How to Switch From Semaglutide to Mounjaro
Timing, starting dose, side effects, cost — and the brand question most guides skip: whether you actually need Mounjaro or Zepbound.
Written by The RX Index Editorial Team · Last verified: April 7, 2026
Bottom line
The common clinician-guided approach: take your last semaglutide dose, avoid any overlap, and start Mounjaro 2.5 mg once weekly on your next injection day — usually about 7 days later. There is no official milligram-for-milligram conversion chart between the two drugs. But here's the part most guides bury: if you're switching for weight loss and you don't have type 2 diabetes, you may need Zepbound, not Mounjaro. Both are tirzepatide — the brand on the prescription changes everything about your coverage and cost.
| Your situation | The real question | Likely next step |
|---|---|---|
| Ozempic + type 2 diabetes | How do I switch to Mounjaro? | Discuss timing, 2.5 mg start, and formulary coverage with your prescriber |
| Wegovy or compounded semaglutide + weight loss (no diabetes) | Should I be asking for Zepbound instead? | Check the obesity-indication tirzepatide path |
| Active nausea, vomiting, or diarrhea right now | Should I wait before switching? | Talk to your clinician before making any changes |
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice. Mounjaro (tirzepatide) is a prescription medication. Always consult a licensed healthcare provider before starting, stopping, or switching any medication.
Talk to your clinician before switching if you have active nausea, vomiting, diarrhea, or dehydration.
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
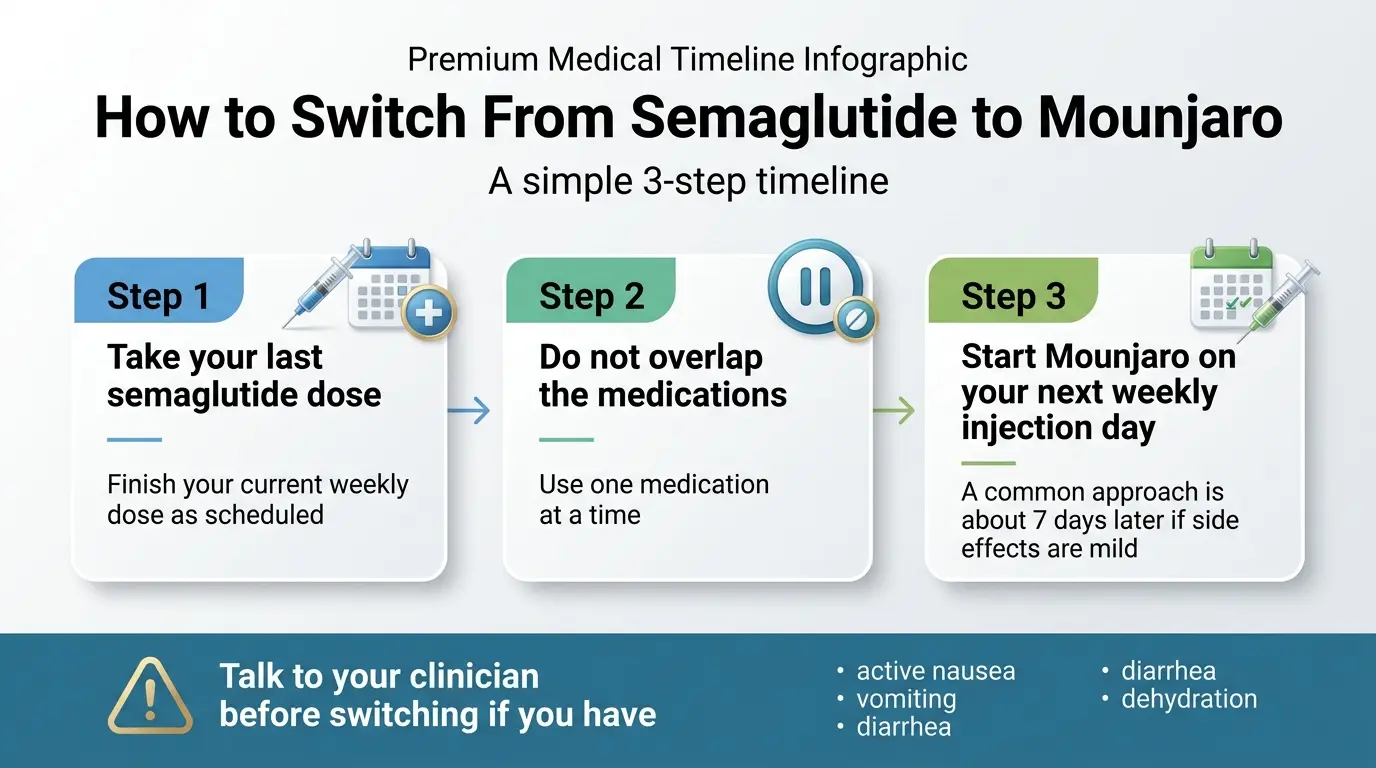
How to Switch From Semaglutide to Mounjaro in 3 Steps
The switch follows three steps: finish semaglutide, wait for your next injection day, and start Mounjaro at 2.5 mg. There is no validated conversion chart, and you should not take both medications at the same time.
