Switching Guide · Last verified April 7, 2026 · FDA, SURMOUNT-5, Zepbound Label
How to Switch From Compounded Semaglutide to Tirzepatide
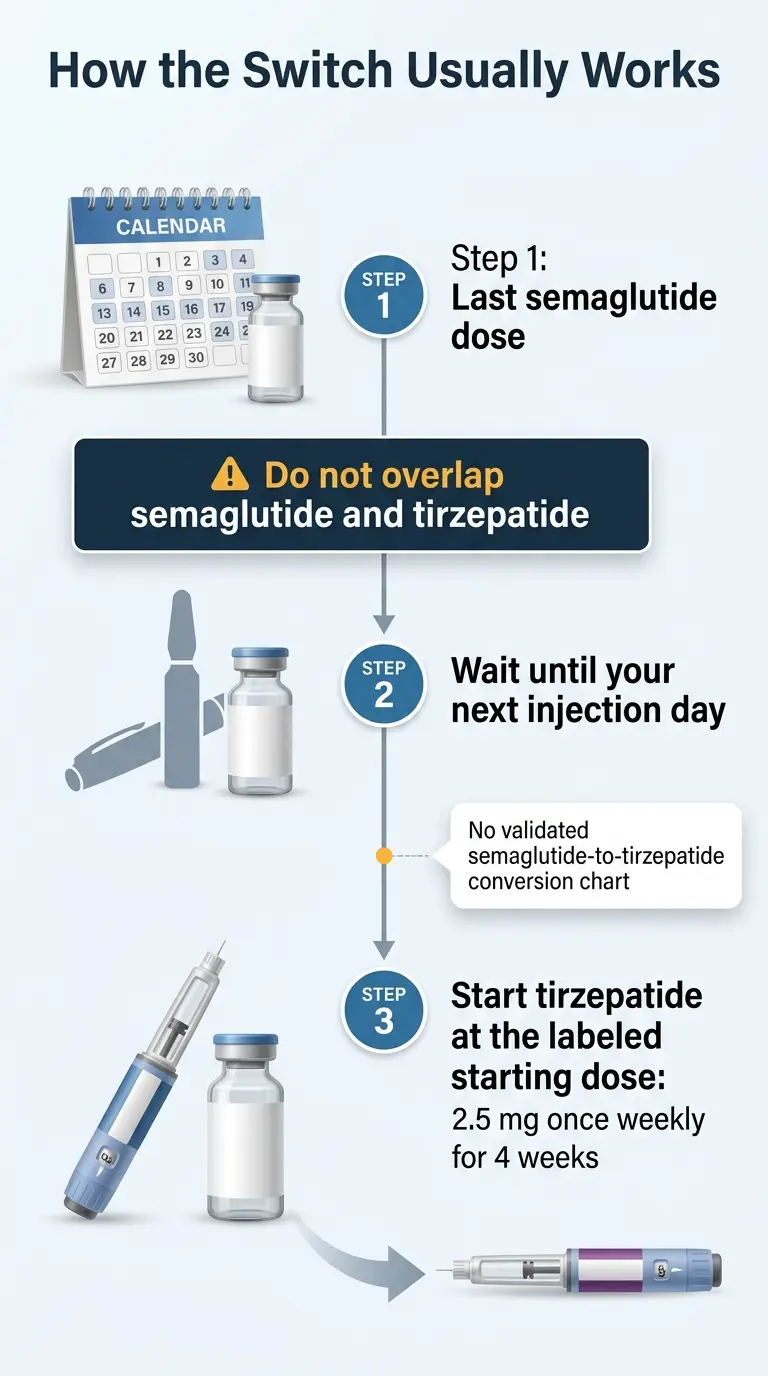
The clinician-guided approach is straightforward: take your last semaglutide injection as scheduled, wait about 7 days (your normal injection day), and start tirzepatide at 2.5 mg under a prescriber’s guidance. Do not overlap the two medications. There is no validated dose conversion chart — any website offering one is giving you false precision that could actually hurt you.
FDA-approved Zepbound (tirzepatide) starts at $299/month through LillyDirect.1 If you have eligible commercial insurance, the Zepbound savings card may bring your cost as low as $25/month.2
By The RX Index Editorial Team · · · Affiliate disclosure · Editorial standards
Quick Reference: The Switch at a Glance
| Question | Answer |
|---|---|
| Can you switch? | Yes, with prescriber guidance |
| Need a washout period? | Usually no — most clinicians start tirz on your next injection day |
| Can you take both at once? | No. Zepbound labeling states coadministration with another GLP-1 agonist is not recommended³ |
| Starting tirzepatide dose? | 2.5 mg/week for 4 weeks is the labeled starting dose; some clinicians individualize for GLP-1-experienced patients³ |
| Conversion chart? | No validated one exists. Do not self-convert |
| Cost (Zepbound self-pay)? | $299–$449/month via LillyDirect; as low as $25/month with eligible commercial insurance¹² |
| Best first step? | Send your vial label and last injection date to a licensed prescriber |
Not sure whether to switch or stay on semaglutide? Answer 6 questions and get a personalized GLP-1 path — including whether tirzepatide or semaglutide fits your budget, goals, and situation.
