How to Switch From Compounded Semaglutide to Zepbound (2026 Guide)
By The RX Index Editorial Team · Last verified: April 1, 2026
Medical disclaimer: This article is for informational purposes only and is not medical advice. Zepbound (tirzepatide) is a prescription medication. Always work with a licensed healthcare provider before starting, stopping, or switching any medication.
If your compounded semaglutide is ending — or you've plateaued and you're ready for something stronger — here's how to switch from compounded semaglutide to Zepbound safely.
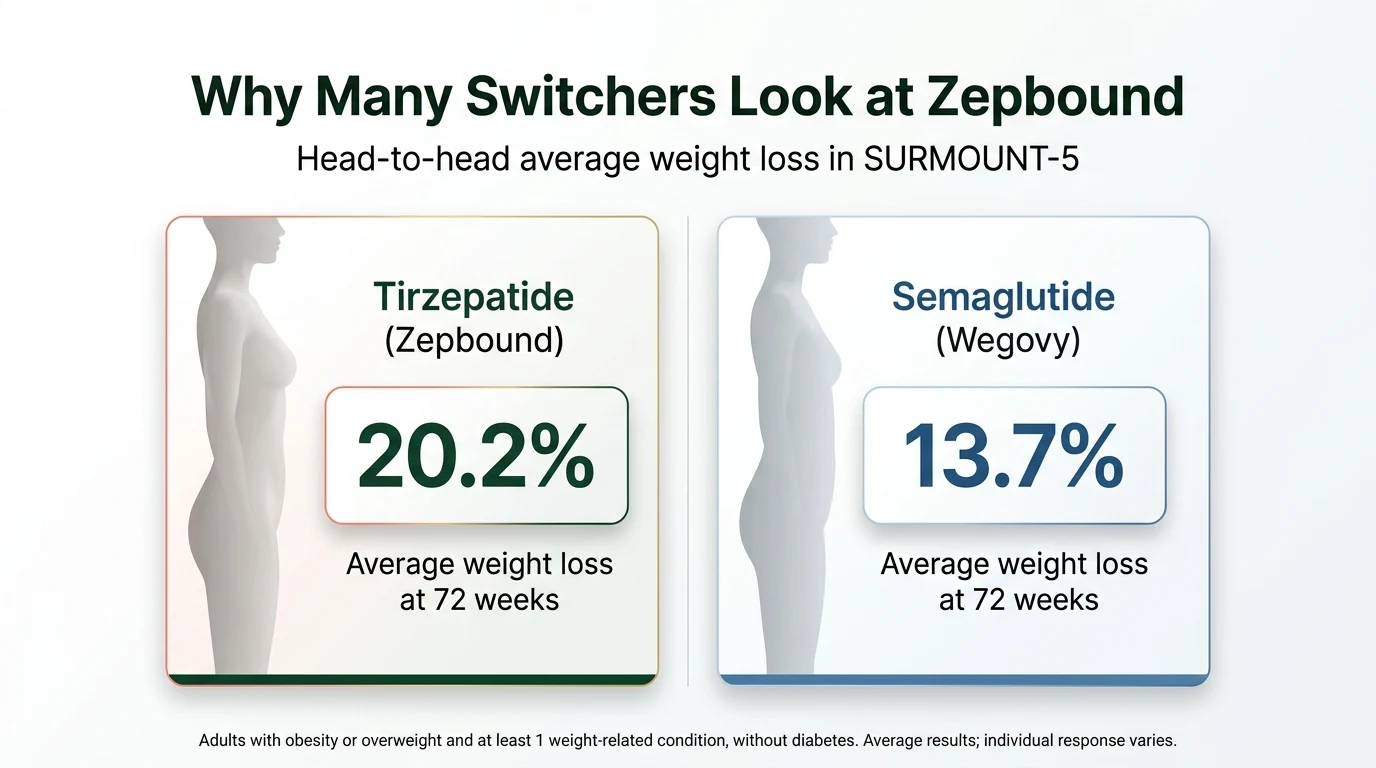
Many patients can make this transition with prescriber guidance. And the clinical evidence may surprise you: tirzepatide (Zepbound) has produced significantly greater average weight loss than semaglutide in both head-to-head trials and large real-world studies — though individual response varies.