Take your last semaglutide dose as scheduled.
Don't skip a dose or try to clear it faster. Just take your final dose as planned and note the date.
Wait until your next weekly injection day
Usually about 7 days — if your side effects are mild or resolved. If you still have active nausea, vomiting, or diarrhea, talk to your clinician about waiting longer.
Start Mounjaro at 2.5 mg once weekly
Unless your clinician gives you a different starting dose. Titrate up every 4 weeks as directed. The rest of this guide covers each step in depth — dosing nuances, what to expect week by week, cost across every access path, and the brand question that changes everything.
Do You Actually Need Mounjaro — or Zepbound?
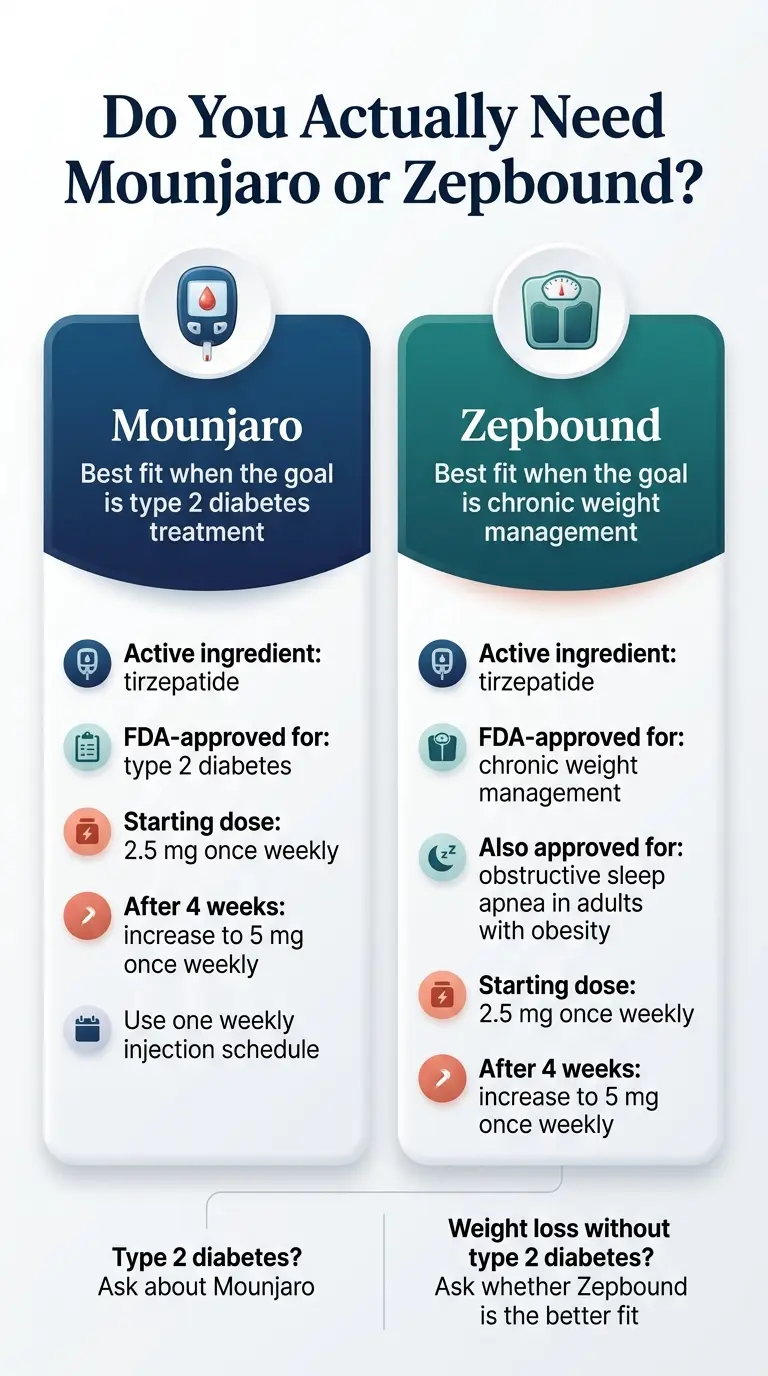
Same active ingredient (tirzepatide), different FDA-approved indications.
Mounjaro and Zepbound are both tirzepatide made by Eli Lilly, but they carry different FDA-approved indications. Mounjaro is approved to improve blood sugar control in adults with type 2 diabetes. Zepbound is approved for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related condition, and for obstructive sleep apnea in adults with obesity. Picking the wrong brand doesn't change the drug — it changes your insurance coverage and out-of-pocket cost.
This is the question no one else is answering clearly enough. Most guides treat "switching to Mounjaro" and "switching to tirzepatide" as interchangeable. They're not.
| Factor | Mounjaro | Zepbound |
|---|---|---|
| Active ingredient | Tirzepatide | Tirzepatide |
| FDA-approved for | Type 2 diabetes (with diet and exercise) | Chronic weight management; OSA in adults with obesity |
| Dose range | 2.5 mg – 15 mg weekly | 2.5 mg – 15 mg weekly |
| Manufacturer | Eli Lilly | Eli Lilly |
| Insurance coverage | Many commercial plans cover for T2D | Limited for weight loss; stricter formulary rules |
| Savings card (with coverage) | As low as $25/mo | As low as $25/mo |
| Self-pay without coverage | ~$1,000–$1,200/mo retail | Starts at $299/mo through LillyDirect vials |
| Medicare Part D | May cover for T2D | Generally not covered for obesity (2026 expansion expected) |
Sources: Mounjaro prescribing information; Zepbound prescribing information; LillyDirect.