Take the free 60-second matching quiz →Should You Actually Switch? An Honest Decision Filter
Before we get into the how, let’s talk about whether you should. Switching medications is not a casual decision, and not everyone on compounded semaglutide needs to make this move.
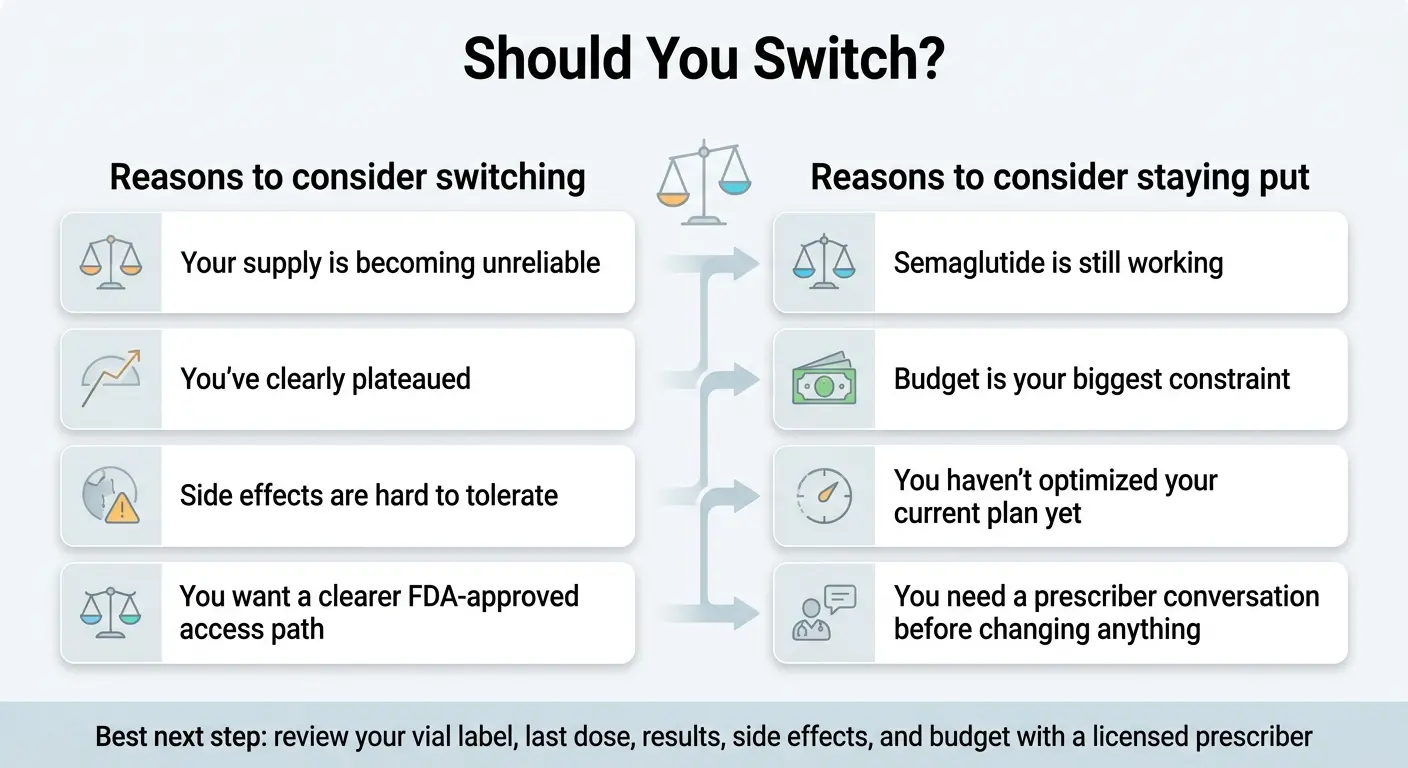
Consider switching if:
- ✓You've been at an adequate semaglutide dose for months and progress has clearly stalled. If you've maxed out your tolerated dose and the scale hasn't moved despite consistent habits — tirzepatide's dual GLP-1 + GIP mechanism may break through where semaglutide alone can't.
- ✓Your compounded semaglutide access is ending or becoming unreliable. This is the most common trigger behind this search right now.
- ✓Semaglutide side effects are interfering with daily life. And aren't improving despite dose adjustments and management strategies.
- ✓Your blood sugar control needs aren't being fully met on semaglutide alone. Tirzepatide's dual-receptor action has shown stronger glycemic control in clinical trials.
Stay on semaglutide if:
- →You're still actively losing weight. If semaglutide is working, there is no clinical reason to switch just because tirzepatide averages higher in studies. Averages aren't guarantees.
