How to Get a Letter of Medical Necessity for GLP-1 Medications
By The RX Index Editorial Team ·
Sources: Novo Nordisk official LMN template, Eli Lilly Zepbound/Mounjaro LMN guides, UnitedHealthcare PA criteria, CVS Caremark 2026 formulary guidance, Keystone First, TennCare/OptumRx, HealthCare.gov, CMS. Full methodology below.
Your doctor writes a letter of medical necessity (LMN) for a GLP-1 — not you. But whether that letter actually gets your GLP-1 covered depends almost entirely on what goes into it, what records are attached, and whether your denial is even the kind a letter can fix. Most GLP-1 letters of medical necessity fail not because the patient doesn’t qualify, but because the letter doesn’t match the insurer’s exact criteria — or because the real problem is a benefit exclusion that no letter can override.
We reviewed eight official LMN templates and payer criteria documents to build something that doesn’t exist anywhere else: a denial-fixability framework that tells you whether pursuing a letter of medical necessity for GLP-1 coverage is worth your time, and a 6-point evidence matrix showing exactly what insurers want to see. Below that, we walk through every section of the letter, every denial type, every deadline, and what to do when insurance is a dead end.

Will a GLP-1 Letter of Medical Necessity Actually Help in Your Case?
A letter of medical necessity improves your odds when the denial is fixable — meaning the insurer needs more documentation, a formulary exception, or step-therapy evidence. It usually does not overturn a true benefit exclusion (where your employer’s plan contractually excludes weight-loss drugs) unless you qualify under a different covered diagnosis.
Before anyone writes a letter, classify your situation:
| Your denial situation | Will an LMN help? |
|---|---|
| Missing documentation or invalid diagnosis code | High — this is a paperwork problem |
| Drug is non-formulary | Medium — depends on clinical rationale |
| Step therapy not completed | Medium — need proof of prior failures |
| Renewal denied (BMI now lower or response not documented) | Medium-High — baseline data is key |
| True benefit exclusion (plan excludes weight-loss drugs) | Low — unless another covered indication applies |
Sources: Novo Nordisk’s Wegovy coverage pathway documentation, Eli Lilly’s Zepbound access resources, and UnitedHealthcare’s commercial PA criteria for GLP-1 medications.
“Denied my renewal citing ‘lack of medical necessity’ based on my current BMI.” — r/HealthInsurance
That’s a renewal denial — row four above — and one of the most fixable types when you have baseline documentation.
That table is the single most important thing on this page. If your denial falls in the top four rows, keep reading. If you’re in the bottom row, skip to When a Letter Usually Fails to understand your real options before spending weeks on a letter that won’t work.
What Exactly Is a Letter of Medical Necessity for GLP-1 — and How Is It Different From Prior Authorization?
A letter of medical necessity (LMN) is a formal document written and signed by your healthcare provider — an MD, DO, NP, or PA — that explains to your insurance company why a specific GLP-1 medication is medically required for your health, not optional or cosmetic.
Most people confuse three different documents. Here’s the difference:
| Document | Who initiates it |
|---|---|
| Prior authorization (PA) | Your doctor's office submits a standardized form |
| Letter of medical necessity (LMN) | Your doctor writes a personalized clinical letter |
| Appeal letter | You or your doctor submits after a denial |
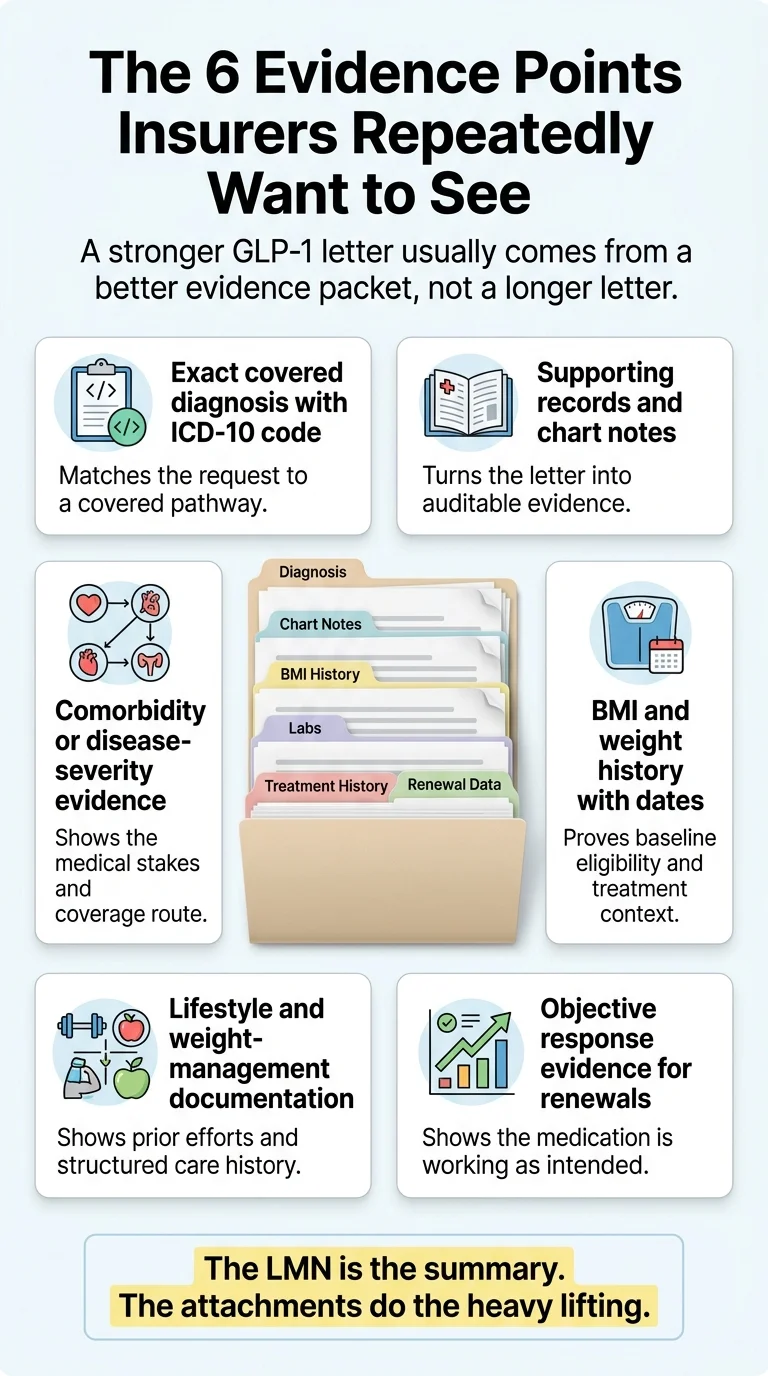