If you have type 2 diabetes → Mounjaro
Mounjaro is the cleaner insurance path. It's the brand your endocrinologist or PCP will write on the prescription, and it's what commercial formularies are most likely to cover with prior authorization. The Mounjaro Savings Card can bring your copay down to $25 per month if your commercial plan covers it.
If your goal is weight loss without type 2 diabetes → Zepbound
If your doctor writes a Mounjaro prescription for weight loss in a patient without diabetes, most insurers will deny it. Mounjaro isn't FDA-approved for that use. Zepbound is the same drug with the weight-management label — which gives you a legitimate insurance claim and access to LillyDirect self-pay vials if insurance won't cooperate.
Before your prescriber writes the script — two questions to ask your insurer
- "Is Mounjaro (tirzepatide) on formulary for type 2 diabetes?"
- "Is Zepbound (tirzepatide) on formulary for chronic weight management?"
The answers will determine your cheapest path before any prescriptions are written.
Still not sure which tirzepatide brand to ask about?
Get matched in 60 seconds based on your diagnosis, insurance, and goals.
Can You Switch From Semaglutide to Mounjaro?
Yes, with clinician guidance. A common clinician-guided approach is to finish your current semaglutide, avoid any overlap between the two medications, and begin Mounjaro on your next weekly injection day — typically about 7 days after your last semaglutide dose — if side effects are mild or resolved.
There's nothing exotic about this switch. Semaglutide (Ozempic, Wegovy) is a GLP-1 receptor agonist. Tirzepatide (Mounjaro, Zepbound) is a dual GIP and GLP-1 receptor agonist — it activates a second hormone pathway (GIP) on top of GLP-1. That dual mechanism is why you start at the bottom of the tirzepatide dose ladder even if you were on maximum-dose semaglutide.
Who should pause and talk to a clinician first
- You currently have active nausea, vomiting, or diarrhea from semaglutide
- You have a personal or family history of medullary thyroid carcinoma (MTC) or MEN 2 syndrome
- You're pregnant, breastfeeding, or planning to become pregnant
- You have a history of pancreatitis
- You have surgery or anesthesia scheduled in the coming weeks
Ozempic to Mounjaro
The most common brand-to-brand switch in the type 2 diabetes space. You're moving from one diabetes-indicated medication to another. Your endocrinologist or PCP handles the transition, and insurance coverage is typically the smoothest here since both drugs are approved for T2D.
Wegovy to Mounjaro
Less common and more nuanced. Wegovy is the semaglutide brand approved for weight management. If you're switching to Mounjaro specifically (not Zepbound), your prescriber needs a diabetes indication to justify Mounjaro. If weight loss is the primary goal, Zepbound is almost always the better destination. If you're on Wegovy and your prescriber suggests Mounjaro, ask: "Is this because I also have type 2 diabetes, or should we be looking at Zepbound?"
Compounded Semaglutide to Mounjaro
If your compounded semaglutide supply is ending — whether due to the FDA resolving the semaglutide shortage in February 2025 or your pharmacy discontinuing it — the brand question matters even more. Most compounded semaglutide users were using it for weight loss, not diabetes. That means Zepbound is usually the right landing spot, not Mounjaro.
See our dedicated guide: How to Switch From Compounded Semaglutide to Zepbound →
Insurance concierge + prior auth support included
How Long Should You Wait After Semaglutide Before Starting Mounjaro?
A formal washout period is often not needed when side effects are mild, but the safest timing depends on symptoms, dose, and clinician judgment. The common approach is to start Mounjaro approximately 7 days after your last semaglutide injection — on your next weekly injection day.
The 7-Day Approach Most Providers Follow
Semaglutide has a half-life of approximately 7 days. By the time your next weekly injection day rolls around, your semaglutide levels are naturally declining. Many providers recommend starting tirzepatide right on that next injection day to stay on your weekly schedule with no meaningful gap in treatment.
A published prospective study found that patients switching directly from GLP-1 medications to tirzepatide 5 mg tolerated it well — only about 13% experienced GI side effects, and just 2% discontinued due to adverse events. The transition is not the dramatic event many people fear.
When a Longer Wait Makes Sense
If you're still dealing with nausea, vomiting, diarrhea, or dehydration from semaglutide, adding a new injectable medication on top of active symptoms is asking for trouble. In these cases, providers may recommend waiting until symptoms settle — sometimes 2 weeks, occasionally longer. Some UK-based providers recommend a 4–5 week washout; if your provider recommends a longer wait, ask them to explain why.
Will You Gain Weight During the Gap?
With a 7-day transition, weight regain is minimal — semaglutide is still partially active. With a longer gap (3–5 weeks), some people report rapid rebound hunger and weight gain. This is one more reason to discuss the shorter transition with your clinician when your side effects allow it.