- →Budget is your primary concern. FDA-approved tirzepatide costs $299–$449/month self-pay.¹ If your current medication is significantly cheaper and still working, switching purely for marginal improvement may not justify the cost increase.
- →You had limited response to semaglutide at adequate doses. Some people have a limited response to incretin-based medications overall. If you saw minimal results even at adequate doses, tirzepatide may offer some improvement — but set realistic expectations.
The part most switching guides won’t tell you
Tirzepatide costs more, and you’ll restart at a low dose. That means reduced appetite suppression for the first several weeks while you titrate up. For some people, that temporary dip — combined with higher monthly costs — isn’t worth it, especially if semaglutide is still working.
Why People Are Suddenly Having to Switch Off Compounded Semaglutide
If you’re reading this, you already know something changed. Here’s what happened and why it matters for your next step.
The regulatory shift
The FDA declared the semaglutide injection shortage resolved on February 21, 2025, and the tirzepatide injection shortage resolved on December 19, 2024.4 Those two dates changed everything.
While the drugs were on the shortage list, compounding pharmacies operated under a legal pathway (Section 503A/503B of the Federal Food, Drug, and Cosmetic Act) that allowed them to produce copies. Once shortages were declared resolved, that pathway narrowed significantly.
What followed the shortage resolutions:
- • Refill disruptions and cancellation emails from telehealth providers
- • Price increases as remaining compounders raised rates
- • In March 2026, FDA issued warning letters to more than 30 telehealth companies for misleading marketing of compounded GLP-1 medications5
- • FDA reiterated that compounded drugs are not FDA-approved and are not the same as generic versions of approved drugs5
Why this matters for your switch: For most people in 2026, FDA-approved tirzepatide (Zepbound) should be the default consideration when switching — not routine compounded tirzepatide. LillyDirect self-pay pricing starts at $299/month,1 and the regulatory environment around compounded versions has tightened substantially.
How Tirzepatide Works Differently Than Semaglutide — And Why Switching Often Breaks a Plateau
Understanding the mechanism difference explains why switching often works — and when it won’t.
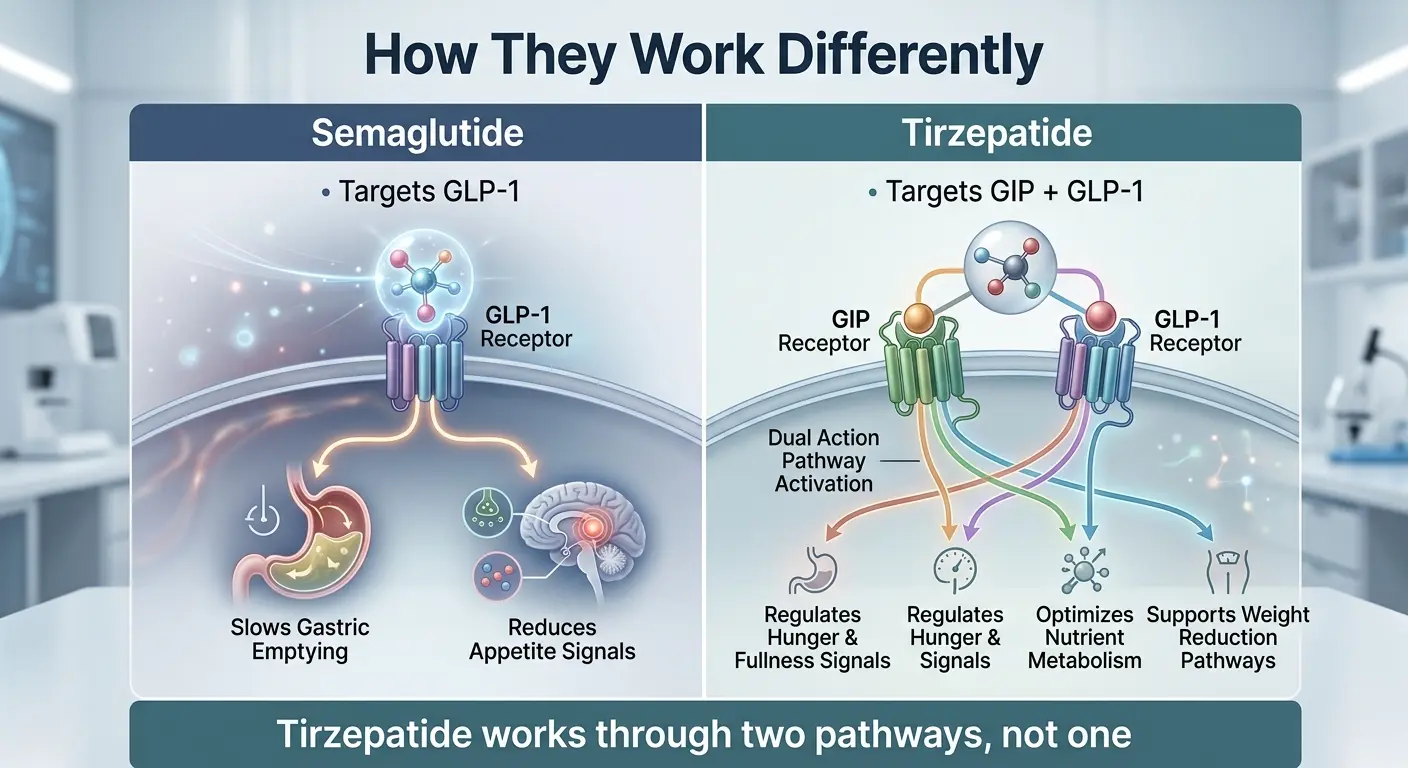
Semaglutide
Activates the GLP-1 receptor only. Suppresses appetite, slows gastric emptying, improves insulin signaling.