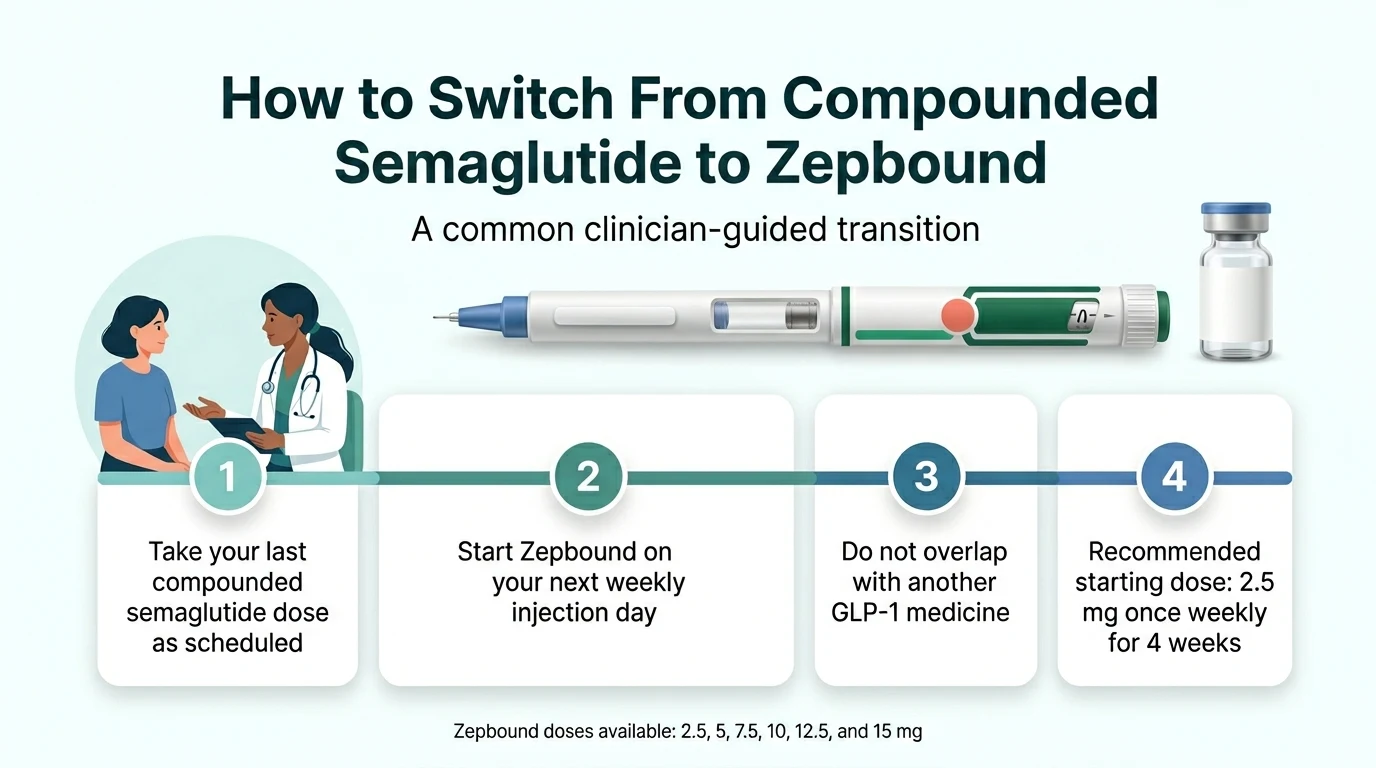
The common clinician-guided approach: take your last compounded semaglutide dose as scheduled, then start Zepbound on your next weekly injection day. The labeled starting dose is 2.5 mg weekly. Some GLP-1–experienced patients are started at 5 mg by their prescriber. Do not overlap Zepbound with another GLP-1 medication.
There is no validated milligram-for-milligram conversion chart between semaglutide and tirzepatide. Anyone telling you otherwise is guessing.
The cost question everyone asks: Zepbound starts at $299/month through LillyDirect self-pay vials, or as low as $25/month for eligible patients with commercial insurance coverage and a Zepbound Savings Card. Those numbers are current as of April 2026.
Quick-reference answers
| Question | Answer |
|---|---|
| Can you switch? | Yes, with prescriber guidance |
| Can you overlap the two medications? | No — coadministration with another GLP-1 receptor agonist is not recommended per the Zepbound label |
| Is there a 1:1 dose conversion? | No validated conversion chart exists |
| When to start Zepbound | A common approach is your next weekly injection day, as directed by your prescriber |
| Starting dose | 2.5 mg weekly; some prescribers start GLP-1–experienced patients at 5 mg |
| Current cash price | $299/mo (2.5 mg), $399/mo (5 mg), $449/mo (7.5–15 mg) via LillyDirect |
| With commercial insurance | As low as $25/mo for eligible patients with coverage and a Savings Card |
Sources: Zepbound prescribing information (FDA), LillyDirect pricing page, Zepbound Savings Card terms — all verified April 2026.

