, Medicaid, or other government insurance.
Scenario 2: You have Medicare
Medicare Part D coverage varies by plan. For diabetes indications, many Part D plans cover Ozempic and Mounjaro, though formulary placement and copays differ. Contact your plan directly or ask your pharmacist to run a coverage check. Separately, CMS launched the Medicare GLP-1 Bridge program (July 1–December 31, 2026) covering certain weight-management uses with a $50 copay — that program is separate from standard Part D diabetes coverage.
Scenario 3: No insurance, paying cash for brand-name
- Ozempic: $349/month self-pay for 0.25/0.5/1mg doses through NovoCare's program; $499/month for the 2mg dose. An introductory offer of $199/month may be available for the first two months (terms and availability vary). List price is approximately $1,027 per pen.
- Mounjaro: List price is $1,112.16 per fill. Cash-pay reductions have focused on Zepbound (tirzepatide's obesity brand). If paying cash for Mounjaro for diabetes, expect to pay closer to list unless you qualify for Lilly's patient assistance.
- Rybelsus: List price approximately $997 per package. A savings card is available for commercially insured patients (as low as $25/month); self-pay pricing should be confirmed directly through NovoCare.
Scenario 4: No insurance, budget-constrained
If brand-name FDA-approved medications are beyond your budget even with the programs above, compounded options exist. We address these honestly in the next section — including what the FDA says about them.
Don't want to navigate insurance on your own?
Ro checks your plan, contacts your insurer, and handles prior authorization paperwork on your behalf. If coverage is available, they fight to get it approved.
Get a Personalized GLP-1 Coverage Report Through Ro →Ro member: "I was not expecting insurance help. Usually patients are their own advocate, so I was thrilled to not have to fight for my coverage." — Ro member (compensated testimonial)
What About Compounded GLP-1s for Diabetes?
We're going to be direct here because this topic requires it.
Compounded semaglutide and tirzepatide are available through certain telehealth platforms at lower prices than brand-name drugs. Compounded drugs are not FDA-approved. The FDA does not verify their safety, effectiveness, or quality before they reach patients.
Why FDA-approved should be your first choice for diabetes
For diabetes management specifically — where you're taking a medication long-term to control a chronic, progressive disease — the verification that comes with FDA approval carries real weight. Manufacturing consistency, purity standards, and dosing accuracy are all formally regulated for FDA-approved products. Compounded medications are not.
What's changed in 2026
The FDA has resolved both the semaglutide injection shortage and the tirzepatide injection shortage. That matters because compounding pharmacies had additional latitude to prepare these drugs while shortages existed. With shortages resolved, the FDA has been clarifying enforcement policies and taking action against misleading marketing of non-FDA-approved GLP-1 products.
When compounded options enter the conversation
If you've exhausted the brand-name paths — your insurance won't cover a GLP-1, you don't qualify for manufacturer assistance, and the cash-pay prices above are still out of reach — then a compounded path through a legitimate, licensed provider may come up as a clinician-guided access option.
MEDVi — compounded semaglutide from $179/first month
MEDVi states on its site that its compounded GLP-1s are not FDA-approved or evaluated for safety, efficacy, or quality. For readers who cannot access brand-name at an affordable price and want a clinician-supervised option.
See MEDVi's Current Cash-Pay Pricing →Not FDA-approved. First-line recommendation remains FDA-approved brand-name options when accessible and affordable.
How Doctors Actually Decide Which GLP-1 Is Best
According to the ADA Standards of Care 2026, GLP-1 receptor agonists are recommended as add-on therapy to metformin (or as initial therapy in some cases) based on these factors:
A1C level and glycemic goals
Higher starting A1C may favor more potent options like tirzepatide or semaglutide over older agents.
Cardiovascular disease
If ASCVD is present or risk is high, the ADA specifically recommends a GLP-1 RA with proven cardiovascular benefit — on current FDA labeling, this includes semaglutide (Ozempic), liraglutide (Victoza), and dulaglutide (Trulicity).
Chronic kidney disease
If CKD is present, semaglutide (Ozempic) has the most direct evidence (FLOW trial) and carries the only FDA-labeled kidney indication.
Weight management goals
If weight loss is a priority alongside glycemic control, tirzepatide or semaglutide produce the most weight reduction in this class.