Tirzepatide
Activates both GLP-1 and GIP receptors. The dual mechanism is what sets it apart — and why plateau patients often see renewed progress.
What the head-to-head data shows
The strongest evidence comes from the SURMOUNT-5 trial — the first large head-to-head study comparing tirzepatide and semaglutide specifically for weight loss in adults with obesity (without diabetes), published in the New England Journal of Medicine:6
| Outcome | Tirzepatide (up to 15 mg) | Semaglutide (up to 2.4 mg) |
|---|---|---|
| Avg. body weight loss at 72 weeks | ~20.2% | ~13.7% |
A separate matched real-world cohort study of 18,386 patients found tirzepatide users were more likely to achieve 5%, 10%, and 15% weight-loss thresholds and had greater adjusted weight loss at 3, 6, and 12 months.7
The honest caveat
These are population averages. Your individual results depend on dose, duration, genetics, lifestyle, and factors no study can predict for you personally. Some people have a limited response to incretin-based medications overall.
FDA-Approved Tirzepatide via Ro
Check your Zepbound coverage and eligibility
Ro offers Zepbound through online prescribing and includes an insurance coverage checker at no cost. The first month starts at $45 (+ medication cost). If you’re switching from compounded semaglutide and need a new prescriber, Ro is a direct path to FDA-approved tirzepatide.
Check Zepbound eligibility on Ro →The 4-Step Switching Protocol Most Clinicians Use
Here’s the actual process. It’s more straightforward than most people expect.
Take your last compounded semaglutide injection as scheduled
No taper needed. Semaglutide has a half-life of about one week, which means it naturally clears your system gradually after your last dose.9
Document everything from your vial label
This is the step most guides skip — and it’s the most important one for people coming from compounded semaglutide. Before your vial is empty or discarded, capture:
- •Concentration (mg/mL on the label)
- •Total volume of the vial
- •Your weekly dose — in mg if you know it, in units if that's what you were told
- •Syringe type and markings you've been using
- •Additives (B12, L-carnitine, etc.)
- •Pharmacy name from the label
- •Date of your last injection
Take a photo of the vial label. You’ll bring this to your prescriber.
Start tirzepatide on your next injection day
Most clinicians recommend starting tirzepatide about 7 days after your last semaglutide dose — on what would have been your next scheduled injection day.
Titrate gradually under prescriber guidance
Standard titration: 2.5 mg → 5 mg → 7.5 mg → 10 mg → 12.5 mg → 15 mg, with dose increases every 4 weeks based on appetite suppression, weight loss progress, and tolerability.3 Your prescriber will adjust the pace based on your response.
Appointment prep checklist
- ☐Photo of compounded semaglutide vial label
- ☐Your weekly dose (mg and/or units)
- ☐Date of last injection
- ☐Side effects you experienced on semaglutide
- ☐Weight loss timeline and any plateau history
- ☐Insurance card (front and back) or cash-pay budget
- ☐List of other medications and supplements
Do You Need a Washout Period Between Semaglutide and Tirzepatide?
Usually, no. Semaglutide’s half-life is approximately 7 days.9 After your last injection, the drug level naturally declines. By the time your next injection day arrives — roughly one week later — you’re at a natural transition point. That’s why most clinicians don’t require a separate washout period.
Some providers may suggest waiting 10–14 days if you experienced severe GI side effects on semaglutide, are coming off a very high compounded dose, or have specific health conditions that warrant extra caution. For most people, though: last semaglutide dose → wait one week → first tirzepatide dose.
A longer gap between medications often creates more risk than a clean handoff — you lose the appetite-suppressing and metabolic effects you’ve built up, making it harder to maintain progress during the transition.
Is There a Semaglutide-to-Tirzepatide Conversion Chart?
There is no validated, official dose-equivalence chart between semaglutide and tirzepatide — not from the FDA, not from Eli Lilly, not from Novo Nordisk. Any website publishing a confident mg-to-mg crosswalk is offering false precision in a space where it doesn’t exist.
- ✗They work through different receptor pathways. Semaglutide is GLP-1 only. Tirzepatide is dual GLP-1/GIP. The milligram numbers are not interchangeable.