An LMN is not a form — it’s a persuasive clinical argument backed by evidence. Think of it as an executive summary stapled to a proof packet. The letter itself can be one to two pages. The evidence packet attached to it does the heavy lifting.
The 6 Evidence Points Insurers Repeatedly Want to See
We reviewed the official LMN templates and PA criteria from Novo Nordisk (Wegovy), Eli Lilly (Mounjaro and Zepbound), UnitedHealthcare, CVS Caremark, TennCare/OptumRx, and Keystone First. Six documentation elements appear across virtually every source.
The RX Index GLP-1 LMN Evidence Matrix
| Evidence element | Why it matters |
|---|---|
| Exact covered diagnosis with ICD-10 code | The reviewer matches your request to a covered pathway before reading anything else. Wrong code = automatic rejection. |
| Supporting records and chart notes | Turns the LMN from an opinion into auditable evidence. A letter without attachments is a letter without teeth. |
| Comorbidity or disease-severity evidence | Unlocks coverage pathways: obesity + hypertension, cardiovascular risk, MASH, OSA, or diabetes routes |
| BMI and weight history with dates | Proves initial eligibility. For renewals, baseline BMI matters more than current BMI. |
| Lifestyle and weight-management documentation | Many payers require evidence of behavioral, diet, exercise, or structured program participation before approving a GLP-1 |
| Objective response evidence (for renewals) | Renewal denials hinge on proving the drug is working — not re-explaining why you started it |
Sources: Novo Nordisk Wegovy sample LMN template (US25SEMO01618); Eli Lilly Mounjaro sample LMN (pp-tr-us-2466); Eli Lilly Zepbound LMN/access guide; UnitedHealthcare Wegovy commercial PA criteria; UnitedHealthcare Zepbound OSA criteria; CVS Caremark 2026 standard formulary guidance; TennCare/OptumRx GLP-1 PA requirements; Keystone First prior authorization criteria.
“What I don’t know is what a successful appeal actually contains beyond ‘my doctor says I need it.’” — r/GLP1ResearchTalk
That’s the gap. “My doctor says I need it” is not evidence. The six elements above are what turns a weak letter into a strong one.
Who Writes the Letter — and How to Make It Easy for Your Doctor
Your doctor writes the letter. You cannot write your own LMN — it must be signed by a licensed healthcare provider. But you absolutely can (and should) prepare everything your doctor needs to write a strong one quickly.
Here’s the reality: the LMNs that get denied usually came from a patient who showed up empty-handed and a doctor who wrote a vague two-sentence note. The ones that get approved usually had a patient who walked in with organized documentation and a clear summary of the insurer’s criteria.
Which provider type can write it?
Any licensed prescriber (MD, DO, NP, PA) can write an LMN. That said, the practical hierarchy matters:
- ·Endocrinologist or obesity medicine specialist — Strongest credibility signal for GLP-1 LMNs
- ·Primary care physician — Effective when paired with strong documentation and supporting evidence
- ·Telehealth provider — Legally valid — a prescriber with an established treatment relationship and full medical history access can write a more detailed letter
Exactly what to say when you ask
“Dr. [Name], my insurance requires a letter of medical necessity for [medication name]. I’ve organized all the documentation you’d need — my weight history, labs, and a list of treatments I’ve tried. I also have the insurer’s specific criteria. Would you be willing to write the letter? I can send everything through the portal so it’s ready when you sit down to write it.”