Why Is Compounded Semaglutide Going Away?
You're not imagining it. If your compounded semaglutide supply is drying up — or your provider told you they can't refill — here's why.
The FDA declared the semaglutide injection shortage resolved on February 21, 2025. That ended the shortage-based pathway many compounding pharmacies had relied on for products that were essentially copies of Ozempic and Wegovy.
The enforcement timeline moved fast. The FDA's grace period for 503A state-licensed pharmacies expired April 22, 2025. For 503B outsourcing facilities, the deadline was May 22, 2025. A federal court upheld the FDA's decision.
As of April 2026, narrow patient-specific 503A exceptions can still exist when a prescriber documents a significant clinical difference for an identified patient — such as a verified allergy to an inactive ingredient in the branded product. But cost or convenience alone does not qualify. Routine mass-compounding of semaglutide copies is effectively over.
Why Zepbound? (This May Be a Better Fit Than You Expect)
Here's the part nobody's telling you clearly enough: switching from compounded semaglutide to Zepbound isn't settling. For many people, it's a step up.
Semaglutide
A GLP-1 receptor agonist. Mimics one gut hormone to help control appetite and blood sugar. That's why it worked for you.
Tirzepatide (Zepbound)
A GIP and GLP-1 receptor agonist. Activates two receptor types instead of one — a dual-action approach with stronger average results in clinical trials.
The data backs this up. A large real-world study of over 18,000 patients found:
| Timeframe | Tirzepatide (Zepbound) | Semaglutide |
|---|---|---|
| 3 months | 5.9% of body weight | 3.6% |
| 6 months | 10.1% | 5.8% |
| 12 months | 15.3% | 8.3% |
Source: Rodriguez PJ, et al. Retrospective cohort analysis, JAMA Internal Medicine, 2024. Individual results vary.
Zepbound also carries FDA approval, meaning every vial meets standardized potency, purity, and manufacturing requirements that compounded products don't undergo. That consistency matters when you're injecting something weekly.
The honest tradeoff: Zepbound costs more than compounded semaglutide did. If you were paying $150–$250 a month for compounded, your costs will increase. We break down every pricing path in detail below — and the gap is smaller than most people expect — but we're not going to pretend the cost is identical. What we can say: the clinical evidence for greater average weight loss and the regulatory certainty are on a different level.
For everyone else — especially if you've plateaued on semaglutide or have meaningful weight still to lose — Zepbound is the strongest FDA-approved option available today.
How to Switch From Compounded Semaglutide to Zepbound: Step by Step
We reviewed the FDA prescribing information, published GLP-1 switching guidance, and real clinician protocols to put this together.
Take Your Last Compounded Semaglutide Dose as Scheduled
No need to taper. Simply take your final compounded semaglutide injection on your regular schedule and note the date.
Semaglutide has a long half-life — roughly 7 days — which means it stays active in your system for weeks after your last injection, declining gradually. That built-in buffer works in your favor during the transition.
Start Zepbound on Your Next Scheduled Injection Day
A common clinician-guided approach is to start Zepbound approximately one week after your last semaglutide dose — on your next regular injection day. This avoids stacking two GLP-1 medications.
If you had significant GI side effects at your last semaglutide dose, your prescriber may want to wait until those symptoms fully clear. That's a clinical judgment call.
Start at the Labeled Dose — 2.5 mg Weekly
This surprises a lot of people. You might have been on 2.0 mg or 2.4 mg of semaglutide — the highest branded dose — and now you're starting Zepbound at what looks like a tiny 2.5 mg.
Here's why: there is no validated semaglutide-to-tirzepatide conversion chart. The medications work through different receptor mechanisms, and the milligram numbers aren't interchangeable. Starting at 2.5 mg isn't a step backward — it's how Zepbound is designed to be initiated.
The 2.5 mg dose is explicitly an initiation dose, not a maintenance dose. It exists to let your body adjust to tirzepatide's dual receptor activity before stepping up. Some prescribers start selected patients at 5 mg — particularly those who tolerated semaglutide well — but that's a clinical conversation.