- ✗Compounded vials make this worse. Compounded semaglutide comes in varying concentrations. One vial might be 1 mg/mL, another 5 mg/mL. The dose you've been taking in 'units' could mean very different actual milligrams depending on concentration.
- ✗FDA has documented the danger. The FDA issued a specific alert about dosing errors with compounded semaglutide, including cases where patients took many times the intended dose due to confusion around units, concentrations, and self-measurement.¹⁰
| ❌ Unsafe internet habit | ✅ Safe clinician handoff |
|---|---|
| “I was on 30 units of sema, what’s the tirz equivalent?” | “Here’s my vial label showing concentration, my syringe markings, and my last injection date” |
| Google a conversion chart and self-dose | Schedule a prescriber visit and bring documentation |
| Assume higher sema dose = higher tirz starting dose | Start at the labeled 2.5 mg and titrate based on response |
What If Your Compounded Semaglutide Was Labeled in Units, mL, or Mixed With B12?
This is the gap that generic switching guides don’t address — and it’s the reality for many people on compounded semaglutide.
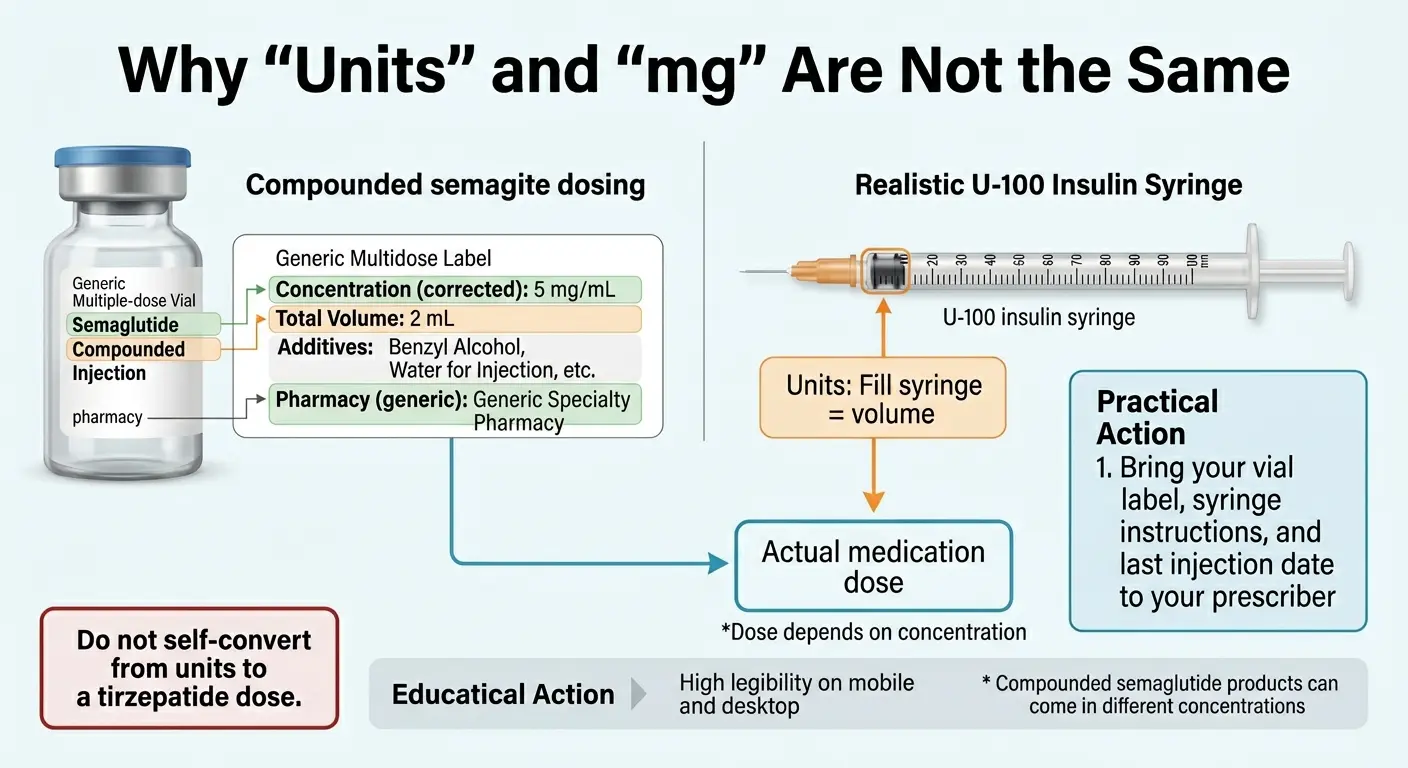
The units problem
Many compounding pharmacies instructed patients to dose in “units” on an insulin syringe rather than milligrams. “30 units” on an insulin syringe means 0.3 mL of liquid. If your vial is 2.5 mg/mL, that’s 0.75 mg. If your vial is 5 mg/mL, that’s 1.5 mg — double the dose from the same “30 units.” This is exactly the kind of confusion that has led to serious dosing errors and hospitalizations.10
What your vial label should show
- •Drug name: Semaglutide (possibly with additives like B12 or L-carnitine)
- •Concentration: Listed as mg/mL (e.g., '2.5 mg/mL' or '5 mg/mL')
- •Total volume: How many mL are in the vial
- •Pharmacy name and contact info
- •Beyond-use date (expiration)
What about B12 and other additives? These don’t change your semaglutide dose, but they’re worth mentioning to your prescriber — they confirm you were on a compounded product, and some additives can affect injection site reactions.