Injection vs. pill preference
Oral semaglutide (Rybelsus) is available for patients who won't do injections, with the caveat that efficacy is lower than injectable versions.
Formulary and cost
This is the practical wildcard that often overrides clinical preference. The drug your insurance covers well is frequently the drug you end up on — and that's okay, because all FDA-approved GLP-1s are effective for blood sugar control.
How Much Do GLP-1s Actually Lower A1C?
The answer depends on three things: which medication, what dose, and where your A1C starts.
| Medication | Typical A1C Reduction | At What Dose |
|---|---|---|
| Tirzepatide (Mounjaro) | 1.9–2.1% | 10–15mg |
| Semaglutide injection (Ozempic) | 1.5–1.8% | 1–2mg |
| Oral semaglutide (Rybelsus) | 1.0–1.4% | 14mg |
| Dulaglutide (Trulicity) | 1.2–1.5% | 1.5–4.5mg |
| Liraglutide (Victoza) | 0.8–1.1% | 1.8mg |
| Exenatide (Byetta) | 0.7–0.9% | 10mcg twice daily |
Why your starting A1C matters
People with higher starting A1C values tend to see larger absolute reductions. If your A1C is 10%, a 2% drop brings you to 8% — meaningful but not at target. If your A1C is 8%, that same drug might bring you to 6.5% — hitting the ADA's recommended target.
How long it takes
A1C reflects your average blood sugar over roughly 2–3 months. Don't expect your A1C to change after 2 weeks on a GLP-1. Most clinicians recheck A1C after 3 months on a stable dose. The full effect is typically visible by 6 months at maintenance dose.
Starter doses don't tell the real story
If you start Mounjaro at 2.5mg or Ozempic at 0.25mg and don't see much change, that's expected — these are titration doses designed to minimize GI side effects. The real A1C impact shows up after you've escalated to therapeutic doses.
Will Insurance Cover a GLP-1 for Diabetes?
Short answer: probably yes, if you have commercial insurance and a documented T2D diagnosis.
What prior authorization usually requires
Insurance companies want to see: (1) a confirmed T2D diagnosis, (2) a recent A1C above your target (usually >7%), (3) documentation that you've tried metformin first (or can't tolerate it), and (4) sometimes evidence of other failed medications (step therapy).
What to ask your insurer
Before your doctor submits prior authorization, call the number on the back of your insurance card and ask:
- "Is Ozempic / Mounjaro on my formulary for type 2 diabetes?"
- "What tier is it on?"
- "Is prior authorization required, and what are the criteria?"
- "Is step therapy required — and if so, which medications do I need to have tried first?"
- "What's my estimated copay at this tier?"
If coverage is denied
- Ask your doctor to submit a peer-to-peer review (a call to the insurance company's medical director)
- File a formal appeal — many medically justified GLP-1 prescriptions are approved on appeal
- Check if the manufacturer assistance program covers your situation
- Explore cash-pay options if appeals fail
Why diabetes coverage is different from weight-loss coverage
Insurance companies have been slow to cover GLP-1s for weight loss — it's often classified as a "lifestyle" benefit. But for type 2 diabetes, GLP-1s are standard-of-care treatment backed by ADA guidelines. That clinical standing makes a real difference in approval rates. If your doctor frames the prescription around your diabetes management (not weight loss), you'll typically have a much easier path.
For more detail, see our full guide to getting insurance to cover GLP-1 medications.
Don't want to deal with insurance calls yourself?
Ro checks your plan, contacts the insurer, and submits all prior authorization paperwork on your behalf. If your plan doesn't cover it, their providers recommend FDA-approved cash-pay alternatives.