Titrate Up Every 4+ Weeks
The official Zepbound dose escalation:
| Weeks | Dose | Purpose |
|---|---|---|
| Weeks 1–4 | 2.5 mg | Initiation — adjusting to the medication |
| Weeks 5–8 | 5 mg | First therapeutic dose |
| Weeks 9–12 | 7.5 mg | Continued escalation if tolerated |
| Weeks 13–16 | 10 mg | Stronger appetite suppression |
| Weeks 17–20 | 12.5 mg | Approaching maximum dose |
| Week 21+ | 15 mg | Maximum labeled dose |
Source: Zepbound FDA prescribing information. You don't have to reach 15 mg. Many people find their maintenance dose at 10 or 12.5 mg.

Stay in Touch With Your Provider
Track your weight, appetite, side effects, and energy levels. Your prescriber adjusts your dose based on your individual response. If you're doing well at 7.5 mg, there's no obligation to go higher.
Report anything that concerns you — persistent nausea, significant GI distress, or anything that feels notably different from what you experienced on semaglutide.
You've already done the hardest part — starting GLP-1 treatment and sticking with it. Switching to Zepbound is the next step in a journey you've already committed to.
Is There a Semaglutide to Zepbound Conversion Chart?
No. And any page that presents one as “official” is misleading you.
No pharmaceutical manufacturer, FDA document, or peer-reviewed study provides a validated milligram-for-milligram mapping between semaglutide and tirzepatide. The drugs activate different receptor combinations, so their doses aren't interchangeable.
What prescribers use instead: your tolerance history, side-effect profile, remaining weight-loss goals, and clinical judgment. That's why the standard practice is to start at 2.5 mg and titrate based on individual response.
What to Bring to Your Prescriber Instead of a Conversion Chart
Rather than trying to match milligrams, prepare this for your prescriber conversation:
| Information to Bring | Why It Matters |
|---|---|
| Your exact compounded semaglutide concentration and weekly dose | Compounded vials vary by pharmacy — concentration ≠ dose |
| Date of your last injection | Determines safe timing for starting Zepbound |
| Side-effect history on semaglutide | Guides whether to start at 2.5 mg or 5 mg |
| Your weight trend (losing, maintaining, plateaued) | Informs titration pace and dose goals |
| Insurance status and plan details | Determines which access path saves you the most |
| What you plan to do with leftover compounded supply | Prescriber needs to counsel against overlap |
What You Should NOT Do During the Switch
This section exists because real people make these mistakes.
✗ Do not take compounded semaglutide and Zepbound together
The Zepbound label explicitly recommends against coadministration with another GLP-1 receptor agonist.
✗ Do not do your own dose conversion math
"I was on 1.7 mg semaglutide, so I'll start at 7.5 mg tirzepatide" — this logic doesn't hold. The milligram numbers operate on completely different scales with different receptor mechanisms. Let your prescriber choose.
✗ Do not wait until you run out of compounded supply to start the process
Getting a Zepbound prescription, navigating insurance, or setting up LillyDirect takes time. Start planning before your last refill so you avoid a treatment gap. A treatment gap is the single biggest risk factor for appetite return and weight regain during a switch.
✗ Do not assume your compounded vial concentration maps onto Zepbound
Compounded semaglutide comes in various concentrations depending on the pharmacy. One more reason a prescriber needs to assess you individually.
What Does Zepbound Actually Cost in 2026?
Cost is the reason most people hesitate. Here are verified numbers across every access path.
| How You're Getting Zepbound | Monthly Cost |
|---|---|
| Commercial insurance + Savings Card (with Zepbound coverage) | As low as $25/mo |
| Commercial insurance + Savings Card (without Zepbound coverage) | $499/mo |
| LillyDirect self-pay vials | $299/mo (2.5 mg), $399/mo (5 mg), $449/mo (7.5–15 mg) |
| Ro Body Program | Vial pricing + $145/mo membership ($45 first month) |
| MEDVi brand path | $99/mo membership + medication at pharmacy/LillyDirect pricing |
| Retail pharmacy, no discount | ~$1,050–$1,086/mo |
All prices verified April 2026. Savings Card valid through 12/31/2026.
Savings Card fine print: The $25/month price applies to eligible commercially insured patients whose plan covers Zepbound single-dose pens. Maximum monthly savings of $100, with a $1,300 annual cap. Medicare, Medicaid, and government program beneficiaries are not eligible.
LillyDirect refill timing: If you're on 7.5 mg or higher and don't refill within 45 days of your previous delivery, the $449 discounted price no longer applies. Post-window pricing: $499 for 7.5 mg, $699 for 10–15 mg. Set a calendar reminder.