What to Bring to Your Prescriber Before You Switch
This section is your action engine. Everything above gave you knowledge. This gives you what to do with it.

Your exact vial label
Photo or the physical vial. This tells your prescriber the concentration, pharmacy source, and any additives.
Your dose in milligrams
Not just '30 units.' If you don't know your mg dose, your prescriber can calculate it from the vial concentration and volume drawn. Formula: dose (mg) = concentration (mg/mL) × volume drawn (mL).
Your last injection date
The specific day.
Your side-effect history
What you experienced, how severe, what helped. This directly affects your tirzepatide starting dose decision.
Your weight and plateau timeline
Starting weight, current weight, when progress stalled, how long. Brings objective data to the conversation.
Your insurance card or budget limit
Your prescriber can't help optimize your access path without knowing what you can afford.
Your other medications
Complete list including supplements.
Questions to ask your prescriber
- • “Based on my semaglutide dose and tolerance, do you recommend starting tirzepatide at 2.5 mg or 5 mg?”
- • “Should I use LillyDirect, go through my pharmacy, or try insurance first?”
- • “What should I do if nausea gets severe during titration?”
- • “When should I schedule my follow-up?”
What to Expect During the Transition
The first month on tirzepatide is primarily an initiation period. Because you’re beginning at 2.5 mg regardless of your previous semaglutide dose, the first few weeks may feel like a step back — particularly if you were on a high dose. Appetite suppression may be less noticeable than what you’re used to. That’s normal at a starter dose, and it builds as you titrate up.
GI side effects — nausea, diarrhea, constipation, abdominal discomfort — are common during initiation. The Zepbound label notes these generally decreased over time.3 Many people who’ve been on semaglutide report the adjustment feels milder than when they first started GLP-1 therapy — though individual experiences vary.
As you reach higher therapeutic doses (typically 7.5 mg and above), the dual GLP-1/GIP mechanism is more fully engaged. This is when most people begin to see meaningful differences in appetite control and weight trajectory compared to their semaglutide experience.
What might not go as planned
- →If you had limited response to semaglutide at adequate doses, tirzepatide may offer some improvement — but likely won’t transform your results.
- →Muscle loss is a risk with both medications. Resistance training and adequate protein (at least 0.7–1.0 g/lb body weight daily) are essential.
- →Psychological eating patterns don’t always change. These medications reduce physical hunger, but stress eating and ingrained habits can persist.
Side Effects: What Changes When You Switch
The side effect profile is similar to what you experienced starting semaglutide. The Zepbound label lists these as common: nausea, diarrhea, vomiting, constipation, abdominal pain, indigestion, injection site reactions, fatigue, belching, hair loss, and heartburn.3
Call your prescriber immediately for:
- • Severe, persistent abdominal pain (possible pancreatitis)
- • Signs of allergic reaction — rash, swelling, difficulty breathing
- • Significant mood changes, depression, or suicidal thoughts
- • Vision changes (especially if you have type 2 diabetes)
Practical management tips
- •Eat smaller, more frequent meals during the first 2–4 weeks
- •Stay aggressively hydrated — aim for 80+ oz of water daily
- •Take your injection in the evening if nausea is bothersome
- •Avoid high-fat and high-sugar meals, which tend to worsen GI symptoms
How Much Does Switching to Tirzepatide Cost in 2026?
Let’s be direct about the money. For many people, switching means paying more than they were on compounded semaglutide.
Zepbound self-pay pricing through LillyDirect
| Dose | Self-pay | Journey Program* |
|---|---|---|
| 2.5 mg (starting) | $299/month | $299/month |
| 5 mg | $399/month | $399/month |
| 7.5 mg | $499/month | $449/month |
| 10 mg | $699/month | $449/month |
| 12.5 mg | $699/month | $449/month |
| 15 mg | $699/month | $449/month |
*Journey Program price requires refilling within 45 days of previous delivery. Prices verified April 2026 via zepbound.lilly.com/savings.1
How to minimize costs
- 1.Check insurance first. Call the number on the back of your card and ask specifically about tirzepatide (Zepbound) coverage for weight management. Some plans that denied semaglutide do cover tirzepatide.