That last sentence is key. You’re not asking your doctor to do research. You’re handing them a completed brief.
What if your doctor says no?
Some providers decline because they don’t have time, aren’t familiar with the process, or don’t feel the clinical rationale is strong enough. If that happens:
- 1.Ask if another provider in the practice can write it
- 2.Request a referral to an endocrinologist or obesity medicine specialist
- 3.If you have a separate relationship with a specialist, ask them instead
- 4.Consider a provider like Ro that offers insurance concierge support — their team checks your coverage and submits prior-authorization paperwork on your behalf
Ro Insurance Concierge
Ro's insurance concierge checks your coverage and handles prior-authorization paperwork — so you don't have to navigate it alone.
Check Your GLP-1 Coverage on Ro (Free) →Free coverage check — no subscription required
What Your Doctor Should Include, Section by Section
This is the most important section on this page. We’ve broken down the LMN into nine components based on what appears across the official Novo Nordisk and Eli Lilly sample templates, mapped to the six evidence points insurers want to see.
1. Opening paragraph: State the exact request and denial reason
The letter should open with the prescriber’s name, credentials, NPI, and practice information, then immediately state what they’re requesting and why. If responding to a denial, Lilly’s Zepbound template specifically instructs the prescriber to reference the denial reason verbatim.
- ·“I am writing to document the medical necessity of [drug name] for [patient name].”
- ·State the FDA-approved indication being pursued
- ·If appealing a denial, state the exact denial reason and reference number
2. Diagnosis and ICD-10 code
This is where most weak letters fail. The ICD-10 code must match a covered indication on the patient’s plan. Common codes for GLP-1 LMNs:
| Diagnosis | ICD-10 code | Typically used for |
|---|---|---|
| Morbid obesity (BMI ≥40) | E66.01 | Wegovy, Zepbound weight management indication |
| Other obesity (BMI 30–39.9) | E66.09 | Wegovy, Zepbound — requires comorbidity documentation |
| Obesity, unspecified | E66.9 | Less specific — E66.01 or E66.09 preferred |
| Type 2 diabetes mellitus | E11.x (various) | Ozempic, Mounjaro — diabetes indication |
| Obstructive sleep apnea | G47.33 | Zepbound — OSA indication (requires sleep study) |
| Atherosclerotic cardiovascular disease | I25.x (various) | Wegovy — cardiovascular risk reduction indication |
| MASH (metabolic-associated steatohepatitis) | K75.81 | Wegovy — MASH with liver fibrosis indication |
Critical compliance note: The diagnosis must be accurate and supported by the medical record. Misrepresenting a diagnosis to obtain coverage creates legal and safety issues.
3. BMI and weight history
Include both current BMI (with measurement date) and historical weight data. For renewal appeals, the baseline BMI at treatment start is often more important than the current number — because successful treatment should lower BMI, and a lower current BMI actually proves the drug is working.
Insurer BMI thresholds — verified from official payer criteria:
| PBM / Plan type | BMI threshold |
|---|---|
| CVS Caremark (Wegovy) | ≥30, or ≥27 with weight-related comorbidity |
| CVS Caremark (Zepbound exception) | ≥30, or ≥27 with comorbidity + documented Wegovy failure |
| UnitedHealthcare (Zepbound) | ≥30, or ≥27 with comorbidity (varies by plan) |
| UnitedHealthcare (Wegovy) | Varies — some plans require ≥30, some ≥40 |
| Medicare Part D | Not covered for weight loss |
| Most commercial plans | ≥30, or ≥27 with comorbidity |
Always verify your specific plan’s criteria by calling member services before your doctor writes the letter.
4. Comorbidities and disease severity
List every weight-related comorbidity with supporting evidence. The more comorbidities documented, the stronger the medical necessity argument. Include:
- ·Hypertension — Recent blood pressure readings, medication list
- ·Type 2 diabetes or prediabetes — A1C levels, fasting glucose
- ·Dyslipidemia — Lipid panel results
- ·Obstructive sleep apnea — Sleep study results with AHI score
- ·NAFLD/MASH — Liver enzyme levels, imaging if available
- ·Cardiovascular disease or risk — ASCVD risk score, cardiac history
- ·Osteoarthritis — Joint pain documentation, imaging
- ·PCOS — Hormonal panel, diagnosis documentation
Each comorbidity should have an objective measurement attached, not just a verbal mention.