Get a Personalized GLP-1 Coverage Report Through Ro →"Since losing 51 pounds through Ro, my day-to-day life has changed dramatically. Someone is always there to walk you through the program." — Ro member (compensated testimonial)
How to Get a GLP-1 Prescription for Diabetes
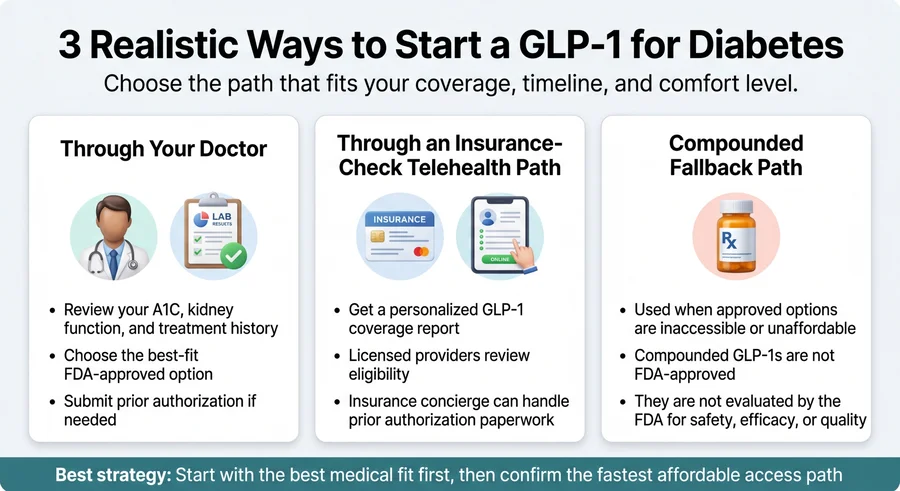
Path 1: Through your doctor
- At your next appointment, raise it directly: "I've been reading about GLP-1 medications for my diabetes. Can we discuss whether one is right for me?"
- Your doctor will check recent labs (A1C, kidney function, lipids) if they haven't been done in the last 3 months
- Based on your clinical profile, they'll recommend a specific medication
- They'll submit prior authorization to your insurance if required
- Once approved, fill at your pharmacy
Timeline: 1–4 weeks from appointment to first dose, depending on insurance
Path 2: Through telehealth (often faster)
- Complete an online health assessment (5–10 minutes)
- A licensed provider reviews your medical history and determines eligibility
- If appropriate, they prescribe a GLP-1 and coordinate with your insurance
- Medication ships to your door or goes to your local pharmacy
Timeline: Cash-pay prescriptions can ship in under a week. Insurance-based prescriptions typically take 2–3 weeks once prior authorization is submitted.
Ro's program prescribes FDA-approved GLP-1s (Ozempic, Mounjaro, Wegovy, Zepbound), includes an insurance concierge that handles prior authorization, and provides monthly provider check-ins. Membership is $45 for the first month and $145/month ongoing — medication cost is separate.
What's Coming: New GLP-1 Medications in the Pipeline
Orforglipron (Eli Lilly)
Once-daily oral GLP-1 pill without food-timing restrictions. Under FDA review for obesity/overweight (PDUFA April 10, 2026). Diabetes-indication submission planned for later in 2026. In head-to-head diabetes data (ACHIEVE-3), outperformed oral semaglutide on both A1C (2.2% vs. 1.4%) and weight loss. Expected cash price: lowest dose starting around $149 via LillyDirect.
Retatrutide (Eli Lilly)
Targets GLP-1, GIP, and glucagon receptors simultaneously. Phase 3 TRANSCEND-T2D-1 results (March 2026) showed A1C reduction of 1.7–2.0% and up to 16.8% weight loss at 40 weeks in T2D. Not yet approved.
CagriSema (Novo Nordisk)
Combination of semaglutide + cagrilintide (amylin analog) in a single weekly injection. Phase 3 results ongoing.
What this means for your decision today: If you need a GLP-1 now, Ozempic and Mounjaro remain the gold standard. The pipeline is exciting but doesn't change today's recommendation. We'll update this page as new approvals happen.
How We Ranked These Medications
We built this ranking around a simple question: if a trusted clinician had to recommend one GLP-1 to the broadest range of adults with type 2 diabetes, what would the evidence support?
| Factor | Weight |
|---|---|
| Clinical fit for diabetes (A1C reduction, glycemic control) | 35% |
| Label breadth and outcomes (FDA-labeled CV and kidney indications) | 25% |
| Tolerability and practical use | 15% |
| Cost and access | 15% |
| Access simplicity | 10% |
Every FDA label claim checked against actual prescribing information on accessdata.fda.gov. Cash-pay prices verified against NovoCare, LillyDirect, and manufacturer pricing pages. Trial data cross-referenced with published results in NEJM, Lancet, and BMJ. Last verified: March 27, 2026 · Next scheduled update: April 2026
What GLP-1 Medications Won't Do — And Why That's Fine
GLP-1s do not cure type 2 diabetes. They manage it — powerfully — but they are ongoing treatment, similar to blood pressure medication. If you stop, your A1C will typically rise back. This is not a failure of the drug. It's the nature of a chronic disease.