- 2.Use the Zepbound savings card at zepbound.lilly.com/savings for eligible commercially insured patients.2
- 3.Ask about the OSA indication if you have documented sleep apnea and obesity — separate coverage pathway for some plans.
- 4.Consider LillyDirect first if you already have a prescriber — cutting out a telehealth membership fee saves money.
- 5.HSA/FSA reimbursement may be available, though coverage rules vary. Check with your plan administrator before assuming eligibility.
Which Access Path Is Best for You?
Not everyone should take the same route. Here’s how to think through it.
Best if you already have a prescriber
Existing prescriber + LillyDirect or local pharmacy
Your doctor can prescribe Zepbound directly. Fill it through LillyDirect for self-pay pricing ($299–$449/month with home delivery or Walmart pickup) or through your pharmacy with insurance.1 This is often the cheapest and fastest path because you’re not paying a separate telehealth membership fee.
Best if you need a new prescriber or insurance navigation
Ro Body Program — FDA-approved Zepbound
Ro offers FDA-approved Zepbound with integrated telehealth, insurance navigation, and a free GLP-1 insurance coverage checker.11 The tradeoff: Ro charges $45 for the first month and $145/month ongoing — separate from medication cost. If you need help getting prescribed and navigating insurance, the all-in-one workflow can be worth the premium — especially if their insurance checker finds coverage that makes tirzepatide affordable.
“I love the fact that I was able to do this from the comfort of my home.” — Ro patient via TrustpilotCheck Zepbound coverage and eligibility on Ro →
If cost is your absolute first filter
Start with the insurance path
If you don’t have coverage, LillyDirect self-pay ($299/month starting dose) is the most transparent option without hidden membership fees.1 If FDA-approved tirzepatide is genuinely outside your budget, talk to your prescriber about FDA-approved semaglutide (Wegovy) or Novo Nordisk’s patient assistance programs.
Still deciding between Wegovy and Zepbound? If your issue was compounded supply reliability rather than a plateau, moving to FDA-approved Wegovy could solve the problem without changing medications. See our Wegovy access guide →
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
Will You Regain Weight During the Switch?
A short, planned transition usually does not mean starting over — especially because semaglutide has a long half-life of about one week.9 The 7-day gap between your last semaglutide injection and your first tirzepatide dose keeps you within that pharmacological window.
You may see a small fluctuation in the first few weeks from water retention changes and food volume shifts as the starter dose provides less appetite suppression than your previous sema dose. This is not the same as fat regain.
The bigger risk is procrastination
A multi-week gap with no medication — because you waited too long to arrange the transition — is a much more likely cause of lost progress than a clean, clinician-guided handoff. Start planning your switch before you run out of compounded semaglutide, not after.
What You Should NOT Do During the Switch
These are the specific mistakes that send people back to searching for help.
Do not take semaglutide and tirzepatide at the same time
The Zepbound prescribing information states that coadministration with another GLP-1 receptor agonist is not recommended.³ This isn't a suggestion — it's a labeled instruction.
Do not 'finish the vial' after starting tirzepatide
If you have leftover compounded semaglutide, do not inject it alongside or between tirzepatide doses. Use a drug take-back or mail-back option when available, and dispose of needles in a sharps container.¹²
Do not self-convert your dose using internet charts
Bring your label to your prescriber. Let them determine your starting dose. This is the single highest-risk mistake in the entire process.
Do not assume compounded tirzepatide is the default next step in 2026
The semaglutide and tirzepatide shortages have been resolved.⁴ More than 30 telehealth companies received FDA warning letters in 2026 for misleading marketing of compounded GLP-1 products.⁵ For most people, FDA-approved Zepbound is the more straightforward path.
Do not let the process drag until you have a long treatment gap
Start planning your switch while you still have supply remaining.
Is Compounded Tirzepatide Still Available — and Should You Use It?
Compounded tirzepatide is still available through some pharmacies and telehealth platforms. But the landscape has changed significantly:
- •FDA declared the tirzepatide shortage resolved on December 19, 20244
- •The legal pathway for routine compounding narrowed significantly
- •FDA issued warning letters to 30+ telehealth companies in early 2026 for misleading compounded GLP-1 marketing5
- •FDA reminded the public that compounded drugs are not FDA-approved and are not the same as generic drugs5
There are narrow scenarios where compounded tirzepatide may still have a legitimate use case — typically involving a patient-specific need (like an allergy to an inactive ingredient in the branded product), ordered through a licensed prescriber and filled by a reputable 503A pharmacy. This is categorically different from mass-market telehealth platforms selling compounded tirzepatide as a routine alternative to Zepbound.
Our editorial call
For most readers of this guide, FDA-approved Zepbound through LillyDirect, insurance, or a platform like Ro is the stronger path in 2026. The self-pay pricing ($299–$449/month) has come down enough that the cost gap with compounded options is much smaller than it used to be — while the regulatory environment around compounded versions has tightened substantially.1
How We Verified This Page
This is a YMYL (Your Money or Your Life) topic. Here’s where our information comes from.