5. Prior treatment history (step therapy)
Insurers want to see that cheaper alternatives were tried and failed. Document each prior treatment with drug name, dosage, start/end dates, duration, specific outcome (weight change, side effects), and reason for discontinuation.
| PBM | What they typically require |
|---|---|
| CVS Caremark | Wegovy trial (12–16 weeks with <5% weight loss) before Zepbound exception |
| Most commercial plans | Trial of metformin, phentermine, orlistat, Contrave, or Qsymia |
| UnitedHealthcare/OptumRx | Varies by plan — some require prior GLP-1 trial, others require oral agents first |
If you haven’t tried step-therapy medications, some prescribers can argue for an exception based on contraindications or clinical guidelines (ADA 2025 Standards of Care recommend GLP-1s for obesity with cardiovascular risk regardless of prior medication trials).
6. Lifestyle documentation
Many payers require evidence of participation in a structured weight-management program, typically for 3–6 months. CVS Caremark’s current Zepbound criteria specifically require 6 months of structured weight-management documentation. Evidence can include:
- ·Nutritionist or dietitian visit records
- ·Gym membership records or fitness program enrollment
- ·Weight Watchers, Noom, or similar program participation
- ·Primary care notes documenting diet and exercise counseling
- ·Food/exercise diary records
If you don’t have formal program documentation, ask your doctor to add a note documenting the diet and exercise counseling they’ve provided. Some insurers accept provider-documented counseling as meeting this requirement.
7. Clinical rationale: Why this drug, why now
The prescriber explains why this specific GLP-1 medication is the appropriate treatment — not just “a GLP-1” generically. Key clinical studies to cite (print this list and give it to your doctor):
| Drug | Key study to cite | What it showed |
|---|---|---|
| Wegovy (semaglutide) | SELECT trial (NEJM, 2023) | 20% reduction in major cardiovascular events in patients with obesity without diabetes |
| Wegovy | STEP 1–4 trials | Average weight loss of 14.9% over 68 weeks |
| Zepbound (tirzepatide) | SURMOUNT-1 trial (NEJM, 2022) | Average weight loss up to 20.9% over 72 weeks |
| Zepbound | SURMOUNT-OSA trial | Significant reduction in AHI for obstructive sleep apnea |
| Ozempic (semaglutide) | SUSTAIN trials | Significant A1C reduction and cardiovascular benefit in T2D |
| Mounjaro (tirzepatide) | SURPASS trials | Superior A1C reduction compared to other diabetes medications |
| Foundayo (orforglipron) | Phase 3 data (2025–2026) | Only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions — FDA approved 2026 |
Also cite: ADA 2025 Standards of Care, Endocrine Society Clinical Practice Guidelines, and AMA Resolution 420 (2013) which recognizes obesity as a chronic disease.
8. Prognosis without treatment
The prescriber should describe what happens to the patient’s health trajectory if the medication is not provided — referencing cardiovascular risk progression (ASCVD risk score), diabetes risk or progression (A1C trajectory), joint deterioration, sleep apnea worsening, and overall mortality risk.
9. Closing: Contact info and peer-to-peer availability
End with the prescriber’s credentials, board certifications, contact information, and an explicit statement of willingness to participate in a peer-to-peer review (a direct phone call between your doctor and the insurer’s medical reviewer). Proactively offering peer-to-peer availability signals confidence and gives the insurer a faster path to resolution than another round of paper review.
How to Get the Insurer’s Exact Criteria Before the Letter Is Written
Do not let your doctor write a generic letter. Both Novo Nordisk and Eli Lilly tell prescribers to follow the patient’s specific plan requirements — and those requirements vary significantly.
Before your appointment, call your insurance company’s member services line and ask these exact questions:
- 1."Is my denial for lack of medical necessity, non-formulary status, step-therapy requirements, or a benefit exclusion?" — This determines your entire strategy.
- 2."What exact clinical criteria does my plan require for [drug name] approval?" — Ask them to read the criteria or mail/fax them to you.
- 3."Does the plan require a specific authorization form in addition to a letter of medical necessity?" — Lilly's official guidance warns that some plans require specific forms and the wrong format can delay the process.
- 4."What supporting documents should be attached?" — Lab work? Chart notes? Sleep study?
- 5."What is my appeal deadline?" — Write this down. Most plans give 180 days, but yours may differ.
- 6."Is there a formulary exception pathway or alternate covered indication that applies?" — This is the question that can change everything.
How to Match the Letter to Your Specific Denial Reason
Not every denial needs the same letter. The strategy changes based on what the insurer actually said.
If the denial says "not medically necessary"
This is the most common — and most fixable — denial type. It means the insurer reviewed the submitted documentation and decided it didn’t meet their clinical criteria. Usually, the problem is incomplete documentation, not a true exclusion. Fix it by: Identifying which specific criteria weren’t met (BMI? Comorbidities? Step therapy? Lifestyle program?), gathering the missing evidence, and resubmitting with a comprehensive LMN that addresses each criterion point by point.