GLP-1s do not replace diet and exercise. They work best as part of a comprehensive approach. The medication amplifies your effort — it doesn't replace it.
Not everyone responds the same way. Trial averages don't predict YOUR result. Some people see dramatic A1C drops. Others see modest improvement.
Side effects are real but manageable for the vast majority. Nausea affects 12–28% of patients depending on the medication, but only 3–7% stop treatment because of it. That means over 93% of people stick with it.
Despite those caveats, GLP-1 receptor agonists are among the most effective medications developed for type 2 diabetes. The BMJ 2024 meta-analysis of 76 trials and over 39,000 patients found that every single GLP-1 studied significantly lowered A1C. The best ones also protect your heart and slow kidney decline. The clinical evidence is as strong as it gets.
Frequently Asked Questions
Which GLP-1 lowers A1C the most?
Mounjaro (tirzepatide) at its highest dose produced the largest A1C reduction in clinical trials — up to 2.1% versus placebo, and significantly more than semaglutide in the head-to-head SURPASS-2 trial. Ozempic (semaglutide injection) is the second strongest at up to 1.8%.
Which GLP-1 has the least side effects?
Mounjaro at lower doses and Rybelsus tend to have the lowest discontinuation rates due to GI side effects. Victoza (liraglutide) tends to cause the most nausea because of daily dosing. All GLP-1 side effects improve significantly after the first 4–8 weeks.
Is Mounjaro actually a GLP-1?
Mounjaro (tirzepatide) is not a pure GLP-1 receptor agonist — it is a dual GIP/GLP-1 receptor agonist, meaning it activates two hormone pathways instead of one. Doctors and patients discuss it alongside GLP-1s because it is used for the same conditions and compared in the same clinical contexts.
Can you take a GLP-1 with metformin?
Yes — this is one of the most common medication combinations in type 2 diabetes. GLP-1s and metformin work through different mechanisms and complement each other well. The ADA guidelines specifically support this combination.
Are GLP-1s better than insulin for type 2 diabetes?
For many patients with T2D, GLP-1s are preferred over insulin because they do not cause hypoglycemia, promote weight loss instead of weight gain, and require less blood sugar monitoring. The ADA guidelines recommend GLP-1 receptor agonists before insulin for most T2D patients who need injectable therapy. However, some patients with very high A1C or advanced diabetes may still need insulin, sometimes in combination with a GLP-1.
Are GLP-1s approved for type 1 diabetes?
No. GLP-1 receptor agonists are FDA-approved only for type 2 diabetes and (some formulations) for obesity. The ADA acknowledges limited off-label use in T1D, but this should only be done under close endocrinologist supervision.
How long does it take a GLP-1 to lower A1C?
A1C reflects a 2–3 month average of blood sugar levels. Most clinicians recheck after 3 months at a stable therapeutic dose. Meaningful A1C changes are typically visible by 3–6 months. Do not judge the medication by your first month at a starting dose.
What happens if you stop taking a GLP-1?
Your A1C will typically rise after discontinuation, and weight lost may return. GLP-1s manage diabetes — they do not cure it. Plan for long-term use with your doctor.
Can you switch from Ozempic to Mounjaro?
Yes, with your doctor's guidance. Switching is common and generally straightforward. Your doctor will determine the appropriate starting dose of the new medication.
Are compounded GLP-1s the same as FDA-approved drugs?
No. Compounded medications are not FDA-approved and have not undergone FDA review for safety, efficacy, or manufacturing quality. They are prepared by compounding pharmacies under state-level or facility-specific oversight. For long-term diabetes management, FDA-approved brand-name medications should be the first choice when accessible and affordable.
What if insurance denies Ozempic or Mounjaro for diabetes?
Ask your doctor to file a peer-to-peer review and a formal appeal. Many medically justified GLP-1 prescriptions are approved on appeal. If appeals fail, explore manufacturer patient assistance programs and cash-pay options. Telehealth platforms like Ro include insurance concierge services that handle prior authorization and appeals on your behalf.