Medicare: CMS's Medicare GLP-1 Bridge program runs from July 1, 2026 through December 31, 2026. Eligible beneficiaries pay a $50 copay. If you're on Medicare, use LillyDirect vials in the interim.
HSA/FSA: Zepbound qualifies for payment through health savings accounts and flexible spending accounts.
Compared to what you were paying: Most people on compounded semaglutide paid $150–$300 per month. LillyDirect vials at $299 for the starting dose put branded Zepbound in a similar range. It's not identical pricing, but it's far from the $1,086 sticker shock most people imagine.
Where to Get a Zepbound Prescription (3 Paths)
You've decided to switch. Now you need the actual prescription. Here are your options, ranked by what makes the most sense for someone switching from compounded semaglutide.
Path 1: Ro — Best for Insurance Navigation and Full-Service Support
Ro's Body Program is the most complete telehealth path to Zepbound for someone switching from compounded. Here's why it matters specifically for you:
Insurance concierge. Ro's team checks whether your insurance covers Zepbound, handles prior authorization, and works to get coverage before defaulting to cash-pay. If you've never navigated a branded GLP-1 through insurance — and most people switching from compounded haven't — this alone can save you hundreds per month.
LillyDirect integration. If cash-pay is your path, Ro facilitates Zepbound vials through LillyDirect at the $299–$449 pricing.
Ongoing provider care. A licensed prescriber manages your titration, monitors your progress, and adjusts your plan — not a one-and-done prescription.
Cost: $45 first month, then $145/month membership + medication cost.
Speed: Eligibility review within 2 days. Cash-pay starts can arrive in less than a week. Insurance typically takes 2–3 weeks due to prior authorization.
If they get Zepbound covered at $25/month instead of $299+, you recoup the membership fee many times over.
Path 2: MEDVi — Lower Membership Fee, Flexible Provider Access
MEDVi has expanded into FDA-approved brand-name prescriptions including Zepbound, Wegovy, and Mounjaro. Their brand path: a $99/month membership gets you access to a licensed provider who can prescribe FDA-approved medications, which you fill through a pharmacy or LillyDirect.
Best for: Budget-conscious switchers who want provider oversight but don't need the full coaching and insurance concierge Ro includes. If you already know your insurance doesn't cover Zepbound and you're going cash-pay, the $46/month savings on the membership adds up.
Not ideal for: If insurance navigation matters to you, Ro's concierge service is more robust.
MEDVi carries a 4.4–4.5 rating on Trustpilot from over 11,000 reviews. Verify current membership terms directly on their site before enrolling, as offerings can change.
Path 3: Your Own Doctor + LillyDirect
Already have a PCP, endocrinologist, or obesity medicine specialist? They can prescribe Zepbound directly and send the prescription to LillyDirect for self-pay vials. No telehealth membership needed. No middleman fees.
This path makes the most sense if you have a prescriber you trust, don't need insurance help, and want the lowest total cost.
Quick Decision Guide
| Your Situation | Best Path |
|---|---|
| Commercial insurance, not sure if Zepbound is covered | Ro |
| No insurance, want provider support and coaching | Ro |
| No insurance, want lowest membership fee | MEDVi |
| Already have your own prescriber | LillyDirect direct |
| On Medicare | LillyDirect vials now; CMS GLP-1 Bridge from July 2026 |
| Not sure Zepbound is right for you | Take our quiz |
What to Expect Week by Week After the Switch
This section stops people from panicking when the first week doesn't match expectations.
Week 1 (2.5 mg — Your First Zepbound Dose)
Mild nausea is the most common early symptom. You may also notice reduced appetite, slight fatigue, or mild stomach discomfort. Semaglutide is still partially active in your system — its long half-life creates a buffer where residual GLP-1 activity overlaps while tirzepatide begins building. Many people tolerate this first week better than they expect.
Drink at least 64–80 oz of water daily. Eat smaller, protein-forward meals. Avoid greasy or heavy foods. Keep anti-nausea basics on hand (ginger tea, bland crackers).
Weeks 2–4 (Still on 2.5 mg)
GI symptoms typically stabilize. Many report appetite suppression becoming noticeable. Residual semaglutide has largely declined, and tirzepatide is doing the primary work. Some people lose 2–5 pounds during the initiation phase. Others don't see meaningful scale movement until the dose increases. Both responses are normal.