Why you should never overlap the two medications
Do not take semaglutide and tirzepatide at the same time. Both act on the GLP-1 receptor. Stacking them increases the risk of severe nausea, vomiting, and potentially dangerous dehydration without providing additional benefit. The Mounjaro prescribing information does not recommend coadministration with another GLP-1 receptor agonist.
What Dose of Mounjaro Do You Start After Semaglutide?
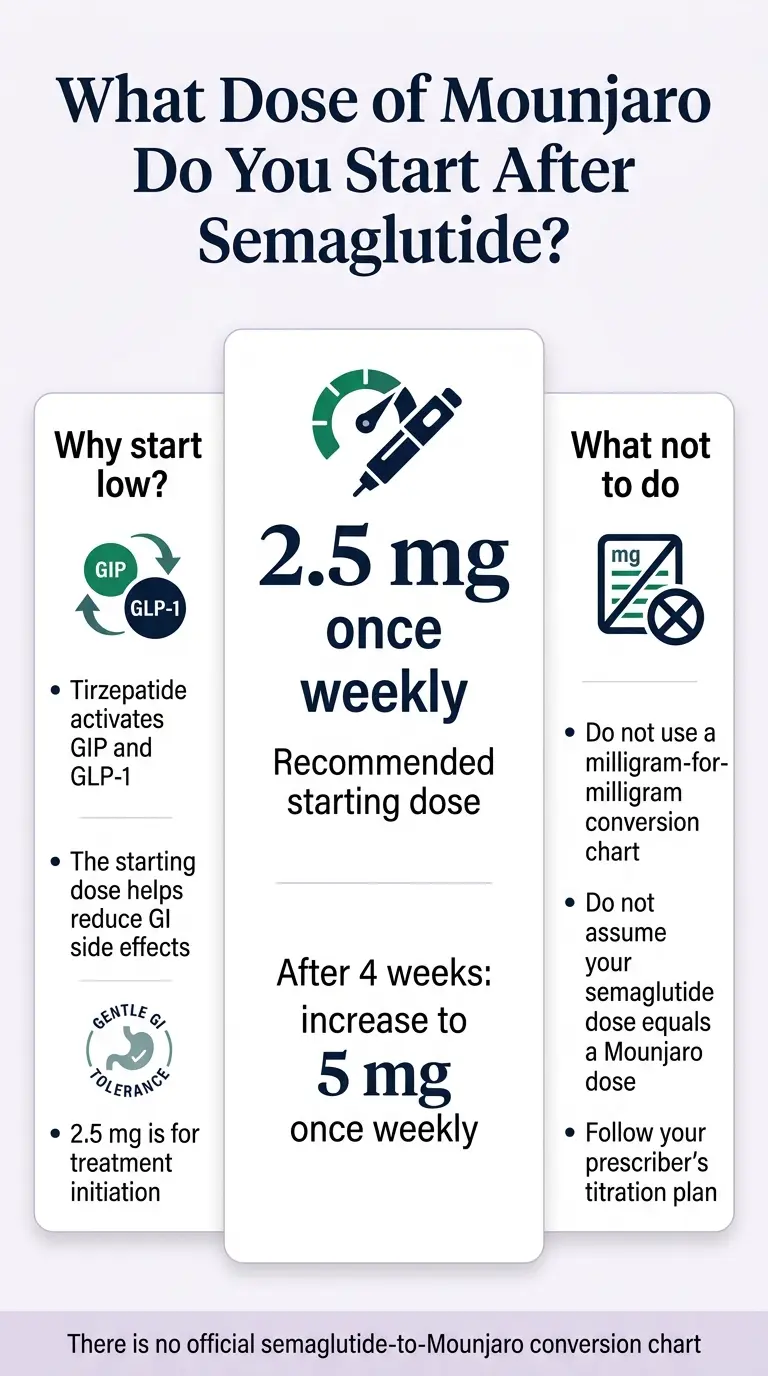
There is no official semaglutide-to-Mounjaro conversion chart. The labeled starting dose is 2.5 mg once weekly.
The labeled Mounjaro starting dose is 2.5 mg once weekly — even if you were on the maximum 2.4 mg dose of semaglutide. There is no official milligram-for-milligram semaglutide-to-Mounjaro conversion. You start low because tirzepatide is a different molecule with a dual receptor mechanism your body hasn't encountered before.
Semaglutide targets one receptor (GLP-1). Tirzepatide targets two (GLP-1 and GIP). Even though your body has adapted to GLP-1 activity from semaglutide, the GIP component is completely new. The 2.5 mg starting dose lets your body adjust to that second pathway without overwhelming your digestive system.
Think of it this way: you're not starting over on the same medication. You're starting a different medication that shares one mechanism with what you've been taking and adds another one on top.