If the drug is non-formulary
Your plan covers GLP-1s, but not the specific one prescribed. This requires a formulary exception request — a formal ask for the plan to cover an off-formulary drug because of clinical reasons. Fix it by: Having the prescriber explain why this specific drug is necessary and why formulary alternatives are not appropriate (different mechanism, prior failure, contraindication, or clinical superiority). Important for Zepbound patients: CVS Caremark removed Zepbound from its standard formulary in July 2025. CVS Caremark now requires a documented Wegovy trial of 12–16 weeks showing less than 5% weight loss before considering a Zepbound formulary exception.
If step therapy wasn't completed
The insurer requires proof you tried cheaper medications first. Fix it by: Documenting every medication you’ve tried — dates, dosages, duration, and specific reasons it didn’t work. If you have a medical reason to skip step therapy (contraindication, drug interaction, or clinical guidelines supporting direct GLP-1 use), the prescriber should cite that explicitly.
If the renewal was denied
You were on the medication, it was working, and the insurer cut you off — often because your current BMI dropped below their threshold. Fix it by: Submitting baseline BMI (before treatment), current BMI, objective response data (weight loss percentage, A1C improvement, blood pressure changes), and a clinical argument that discontinuing treatment would cause health regression. The STEP 1 trial extension showed patients regained approximately two-thirds of their weight within a year of stopping semaglutide — that data point belongs in the letter.
If the plan says weight-loss drugs are excluded
This is the hardest denial to overturn. If your employer’s plan contractually excludes weight-loss medications, an LMN arguing for obesity treatment usually will not override the contract language. But that’s not always the end of the road — see the next section on alternate diagnosis pathways.
When Another Diagnosis Can Unlock Coverage
Some plans exclude “weight-loss drugs” broadly but still cover GLP-1 medications under other FDA-approved indications. This is where the specific drug and your specific health profile create opportunities that a generic LMN approach would miss.

| Drug | Alternate covered indication |
|---|---|
| Wegovy | Cardiovascular risk reduction in adults with established CVD and obesity/overweight |
| Wegovy | MASH (metabolic-associated steatohepatitis) with liver fibrosis |
| Zepbound | Moderate-to-severe obstructive sleep apnea in adults with obesity |
| Ozempic | Type 2 diabetes (glycemic control) |
| Mounjaro | Type 2 diabetes (glycemic control) |
“My dr was able to get Zepbound approved ... with a letter of medical necessity for Sleep Apnea.” — r/glp1
Compliance note: The diagnosis must be real and supported by objective testing. Many people with obesity have undiagnosed sleep apnea, undiagnosed prediabetes, or undocumented cardiovascular risk — getting properly evaluated serves their health regardless of insurance strategy.
When a Letter of Medical Necessity Usually Fails
A letter of medical necessity does NOT usually overturn a true weight-loss benefit exclusion. Novo Nordisk’s own Wegovy coverage documentation explicitly separates benefit exclusions from other denial types and warns that obesity-drug exclusions typically result in automatic denials regardless of medical necessity arguments.
If your employer’s plan says “weight-loss medications are excluded from coverage” and you don’t qualify under an alternate covered indication, then rewriting the same LMN three times is not a strategy — it’s a stall.
Here’s what actually works in that situation:
Employer-benefits escalation
If you work for a large company, HR controls the benefit design — not the insurer. Some employees have successfully petitioned HR to add GLP-1 coverage. According to the KFF 2025 Employer Health Benefits Survey, 19% of firms with 200+ workers cover GLP-1 drugs for weight loss, and among firms with 5,000+ employees that number jumps to 43%. Coverage is expanding.
Open enrollment plan switch
During open enrollment, evaluate whether plans using different PBMs (Express Scripts, OptumRx) or plan tiers offer GLP-1 coverage. One plan from the same employer may exclude GLP-1s while another covers them.
Skip insurance entirely
If the appeal math doesn’t add up, cash-pay GLP-1 programs bypass the entire insurance apparatus — no LMN, no prior auth, no denial letters, no waiting weeks for a decision. See the cash-pay options below.
For a full walkthrough of every insurance coverage strategy — not just the LMN — see our complete guide to getting insurance to cover GLP-1 medications.
If Insurance Is a Dead End: Cash-Pay GLP-1 Providers That Don’t Require an LMN
If your plan excludes weight-loss drugs, your appeal was denied, or you’d rather not spend weeks navigating paperwork — legitimate telehealth providers offer GLP-1 programs with no insurance, no LMN, and no prior authorization required.
Ro — Best for Insurance Help + Cash-Pay Backup
FDA-approved medications · Insurance concierge · All 50 states
- ✓Membership: $39 first month, then as low as $74/mo with annual plan ($149/mo monthly billing). Medication separate.
- ✓FDA-approved medications: Wegovy, Zepbound KwikPen, Foundayo (orforglipron) — the only GLP-1 pill with no food or water timing restrictions
- ✓Free GLP-1 Insurance Coverage Checker — checks your plan before you pay anything
- ✓Insurance concierge checks coverage and handles PA paperwork
- ✓Available in all 50 states and D.C.