"2.5 mg feels weaker than what I was on" is expected. This is an initiation dose. The real momentum builds as you step up.
Weeks 5–8 (5 mg — First Therapeutic Dose)
This is where many people feel the switch start to click. The dual GLP-1 + GIP receptor activity starts showing its strength. Many report deeper appetite suppression and quieter food noise — especially evening cravings. A brief return of mild GI symptoms is possible as your body adjusts to the higher dose. These typically resolve within a few days.
Months 3–6 (Titrating to Your Maintenance Dose)
Most people find their maintenance dose between 7.5 mg and 15 mg. Weight loss of 1–2 pounds per week is typical during active titration. Your prescriber adjusts based on appetite control, side effects, and progress. This is when the clinical advantage of tirzepatide over semaglutide tends to show most clearly.
Will I Regain the Weight I Lost on Semaglutide?
This is the fear behind the search. Let's address it directly.
A short, planned handoff is far less likely to feel abrupt than a prolonged treatment gap. Semaglutide has a half-life of approximately 7 days. When you start Zepbound approximately one week later, you're not going from “medicated” to “unmedicated” — you're bridging from one GLP-1 medication to a dual-receptor agonist while residual semaglutide is still declining.
The real risk factor isn't the switch itself — it's a prolonged gap between medications. If you stop compounded semaglutide and wait weeks or months to start Zepbound, appetite return and some weight regain become more likely.
Is It Worth Switching If You've Plateaued?
If you've been on compounded semaglutide for months, the weight loss has stalled, and you still have meaningful weight to lose — this is one of the strongest reasons to consider switching.
Tirzepatide's dual receptor mechanism offers a different approach. By activating GIP receptors that semaglutide doesn't target, Zepbound can push through plateaus that semaglutide alone couldn't resolve. The SURMOUNT-5 trial, published in the New England Journal of Medicine in 2025, demonstrated that tirzepatide produced significantly greater weight loss than semaglutide in adults with obesity over 72 weeks.
If you've plateaued, still have weight to lose, and can manage the pricing outlined above — Zepbound is the strongest clinical option available today.
Who Should NOT Switch to Zepbound
We'd rather lose you from this page than have you make an unsafe choice. If any of the following apply, talk to your prescriber before considering the switch.
Personal or family history of medullary thyroid carcinoma (MTC)
Zepbound carries a boxed warning: it should not be used in patients with a personal or family history of MTC or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
Known serious hypersensitivity to tirzepatide
If you've had a serious allergic reaction to tirzepatide or any ingredient in Zepbound, it's contraindicated.
History of pancreatitis
Zepbound has not been studied in patients with a history of pancreatitis. Discuss this with your prescriber.
Pregnancy
Zepbound may cause fetal harm. When pregnancy is recognized, discontinue Zepbound and contact your prescriber.
If none of those apply but you're still unsure, take our 60-second GLP-1 matching quiz — it'll point you in the right direction based on your specific situation.
Common Side Effects During the Switch — and What's a Red Flag
Switching from one GLP-1 medication to another can bring side effects, even if you tolerated semaglutide well.
Common and generally expected
Nausea, diarrhea, constipation, stomach pain, indigestion, decreased appetite, and fatigue. Listed in the Zepbound prescribing information; most noticeable during dose increases and ease as the body adjusts.
When to call your prescriber
Persistent vomiting, signs of dehydration, significant abdominal pain that doesn't resolve, or anything that feels markedly worse than what you experienced on semaglutide.
When to seek urgent care
Symptoms of a serious allergic reaction (swelling of face, lips, tongue, or throat; severe rash; trouble breathing), symptoms of pancreatitis (severe abdominal pain that won't go away), or any sudden change in vision.
Practical first-week approach: Stay hydrated. Eat smaller meals. Avoid heavy, greasy foods. If nausea is manageable, give it a few days — it typically peaks and then fades. If it's interfering with daily life, contact your prescriber before your next dose.
How to Verify That Your Provider and Pharmacy Are Legitimate
If you've been in the compounded world, you know that not every provider or pharmacy operates at the same standard. As you move to branded Zepbound, it's worth taking 60 seconds to verify.