Mounjaro titration schedule (every 4 weeks)
Your prescriber adjusts based on your response, tolerability, and treatment goals. Not everyone needs to reach 15 mg.
| Your semaglutide dose | Typical Mounjaro starting point | Notes |
|---|---|---|
| 0.25–0.5 mg Ozempic (still titrating) | 2.5 mg | Labeled start; you're early in GLP-1 therapy |
| 1.0 mg Ozempic (maintenance) | 2.5 mg | Labeled start; titrate up based on response |
| 2.0 mg Ozempic (max dose) | 2.5 mg (some providers: 5 mg) | Higher start only if GI tolerance was excellent |
| 1.7–2.4 mg Wegovy | 2.5 mg (some providers: 5 mg) | Same logic as high-dose Ozempic |
| Compounded semaglutide (varies) | 2.5 mg | Compounded doses vary widely; default to labeled start |
Is There a Semaglutide to Mounjaro Conversion Chart?
No official conversion chart exists. Semaglutide and tirzepatide are different molecules that work through different receptor pathways, and their dosing ranges aren't directly comparable. Published dose charts are guides for discussion, not validated conversions.
Semaglutide doses range from 0.25 mg to 2.4 mg weekly. Tirzepatide doses range from 2.5 mg to 15 mg weekly. Looking at those numbers, it's tempting to think 2.4 mg of semaglutide "equals" some specific mg of tirzepatide. It doesn't. The milligram amounts reflect each drug's individual potency curve — like comparing kilometers and miles, different scales measuring overlapping but not identical effects.
Some clinics publish tables showing approximate clinical equivalency based on trial outcomes. These can be useful for setting expectations about where you might land once fully titrated. Use these guides to have a conversation with your prescriber. Don't use them to self-prescribe a starting dose.
Skip the guesswork
Get a plan based on your actual situation — diagnosis, insurance, and goals.
What to Expect in the First 4–8 Weeks After Switching
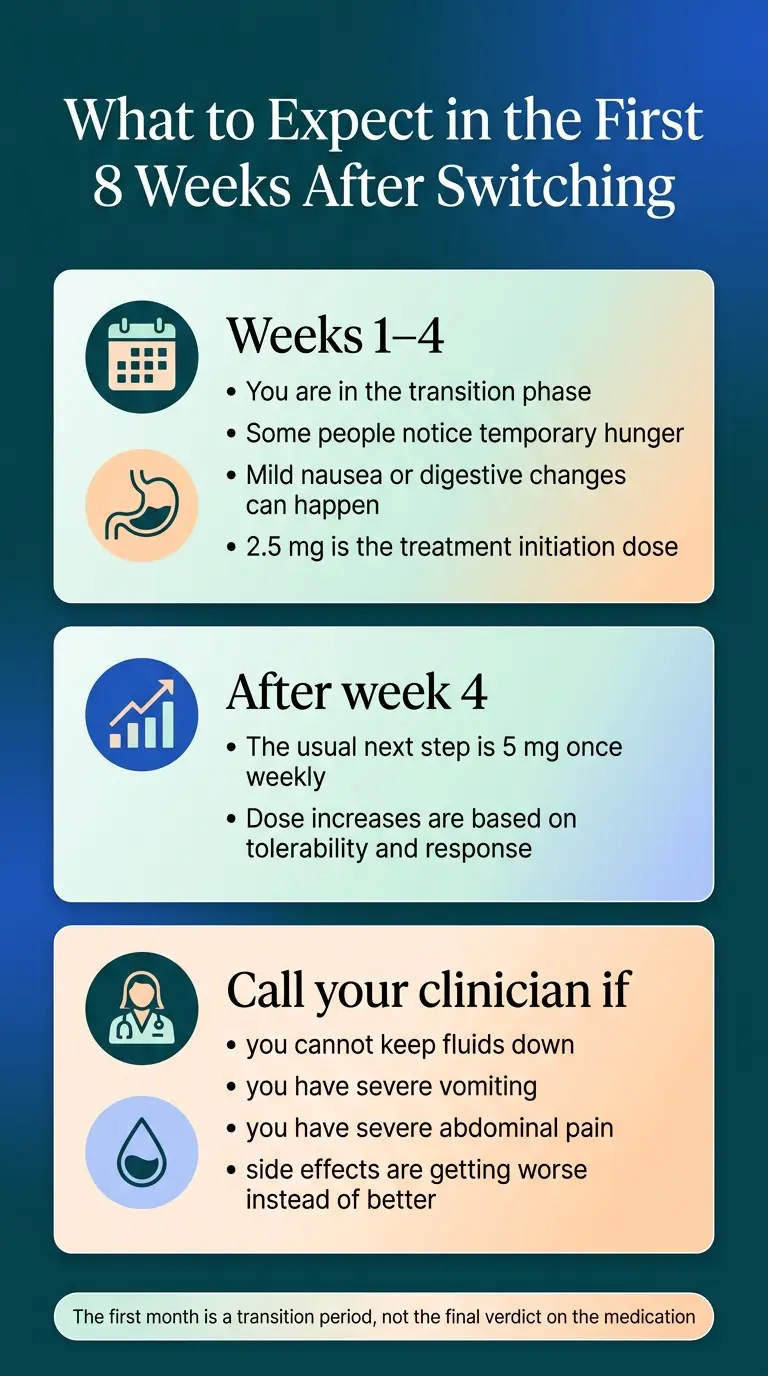
The first month is a transition period, not the final verdict on the medication.