Free coverage check — no prescription or commitment required
MEDVi — Best Compounded Cash-Pay Option
Compounded GLP-1 · No insurance required · Competitive pricing
When the math on insurance doesn’t work — your plan excludes GLP-1s, your appeal failed, or you don’t want to spend weeks fighting — compounded GLP-1 programs can offer a significantly more affordable path. MEDVi is the strongest option we’ve reviewed for licensed providers, verified pharmacy sourcing, and consistently competitive pricing.
- ✓Best for: Readers whose insurance is a dead end and who want to start treatment without waiting
- ✓Medications: Compounded semaglutide and tirzepatide
- ✓No prior authorization or LMN required
FDA compliance note: Compounded GLP-1 medications are not FDA-approved products and are not interchangeable with brand-name Wegovy, Zepbound, or Ozempic. See the FDA compounded GLP-1 information page.
Other legitimate cash-pay options
- Eden Health — Strong clinical feel with licensed providers. Good for readers who want a more traditional medical experience from a telehealth provider.
- SkinnyRX / TrimRX — Budget-friendly compounded options for cost-sensitive readers.
- LillyDirect — Brand-name Zepbound vials at $449/month (7.5mg+ doses) direct from Eli Lilly, no insurance required.
Medicare and GLP-1 Coverage in 2026: The GLP-1 Bridge
The baseline rule: Medicare Part D cannot cover GLP-1 medications prescribed solely for weight loss due to federal statute. However, Part D can cover GLP-1s prescribed for covered indications — type 2 diabetes (Ozempic, Mounjaro), obstructive sleep apnea (Zepbound), and cardiovascular risk reduction or MASH (Wegovy).
For Medicare beneficiaries pursuing an LMN now: Focus your letter on a covered indication (T2D, OSA, CV risk, or MASH) rather than weight management alone. That gives you the strongest path under current Part D rules while the Bridge program ramps up.
How to Submit the Appeal Without Missing Deadlines
Appeal timing is where many patients lose. They wait, they procrastinate, they miss the window.
How long you have to file
| Action | Deadline |
|---|---|
| File an internal appeal after denial | Up to 180 days on most plans (check your denial letter — yours may differ) |
| Request external review after final internal denial | At least 4 months from final internal decision under federal rules |
How long the insurer has to respond
| Action | Insurer’s deadline |
|---|---|
| Respond to a standard prior authorization request | 15 days |
| Respond to an urgent/expedited PA request | 72 hours |
| Decide an internal appeal (pre-service) | 30 days |
| Decide an internal appeal (post-service) | 60 days |
| Decide a standard external review | 45 days |
| Decide an expedited external review | 72 hours |
The appeal submission checklist
- 1.Get the denial in writing. You need the exact denial reason, the criteria they used, and the appeal deadline.
- 2.Gather all evidence. Use the 6-point evidence matrix above. Don't submit a letter without attachments.
- 3.Have your doctor write or update the LMN. Address the specific denial reason, not generic medical necessity.
- 4.Submit through the correct channel. Some plans require fax, some have online portals, some accept mail. Confirm with member services.
- 5.Keep records. Save confirmation numbers, fax receipts, portal screenshots, and call notes with dates and representative names.
- 6.Follow up before the deadline. Call to confirm receipt within 5 business days of submission.