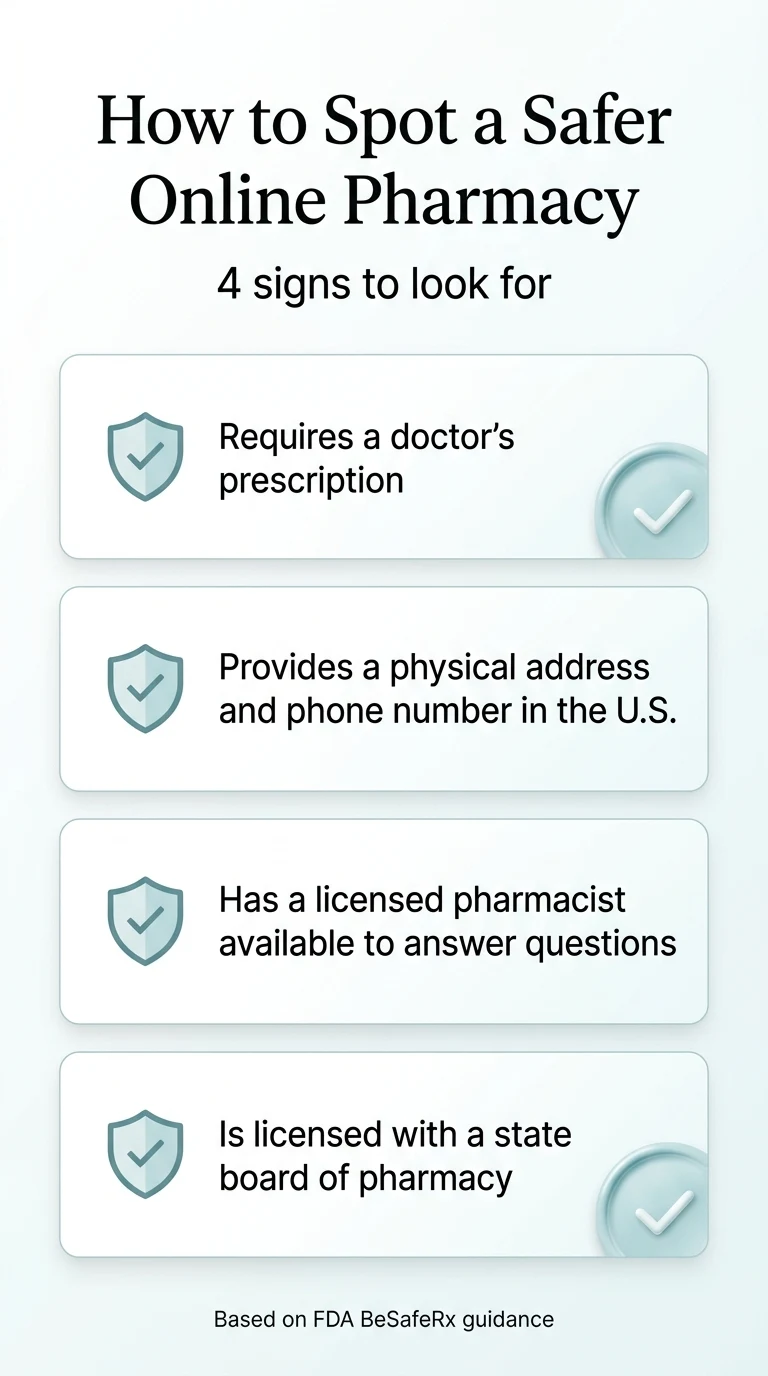
The FDA's BeSafeRx program identifies safe online pharmacy signs: requires a valid prescription, provides a U.S. address and phone number, has a licensed pharmacist available for questions, and is licensed by a state board of pharmacy.
Red flags to avoid
No prescription required. Unusually low pricing with no clear source. “Research use” disclaimers. No physical address or phone number.
LillyDirect (Eli Lilly's official self-pay platform) and Ro are both established, licensed entities. If you're using either, you're on solid ground. For any unfamiliar provider, run them through the NABP verification tool at safe.pharmacy.
Honest Tradeoffs: What You Gain and What Changes
What's better with Zepbound
- FDA-approved — standardized quality controls
- Dual receptor mechanism (GIP + GLP-1)
- Insurance-eligible; potential $25/mo access
- Prefilled pen option available
- Strong clinical evidence base (SURMOUNT trials)
What changes
- Higher price point — from $150–300 to $299+
- Less dosing flexibility (fixed weekly doses)
- Insurance prior authorization may be required
What stays the same
- Weekly injections — same basic routine
- Similar GI side-effect profile
- Ongoing provider oversight required
Methodology: How We Verified This Page
Every factual claim on this page is traceable to a primary source:
- Dosing information: Zepbound FDA prescribing information
- Pricing: LillyDirect pricing page and Zepbound Savings Card terms, verified April 2026
- Clinical trial data: SURMOUNT-5 (NEJM, 2025); Rodriguez PJ, et al. (JAMA Internal Medicine, 2024)
- FDA regulatory timeline: FDA.gov press releases and compounding enforcement guidance
- GLP-1 switching guidance: Almandoz JP, et al. Clinical Diabetes, 2020.