The first month is the part people are most anxious about, and it's the most variable. Some people feel hungrier at the lower starting dose, others report fewer GI side effects than they had on semaglutide, and a few notice stronger appetite suppression almost immediately. The key framing: the first 4 weeks are a transition period, not the final verdict on the medication.
| Time period | What you may notice | What's normal | When to call your prescriber |
|---|---|---|---|
| Week 1–2 | Mild nausea, bloating, or digestive changes. Possibly more hunger than you had on semaglutide. | Your body is adjusting to a new molecule and the GIP receptor activation. | Severe vomiting, inability to keep fluids down, or sharp abdominal pain |
| Week 3–4 | Appetite suppression building. GI symptoms usually improving. Some people feel "different" from semaglutide — the appetite effect has a different quality. | Normal. The dual mechanism is kicking in. | Persistent diarrhea, dehydration signs, or worsening symptoms instead of improving |
| Week 5–8 (after first dose increase to 5 mg) | Brief GI flare possible at the new dose. Appetite suppression strengthening. Weight loss typically resuming or accelerating. | Mild nausea around dose increases is common and usually passes in a few days. | Same as above; also watch for signs of low blood sugar if you're on insulin or sulfonylureas |
Tips that actually help during the transition
- •Eat smaller, more frequent meals. Tirzepatide slows gastric emptying. Large meals sit heavier.
- •Cut back on high-fat and fried foods especially in the first 2 weeks after each dose increase. Fat takes longer to digest, and the combination with slowed gastric emptying can trigger nausea.
- •Stay hydrated. Reduced appetite often means reduced fluid intake without realizing it. Set a water reminder if you need to.
- •Prioritize protein. This matters on any GLP-1 medication, but especially during a switch when appetite may fluctuate.
- •Don't judge the medication at 2.5 mg. The starting dose is for tolerability, not efficacy. Give it time to titrate.
"My insurance finally covers GLP-1s. I'm starting Mounjaro from compounded semaglutide…"— Reddit r/Mounjaro user, February 2025
"Mounjaro is night and day. I have zero hunger, no food noise…"— Reddit r/Mounjaro user, 2024
Note: These are anecdotal individual experiences, not typical results — but they illustrate the range of what people report. The honest takeaway: most people tolerate the switch well. A minority have a rough first couple of weeks. Almost everyone needs to adjust expectations during the low-dose titration period.
Why Do People Switch From Semaglutide to Mounjaro?
The most common reasons are a weight loss plateau, inadequate blood sugar control despite dose optimization, persistent side effects, or an insurance change that now covers tirzepatide.
The plateau problem: You lost 15, 20, 30 pounds on semaglutide. Then progress stopped, sometimes for months, even at the maximum dose. Tirzepatide's additional GIP pathway may help push past that stall by targeting a second hormonal lever. That's the theory, and the clinical data supports it on average — though individual results vary.
| Study | What it compared | Key finding | Context |
|---|---|---|---|
| SURMOUNT-5 (2025) | Tirzepatide vs. semaglutide in adults with obesity | 20.2% mean weight loss with tirzepatide vs. 13.7% with semaglutide at 72 weeks | Randomized, head-to-head trial |
| Real-world cohort (2024, JAMA, n≈18,000) | Tirzepatide vs. semaglutide in clinical practice | Tirzepatide patients 1.76x more likely to lose ≥5% body weight, 3.24x more likely to lose ≥15% | Large dataset, real-world conditions |
| SURPASS-2 (2021, type 2 diabetes) | Tirzepatide vs. semaglutide 1 mg in T2D | Tirzepatide reduced A1C by up to 2.3% vs. 1.86% for semaglutide; greater weight loss at all doses | Note: compared to semaglutide 1 mg only, not 2 mg or 2.4 mg doses |
How Much Does Mounjaro Cost, and Will Insurance Cover It?
Mounjaro's list price is $1,112.16 for a 28-day supply. With commercial insurance coverage plus the Mounjaro Savings Card, eligible patients may pay as little as $25 for up to a 3-month prescription. Without insurance, the self-pay landscape for tirzepatide is better through Zepbound via LillyDirect.
| Access path | Monthly cost | Best for | Key requirements |
|---|---|---|---|
| Mounjaro + commercial insurance + savings card | As low as $25/mo | Type 2 diabetes with commercial coverage | Insurance must cover Mounjaro; savings card enrolled |
| Zepbound + commercial insurance + savings card | As low as $25/mo | Obesity/overweight with commercial coverage | Insurance must cover Zepbound; savings card enrolled |
| Zepbound self-pay vials (LillyDirect) | Starts at $299/mo; varies by dose | No insurance coverage, want brand-name | Prescription required |
| Compounded tirzepatide (telehealth providers) | Varies by provider | Cash-pay patients | Telehealth consult; compounding pharmacy |
| Mounjaro retail (no insurance, no savings) | ~$1,000–$1,200/mo | Last resort | Not recommended — explore alternatives first |
Pricing verified April 7, 2026. Savings card terms and LillyDirect pricing change periodically — verify before filling.
The insurance conversation
For type 2 diabetes: Mounjaro has the strongest insurance footing. Prior authorization is common — your prescriber submits documentation showing a T2D diagnosis and inadequate control on current therapy. Coverage varies by plan.