- 7.Request a peer-to-peer review. Your doctor speaking directly with the insurer's medical reviewer can be one of the most effective steps — ask proactively, don't wait for the insurer to offer it.
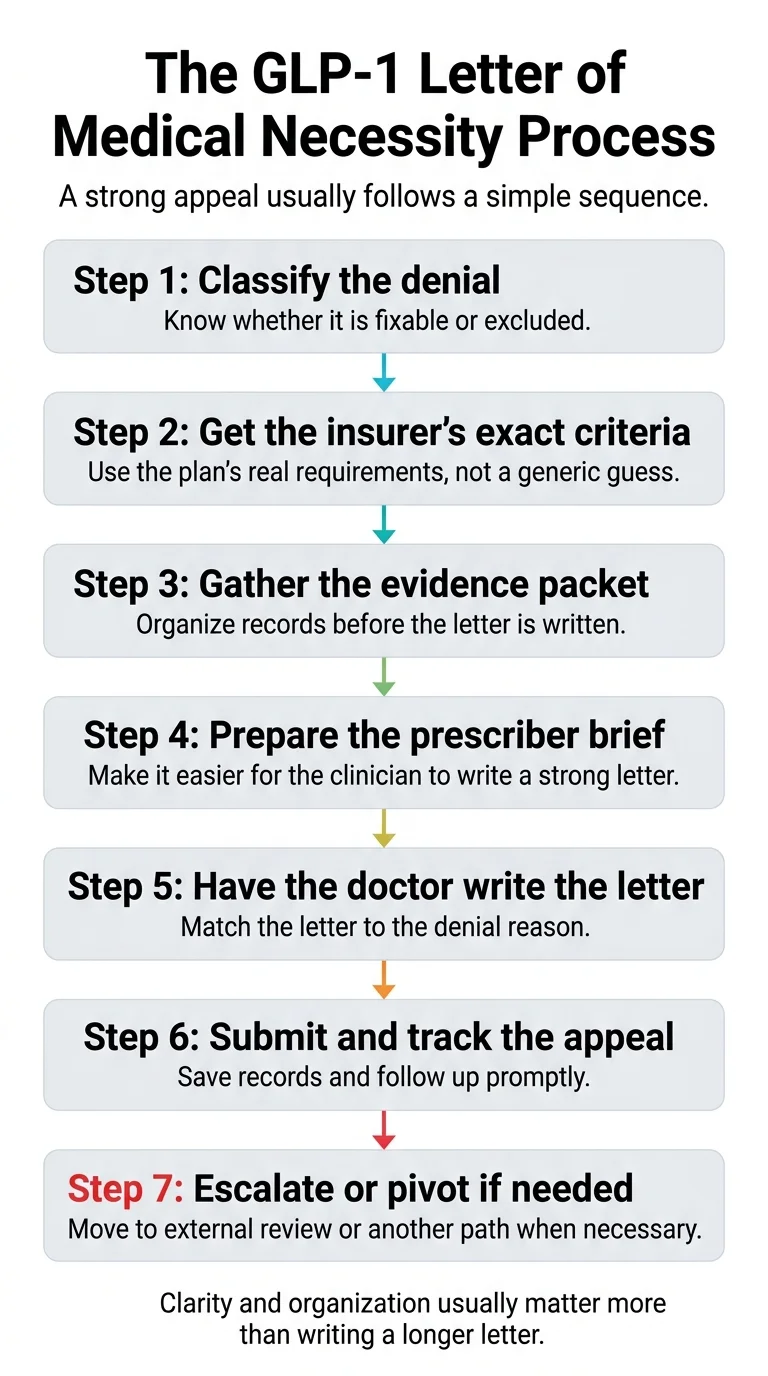
The Step-by-Step GLP-1 Letter of Medical Necessity Process
Here’s the complete sequence, start to finish:
- 1
Classify your denial.
Use the fixability table at the top of this page. Is it a documentation gap, formulary issue, step-therapy problem, renewal denial, or true benefit exclusion?
- 2
Get the insurer's exact criteria.
Call member services using the phone script above. Write down every criterion they list. Ask for the specific form required.
- 3
Gather your evidence packet.
Use the 6-point evidence matrix as your checklist. Collect labs, weight history, medication history, lifestyle documentation, and any specialist records.
- 4
Prepare the prescriber brief.
Organize everything into a one-page summary your doctor can reference while writing the letter. Include: the denial reason, insurer criteria, your BMI and weight timeline, comorbidities with lab values, medications tried with dates and outcomes, lifestyle program documentation, and the clinical studies relevant to your drug.
- 5
Schedule the appointment.
Tell the office you need an LMN for a GLP-1 insurance appeal and you're bringing all documentation. Ask for extra time if needed.
- 6
Have your doctor write and submit the LMN.
The letter should address the exact denial reason, include the evidence packet, use the correct ICD-10 code, and offer peer-to-peer review availability.
- 7
Track and follow up.
Confirm submission receipt within 5 days. Note every deadline. If no response within the expected timeframe, call and escalate.
- 8
Escalate or pivot.
If the appeal is denied, request external review. If external review fails or the denial is a true exclusion, pivot to an alternate covered indication or a cash-pay provider.
Ro Insurance Concierge
Ro's concierge checks your coverage and submits prior-authorization paperwork so you can focus on starting treatment.
Let Ro Handle the Insurance Process →Free coverage check — no subscription required
Using HSA or FSA to Pay for GLP-1 Medications
Even if you’re paying cash for a GLP-1 through a telehealth provider, your HSA (Health Savings Account) or FSA (Flexible Spending Account) may reimburse the expense — but the documentation requirements depend on your plan administrator.
What the IRS says: Under IRS Topic 502, weight-loss expenses can qualify as deductible medical expenses when prescribed to treat a specific disease diagnosed by a physician (such as obesity, type 2 diabetes, or cardiovascular disease).
What this means practically: Your plan administrator determines what documentation they need to verify the expense. This may include a prescription, a detailed receipt, a letter from your provider connecting the medication to a diagnosed medical condition, or some combination.
What to keep on file: Your prescription, itemized receipts showing the medication and provider, and any documentation from your provider that connects the GLP-1 to a medical diagnosis.
For a deeper dive on which GLP-1 programs work best with HSA and FSA payments, see our GLP-1 HSA/FSA eligibility guide.
Frequently Asked Questions
Can my primary care doctor write a GLP-1 letter of medical necessity?
Yes. Any licensed prescriber (MD, DO, NP, or PA) can write an LMN. What matters most is whether the letter addresses the insurer's specific criteria and includes supporting evidence — not the prescriber's specialty.
Do I need a separate letter if prior authorization was already denied?