Frequently Asked Questions
Can you take compounded semaglutide and Zepbound at the same time?
No. Zepbound’s prescribing information states that coadministration with another GLP-1 receptor agonist is not recommended. Take your last compounded dose, then start Zepbound on your next scheduled injection day as directed by your prescriber.
How long should I wait between my last semaglutide dose and my first Zepbound dose?
A common clinician-guided approach is to start Zepbound on your next weekly injection day — roughly 7 days after your last semaglutide dose. Your prescriber may adjust this based on your side-effect history or individual circumstances.
What dose of Zepbound should I start on after semaglutide?
The labeled starting dose is 2.5 mg weekly. Some prescribers start GLP-1–experienced patients at 5 mg based on prior tolerance, but this is a clinical judgment call — not a default.
Is there an official semaglutide-to-Zepbound conversion chart?
No. No validated milligram-for-milligram conversion chart exists between semaglutide and tirzepatide. The medications work through different receptor mechanisms and their doses are not interchangeable.
Will 2.5 mg of Zepbound feel weaker than what I was on?
It can, especially in the first few weeks. The 2.5 mg dose is an initiation dose, not a maintenance dose. Appetite suppression and weight loss typically increase as you titrate to higher doses over the following weeks.
Does insurance cover switching to Zepbound?
Coverage varies by plan. Many commercial insurance plans cover Zepbound, often requiring prior authorization. Lilly’s Savings Card can bring the copay to as low as $25/month for eligible patients with commercial coverage. Medicare Part D does not currently cover Zepbound for weight loss, though the CMS GLP-1 Bridge program launching July 2026 may provide $50/month access for eligible beneficiaries.
What if my doctor wants me off compounded semaglutide immediately?
Start the branded Zepbound process now. Don’t wait until your supply runs out to check insurance, find a telehealth provider, or set up LillyDirect. A treatment gap is the single biggest risk factor for appetite return and weight fluctuation during a switch.
Can I switch to Wegovy instead of Zepbound?
Yes. Wegovy (semaglutide) is another FDA-approved option for weight management. If your insurance covers Wegovy but not Zepbound, or if Wegovy’s cash-pay pricing fits your budget better, it’s a reasonable alternative. Head-to-head clinical data favors Zepbound for greater average weight loss, but individual responses vary.
Is compounded semaglutide still available in 2026?
In very limited circumstances. After the FDA declared the semaglutide shortage resolved and enforcement grace periods expired in mid-2025, routine compounding of semaglutide copies is no longer permitted. Narrow 503A exceptions exist for patients with a documented individual medical need — such as a verified allergy to an inactive ingredient in the branded product — but cost or convenience alone does not qualify.
Can I use my HSA or FSA to pay for Zepbound?
Yes. Zepbound is an FDA-approved prescription medication and is eligible for payment through health savings accounts and flexible spending accounts.
Still Not Sure Which GLP-1 Program Is Right for You?
A few quick questions about your insurance, budget, medical history, and goals. We match you with the right medication and the best way to pay for it. No spam. No obligations.
Take the Free GLP-1 Matching Quiz →Related guides
Sources
- Zepbound (tirzepatide) prescribing information. FDA Access Data. Eli Lilly and Company.
- Zepbound Savings Card terms and conditions. zepbound.lilly.com/savings. Verified April 2026.
- LillyDirect self-pay pricing. zepbound.lilly.com/coverage-savings. Verified April 2026.
- FDA. “FDA clarifies policies for compounders as national GLP-1 supply begins to stabilize.” FDA.gov, 2025.
- Surmount-5 trial results. New England Journal of Medicine. 2025.
- Rodriguez PJ, et al. JAMA Internal Medicine. 2024.
- Almandoz JP, et al. Clinical Diabetes. 2020.
- CMS. Medicare GLP-1 Bridge program. cms.gov.
The RX Index is an independent research platform. We may earn a commission from providers linked on this page. Our editorial recommendations are based on independent research, verified pricing, and clinical accuracy — not compensation. Full affiliate disclosure →
This content is for informational and educational purposes only and is not medical advice. All medication decisions should be made by a licensed clinician based on your individual health profile.