For weight loss without diabetes: Most commercial plans don't cover Mounjaro for weight loss since it's not FDA-approved for that indication. Zepbound is the FDA-approved weight-loss tirzepatide, but coverage is still limited — many plans treat obesity medications as "lifestyle" exclusions.
For Medicare: Part D may cover Mounjaro for type 2 diabetes. Weight-loss medications have historically been excluded. Check with your Part D plan directly for the most current information.
What the Savings Card actually does
The Mounjaro Savings Card reduces your copay for eligible commercially insured patients — as low as $25 for a 1-, 2-, or 3-month supply. Not eligible: Medicare, Medicaid, TRICARE, VA, or other government insurance. The Zepbound Savings Card works similarly for eligible patients.
A note on compounded tirzepatide
Compounded tirzepatide is not FDA-approved, and the FDA does not verify its safety, effectiveness, or quality before it reaches patients. The FDA resolved the tirzepatide shortage on December 19, 2024. The availability and legal status of compounded tirzepatide may continue to evolve. If you're considering this path, verify that your provider uses a licensed pharmacy and discuss the regulatory status with them.
If you have commercial insurance → for diabetes
Check Mounjaro Coverage Navigation on Ro →If you're a cash-pay patient → tirzepatide options
See Tirzepatide Pricing and Options on MEDVi →What if Mounjaro Doesn't Work — Can You Switch Back?
Yes. Switching back to semaglutide is possible with clinician guidance. The timing and restart dose depend on why you stopped tirzepatide, whether side effects are still active, and what dose you were on.
This isn't a one-way door. Some patients switch to tirzepatide and prefer it. Others discover they had better appetite control or fewer side effects on semaglutide. A few try both and settle on a preference after comparing their actual experience with each drug. Finding the right GLP-1 is sometimes a process, not a single decision.
The main thing to know: you will likely need to retitrate semaglutide from a lower dose if you switch back. Your body's adaptation to semaglutide decreases while you're off it. Your prescriber will determine the appropriate restart dose.
When You Should NOT Switch Yet
Do not force the switch based on internet hype alone. If any of the following apply, wait.
Active nausea, vomiting, or dehydration
If you're still experiencing significant side effects from semaglutide, adding a new GLP-1/GIP agonist will likely make things worse. Wait until symptoms resolve, then discuss timing with your prescriber.
Medullary Thyroid Carcinoma (MTC) or MEN 2 Syndrome
Tirzepatide carries a boxed warning: it is contraindicated in patients with a personal or family history of MTC or MEN 2. If this applies to you, tirzepatide is not an option regardless of brand.
Pregnancy, breastfeeding, or planning to conceive
Tirzepatide should be stopped at least 2 months before a planned pregnancy due to its long washout period. If you're currently pregnant or breastfeeding, this medication is not appropriate.
Oral contraceptive users — a detail most guides miss
The Mounjaro prescribing information notes that tirzepatide may reduce the effectiveness of oral hormonal contraceptives by slowing gastric emptying. Discuss switching to a non-oral backup method or adding a barrier method for 4 weeks after starting Mounjaro and 4 weeks after each dose increase. This is not a minor detail — it's in the label.
Upcoming surgery or anesthesia
GLP-1 medications slow gastric emptying, which matters for anesthesia safety. Tell your anesthesiologist that you take semaglutide or tirzepatide. Current multisociety guidance says most patients can continue GLP-1 medications before surgery, but the plan should be individualized. Discuss timing with both your prescriber and anesthesiologist before starting tirzepatide if surgery is upcoming.
How We Verified This Guide
Every factual claim on this page is traceable to official prescribing information, published clinical data, or verified manufacturer pages. We don't cite secondhand summaries when the primary source is available.
| Source | Used for |
|---|---|
| Mounjaro prescribing information (pi.lilly.com) | Dosing, titration schedule, contraindications, oral contraceptive warning |
| Zepbound prescribing information (pi.lilly.com) | FDA indication, coadministration guidance |
| Mounjaro FAQ and pricing page (mounjaro.lilly.com/faq) | List price $1,112.16, Savings Card terms, $25/mo minimum |
| LillyDirect (lillydirect.com) | Zepbound self-pay pricing from $299/mo |
| SURMOUNT-5 trial (Eli Lilly press release, 2025) | 20.2% vs. 13.7% weight loss head-to-head data |
| JAMA real-world cohort study (2024, n≈18,000) | 1.76x more likely ≥5% weight loss with tirzepatide |
| SURPASS-2 (NEJM, 2021) | Tirzepatide vs. semaglutide 1 mg A1C and weight loss comparison |
| FDA drug shortage resolution notices (fda.gov) | Tirzepatide shortage resolved Dec 19, 2024; semaglutide Feb 21, 2025 |
| ASA multisociety perioperative GLP-1 guidance | Surgery/anesthesia recommendations |
What would trigger an update: Any revision to the Mounjaro or Zepbound prescribing information, any change in list pricing or savings card terms, any new head-to-head trial data, or any significant shift in insurance coverage policy. Last verified: April 7, 2026.
FAQ: Switching From Semaglutide to Mounjaro
Can you switch from semaglutide to Mounjaro without a break?