1 Eli Lilly — Zepbound Self Pay Journey Program pricing — zepbound.lilly.com/savings
2 Eli Lilly — Zepbound savings card terms — lilly.com/lillydirect/medicines/zepbound/savings-card-terms-conditions
3 FDA — Zepbound (tirzepatide) prescribing information (2025 label) — accessdata.fda.gov
4 FDA — Semaglutide and tirzepatide shortage resolution — fda.gov/media/185526/download
5 FDA — Compounding policy and telehealth warning letters — fda.gov/drugs/drug-alerts-and-statements
6 SURMOUNT-5 trial, New England Journal of Medicine — DOI: 10.1056/NEJMoa2416394
7 Real-world tirzepatide vs semaglutide outcomes, JAMA Internal Medicine — jamanetwork.com/journals/jamainternalmedicine/fullarticle/2821080
8 Prospective GLP-1 to tirzepatide switching study — PubMed ID 38723893
9 FDA — Wegovy (semaglutide) prescribing information, pharmacokinetics — accessdata.fda.gov
10 FDA — Alert on dosing errors with compounded semaglutide — fda.gov/drugs/human-drug-compounding
11 Ro — Weight loss pricing and program details — ro.co/weight-loss/pricing
12 FDA — Safe disposal of unused medicines — fda.gov/drugs/safe-disposal-medicines
What this page does NOT claim:
- • We do not claim compounded and FDA-approved medications are interchangeable
- • We do not claim any specific weight loss result for any individual
- • We do not provide medical advice — decisions to switch should be made with a licensed prescriber
- • We do not claim any conversion chart between semaglutide and tirzepatide is validated
Frequently Asked Questions
Can you switch from compounded semaglutide to tirzepatide?
Yes. Most people can switch with prescriber guidance. The common approach is to take your last semaglutide dose, wait about 7 days (your next injection day), and start tirzepatide at 2.5 mg weekly. Always do this under clinical supervision — not based on internet dosing advice.
Do you need to taper off or wash out semaglutide first?
Usually not. Semaglutide's long half-life of approximately 7 days means it naturally clears after your last injection. Most clinicians time the switch to your next injection day. A longer washout may be recommended if you experienced severe side effects or are on a very high dose.
Can you take semaglutide and tirzepatide at the same time?
No. The Zepbound prescribing information states that coadministration with another GLP-1 receptor agonist is not recommended.
What dose of tirzepatide should I start on after semaglutide?
The labeled starting dose of Zepbound is 2.5 mg once weekly for 4 weeks, regardless of your previous semaglutide dose. Some clinicians may individualize the starting dose for GLP-1-experienced patients — but this is their call, not yours.
Is there a semaglutide-to-tirzepatide conversion chart?
No validated conversion chart exists. The medications work through different receptor pathways, making direct mg-to-mg conversion scientifically unsound. Compounded semaglutide's varying concentrations make internet charts even more unreliable and potentially dangerous.
What if my compounded semaglutide dose was listed in units instead of mg?
Do not self-convert from units. Units on an insulin syringe represent volume (mL), and the actual drug dose depends on your vial's concentration. Bring your exact vial label and syringe instructions to a licensed prescriber.
What should I do with leftover compounded semaglutide?
Do not continue using it after starting tirzepatide. Use a drug take-back or mail-back option when available, and dispose of needles and syringes in an appropriate sharps container following FDA guidance.
Will I regain weight if there is a gap between medications?
A short, planned transition usually does not mean starting over. Semaglutide's long half-life means it still provides some effect during the 7-day handoff window. The bigger risk is an unplanned multi-week gap — which is why starting the process before you run out is important.
Is compounded tirzepatide still available in 2026?
The legal landscape has narrowed significantly since the tirzepatide shortage was declared resolved in December 2024. Routine mass-market compounding faces increased regulatory scrutiny. For most people, FDA-approved Zepbound is the more straightforward and reliable path.
How long until I see results after switching to tirzepatide?
Response timing varies. Because tirzepatide is started at a low dose and titrated gradually, the first month is primarily an initiation period. Meaningful changes typically depend on reaching a therapeutic dose through titration over several weeks, not the first few injections.
Still not sure which GLP-1 program is right for you?
Answer 6 questions and get matched with the access path that fits your budget, goals, and situation — not a one-size-fits-all recommendation.
This article is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before starting, stopping, or switching any medication. Some links on this page are affiliate links — we may earn a commission at no extra cost to you. This does not affect our editorial recommendations. Affiliate disclosure · Editorial standards
Related guides
- How to Switch From Compounded Tirzepatide to Mounjaro (2026)
- How to Switch From Semaglutide to Zepbound: 5 Steps, Doses & Real Cost (2026)
- How to Switch From Semaglutide to Mounjaro (2026): Timing, Doses, Cost
- How to Get GLP-1 Without Insurance in 2026: Real Prices [Verified]
- Switch Compounded Semaglutide to Zepbound (2026)