Do GLP-1 side effects get better over time?
Yes, for most people. Nausea peaks during dose escalation (the first 4–8 weeks) and substantially improves once you reach your maintenance dose. Studies show the vast majority of patients who experience early GI side effects are able to continue treatment.
References
- Ozempic (semaglutide) prescribing information. Novo Nordisk. FDA Access Data. accessdata.fda.gov/drugsatfda_docs/label/2025/209637s025lbl.pdf
- Frias JP, et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021;385:503-515. (SURPASS-2)
- Eli Lilly. "What to Know About Orforglipron." lilly.com. Updated February 2026.
- Yao H, et al. Comparative effectiveness of GLP-1 receptor agonists on glycaemic control, body weight, and lipid profile for type 2 diabetes: systematic review and network meta-analysis. BMJ. 2024;384:e076410.
- Mounjaro (tirzepatide) prescribing information. Eli Lilly. accessdata.fda.gov/drugsatfda_docs/label/2025/215866s039lbl.pdf
- NovoCare. Ozempic pricing and savings. novocare.com/diabetes/products/ozempic. Verified March 2026.
- Lilly pricing information. Mounjaro list price. pricinginfo.lilly.com/mounjaro. Verified March 2026.
- NovoCare. Rybelsus pricing. novocare.com/diabetes/products/rybelsus/explaining-list-price.html. Verified March 2026.
- SUSTAIN clinical trial program. Published across multiple NEJM and Lancet papers, 2016–2022.
- Marso SP, et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2016;375:1834-1844. (SUSTAIN-6). 26% relative risk reduction in MACE, HR 0.74 (95% CI: 0.58, 0.95).
- Perkovic V, et al. Effects of Semaglutide on Chronic Kidney Disease in Patients with Type 2 Diabetes. N Engl J Med. 2024. (FLOW trial).
- SURPASS-CVOT. Tirzepatide noninferior to dulaglutide for MACE. ACC summary: acc.org. January 2026.
- Trulicity (dulaglutide) prescribing information. Eli Lilly. REWIND trial: Gerstein HC, et al. Lancet. 2019;394:121-130.
- Victoza (liraglutide) prescribing information. Novo Nordisk. LEADER trial: Marso SP, et al. N Engl J Med. 2016;375:311-322.
- Rybelsus (oral semaglutide) prescribing information. Novo Nordisk.
- SOUL trial. FDA expanded oral semaglutide label for CV risk reduction in adults with T2D at elevated cardiovascular risk, October 2025.
- Rosenstock J, et al. Efficacy and safety of once-daily oral orforglipron compared with oral semaglutide in adults with type 2 diabetes (ACHIEVE-3). Lancet. February 2026.
- CMS. Medicare GLP-1 Bridge program. cms.gov/medicare. July 1–December 31, 2026.
- FDA. Compounding and the FDA: Questions and Answers. fda.gov/drugs/human-drug-compounding.
- FDA. Drug shortage resolution notices for semaglutide injection and tirzepatide injection. fda.gov.
- FDA. "FDA Intends to Take Action Against Non-FDA-Approved GLP-1 Drugs." fda.gov/news-events/press-announcements.
- MEDVi. home.medvi.org/glp. "Not FDA-approved or evaluated for safety, efficacy, or quality."
Still not sure which GLP-1 is right for your diabetes?
Everyone's diabetes is different. The right GLP-1 depends on your A1C, your cardiovascular risk, your kidney health, how you feel about injections, and what your insurance will cover. If you've read this far and you're still not sure, that's completely normal — this is a real medical decision with multiple moving parts.
Take the Free 60-Second GLP-1 Matching Quiz →Get a personalized action plan based on your A1C goals, heart/kidney history, pill-vs-shot preference, and budget.
Or, if you already know what you want:
Ro: FDA-approved GLP-1s, insurance concierge, licensed providers. MEDVi: Compounded semaglutide from $179/mo — not FDA-approved.
This content is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before starting or changing any medication. The RX Index may earn a commission through partner links at no additional cost to you. Our recommendations are based on clinical evidence and editorial judgment — affiliate relationships do not influence our rankings. Last updated: March 27, 2026.