Most people switch by taking their last semaglutide dose, not overlapping the medications, and starting Mounjaro on the next weekly injection day — typically about 7 days later. A formal washout period is often not needed when side effects are mild, though providers may recommend a longer wait if symptoms are still active.
How long after semaglutide can I start Mounjaro?
The common clinician-guided approach is approximately 7 days — on your next scheduled injection day. Semaglutide's half-life is about 7 days, so levels are naturally declining by then. Longer waits may be appropriate if you're still experiencing significant side effects.
What dose of Mounjaro do you start after semaglutide?
The labeled starting dose is 2.5 mg once weekly, regardless of your prior semaglutide dose. There is no official milligram-for-milligram conversion between semaglutide and tirzepatide. Some clinicians may start at 5 mg for patients who tolerated higher semaglutide doses without GI issues.
What dose of Mounjaro do you start after Ozempic 1 mg?
The labeled starting dose is 2.5 mg weekly, regardless of your prior semaglutide dose. Some clinicians may start at 5 mg for patients who tolerated higher semaglutide doses without GI issues, but 2.5 mg is the labeled initiation dose per the prescribing information.
What dose of Mounjaro do you start after Wegovy 2.4 mg?
Still 2.5 mg in most cases. Even at the highest semaglutide dose, your body hasn't encountered tirzepatide's GIP receptor activity before. Starting at 2.5 mg allows for adjustment. Some providers may begin at 5 mg based on individual tolerance.
Is there a semaglutide to Mounjaro conversion chart?
No official milligram-for-milligram conversion chart exists. Semaglutide and tirzepatide are different molecules with different mechanisms and dose ranges. Published tables are discussion guides, not validated conversions.
Can you take semaglutide and Mounjaro at the same time?
No. Coadministration of tirzepatide with another GLP-1 receptor agonist is not recommended. Taking both simultaneously increases side effect risk without adding benefit.
Should I ask for Mounjaro or Zepbound?
Mounjaro is FDA-approved for type 2 diabetes. Zepbound is FDA-approved for chronic weight management in adults with obesity. Both contain tirzepatide. Your diagnosis determines which brand is the better insurance and cost path.
Is Mounjaro for weight loss or diabetes?
Mounjaro is FDA-approved for type 2 diabetes. Zepbound — the same active ingredient (tirzepatide) made by the same manufacturer — is FDA-approved for chronic weight management. If your primary goal is weight loss and you don't have type 2 diabetes, Zepbound is typically the more appropriate brand to discuss with your prescriber.
Will I feel hungrier when I switch to Mounjaro?
Possibly, during the first 2–4 weeks. If you were on a higher semaglutide dose and drop to 2.5 mg tirzepatide, the appetite suppression effect may temporarily decrease. This improves as your tirzepatide dose titrates upward.
Is Mounjaro stronger than semaglutide?
In the SURMOUNT-5 head-to-head trial, tirzepatide produced 20.2% average body weight loss vs. 13.7% for semaglutide over 72 weeks. Individual response varies and some patients respond better to semaglutide.
How much does Mounjaro cost without insurance?
The manufacturer list price is $1,112.16 for a 28-day supply. With the Mounjaro Savings Card and commercial insurance coverage, eligible patients may pay as low as $25 for up to a 3-month supply. Without coverage, Zepbound self-pay vials through LillyDirect (starting at $299/month) are a more affordable brand-name alternative.
What if I'm switching from compounded semaglutide to Mounjaro?
The switching approach is the same: last dose, wait about 7 days, start tirzepatide at 2.5 mg. Most compounded semaglutide users were using it for weight loss, which means Zepbound is often the better brand destination than Mounjaro.
Your Next Step
You've read the protocol. You know the timing, the doses, the costs, and — critically — which tirzepatide brand actually fits your situation. Now it's about doing something with that clarity.
If you have type 2 diabetes and commercial insurance
Talk to your prescriber about Mounjaro, confirm formulary coverage, and enroll in the Mounjaro Savings Card before your first fill.
Check Mounjaro Coverage Navigation on Ro →If you want tirzepatide for weight loss without diabetes
The brand you need is Zepbound, not Mounjaro. Explore LillyDirect self-pay vials or alternatives through a telehealth provider.
See Current Tirzepatide Options on MEDVi →Still not sure which path fits?
Free 60-Second GLP-1 Matching Quiz
It asks about your diagnosis, insurance, current medication, and goals — and gives you a specific next step, not a generic recommendation.
Take the Free GLP-1 Matching Quiz →6 questions · 60 seconds · Free · No signup
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
Related Guides
The RX Index is an independent editorial publisher covering GLP-1 medications and telehealth providers. We may earn a commission when you start treatment through our provider links. Our editorial recommendations are based on independent research, verified pricing, and clinical accuracy — not compensation.
This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider before starting, stopping, or switching any medication.
Last verified: April 7, 2026 · Sources: Mounjaro PI, Zepbound PI, SURMOUNT-5 (2025), JAMA cohort study (2024), SURPASS-2 (NEJM 2021), FDA drug shortage notices, ASA perioperative guidance, Eli Lilly pricing pages.
Related guides