Usually, yes. The initial PA submission is a standardized form. An LMN is a more detailed, personalized clinical argument submitted alongside an appeal. Think of the PA form as the application and the LMN as the supporting brief.
How long should the letter be?
One to two pages for the letter itself, plus as many pages of attachments (labs, records, medication history, program documentation) as needed to support the case. Novo Nordisk's sample LMN template suggests the letter itself takes about 10–15 minutes to write when the clinician has all supporting data ready.
Will a letter help if my plan excludes weight-loss drugs?
Usually not for the exclusion itself. But if you qualify under an alternate covered indication — cardiovascular risk reduction (Wegovy), obstructive sleep apnea (Zepbound), MASH with fibrosis (Wegovy), or type 2 diabetes (Ozempic, Mounjaro) — a letter targeting that indication can succeed even when the 'weight-loss drug' category is excluded.
What if the denial says my current BMI is too low now?
This is a renewal denial. Your prescriber should include your baseline BMI (before treatment started) alongside your current BMI to show that the medication is working as intended. Include clinical data showing health improvements and cite the STEP 1 trial extension, which demonstrated that patients regain approximately two-thirds of lost weight within a year of stopping semaglutide.
Can Zepbound be covered for sleep apnea even if weight-loss drugs are excluded?
In some plans, yes. Zepbound's FDA-approved indication for moderate-to-severe obstructive sleep apnea in adults with obesity is a separate coverage pathway. This even applies to some Medicare Part D plans that otherwise exclude weight-loss medications. A sleep study showing AHI ≥15 is required.
What about Medicare coverage for GLP-1s?
Medicare Part D doesn't cover GLP-1s for weight loss, but does cover them for type 2 diabetes, OSA (Zepbound), cardiovascular risk (Wegovy), and MASH (Wegovy). Additionally, the CMS Medicare GLP-1 Bridge program (July–December 2026) will offer Foundayo, Wegovy, and Zepbound KwikPen to eligible beneficiaries at a $50 monthly copay.
Can an LMN help with HSA or FSA reimbursement?
It depends on your plan administrator. The IRS requires that weight-loss expenses treat a specific diagnosed disease to qualify as medical expenses. Your administrator determines what documentation they need — this may include a prescription, itemized receipt, or provider letter connecting the medication to a medical diagnosis.
What if my doctor doesn't know what to include?
Prepare a one-page prescriber brief using the evidence matrix and section-by-section breakdown in this guide. Print the relevant clinical study citations from the table above. Organizing the information so your doctor can focus on writing — not researching — is the single best thing you can do.
What if I need a provider who handles insurance paperwork?
Ro offers a free GLP-1 Insurance Coverage Checker and an insurance concierge that checks your coverage and submits prior-authorization paperwork. Membership starts at $39 for the first month (medication cost is separate).
How long do I have to appeal?
Most marketplace and private plans allow up to 180 days for an internal appeal, but your specific plan may differ. After a final internal denial, federal rules give you at least 4 months to request an independent external review. Check the deadline on your denial letter immediately — it's the first thing to look at.
How We Built and Verify This Guide
This guide was built from primary official sources — not by summarizing other blog posts.
Official sources reviewed:
- ·Novo Nordisk Wegovy Sample Letter of Medical Necessity (US25SEMO01618)
- ·Novo Nordisk Wegovy Coverage Pathway Documentation (novoMEDLINK)
- ·Eli Lilly Mounjaro Sample Letter of Medical Necessity (pp-tr-us-2466)
- ·Eli Lilly Zepbound Appeals and LMN Guide
- ·Eli Lilly Zepbound Access and Coverage Page
- ·UnitedHealthcare Wegovy Commercial PA Criteria
- ·UnitedHealthcare Zepbound OSA Coverage Criteria
- ·CVS Caremark 2026 Standard Formulary Guidance
- ·TennCare/OptumRx GLP-1 PA Requirements
- ·Keystone First Prior Authorization Criteria
- ·HealthCare.gov Internal Appeals and External Review Guidelines
- ·CMS Appeal Regulations
- ·CMS Medicare GLP-1 Bridge
- ·IRS Topic 502: Medical and Dental Expenses
- ·KFF/Peterson Health System Tracker 2025 Employer Survey
- ·ADA 2025 Standards of Care in Diabetes
Refresh schedule: Payer criteria and provider pricing are re-verified monthly. Clinical guideline citations are updated annually. The “Last verified” date at the top of this page reflects the most recent full review.
What this guide covers: How to get, prepare for, and strengthen a letter of medical necessity for GLP-1 medications, including when a letter is likely to work and when it isn’t.
What this guide does not cover: Specific legal advice, plan-specific contract interpretation, or medical recommendations. Always work with your healthcare provider and review your specific plan documents.
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
Not sure which GLP-1 path is right for your situation?
Take our free 60-second matching quiz to find the right provider for your budget, insurance, and medication goals.
Find My GLP-1 Path →