How to Switch from Semaglutide to Tirzepatide: Your Complete 2026 Guide
By The RX Index Editorial Team · Last verified: April 1, 2026 · Sources: FDA prescribing information, 12+ peer-reviewed studies, verified provider pricing
The RX Index may earn a commission when you start a paid program through links on this page. This never influences our editorial recommendations. Prices and policies were checked April 1, 2026.
The Short Answer
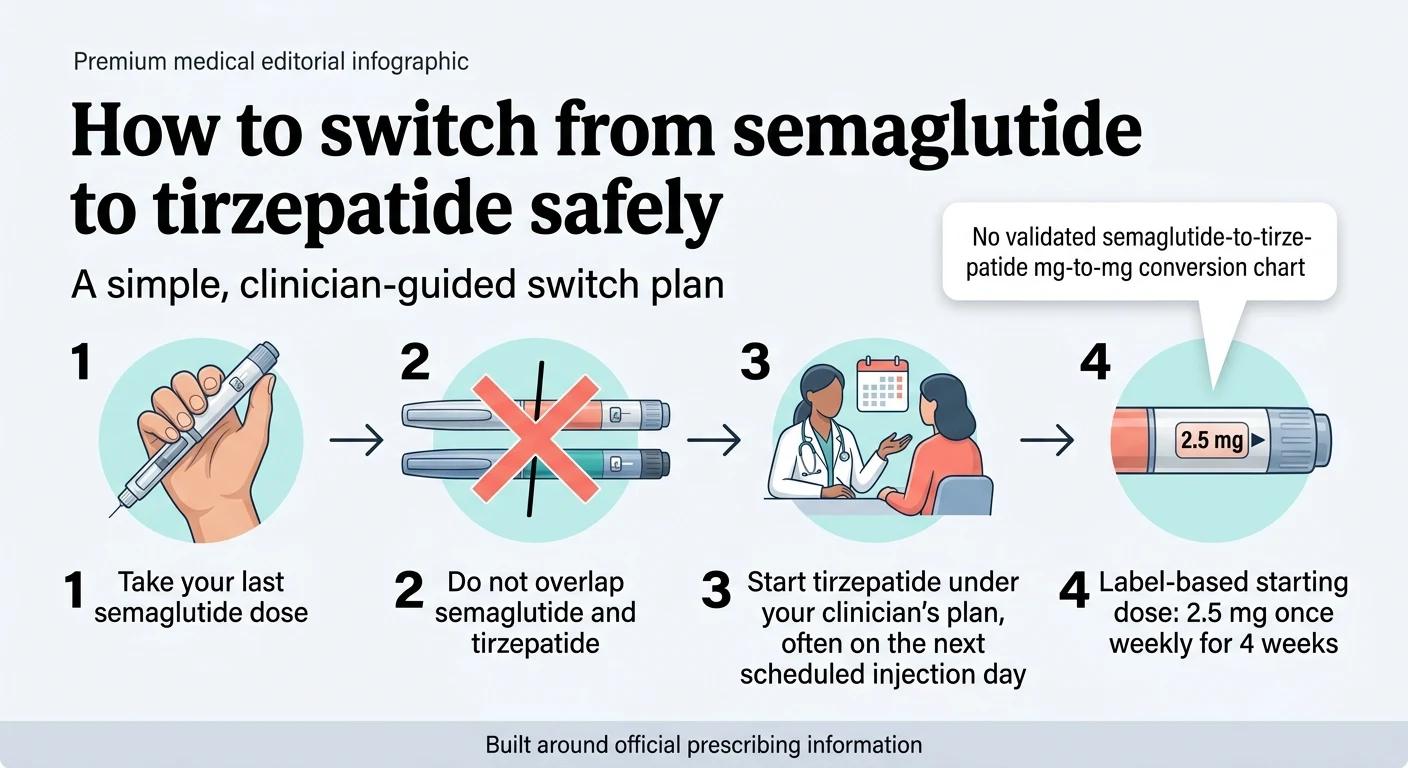
You can switch from semaglutide to tirzepatide without a lengthy washout. The standard approach: take your last semaglutide dose, avoid overlapping the two drugs, and start tirzepatide about 3–10 days later — most commonly on your next scheduled injection day. The FDA-label starting dose is 2.5 mg once weekly for 4 weeks, regardless of your previous semaglutide dose. There is no validated semaglutide-to-tirzepatide dose-equivalence chart.
Why are so many people making this switch? In the SURMOUNT-5 obesity trial, tirzepatide produced 20.2% average body weight loss vs. 13.7% for semaglutide at 72 weeks. Here's everything you need to know to do it safely.
What you'll find on this page: Whether you should switch, the exact 5-step protocol, what dose to start on (and why there's no real “conversion chart”), what the first month actually feels like, side effects, how much it costs, and where to get tirzepatide prescribed — all with cited sources and verified pricing.
Should You Switch from Semaglutide to Tirzepatide?
Probably yes if you've stalled, can't tolerate the side effects, or want stronger results. Definitely not if semaglutide is still working well for you.
Not everyone needs to switch. If you're losing weight consistently on Ozempic or Wegovy and the side effects are manageable, there is zero reason to change medications just because tirzepatide gets more attention online.
But if something has changed — you've hit a wall, the nausea never let up, your compounded semaglutide supply got disrupted, or your doctor mentioned Mounjaro or Zepbound — then switching is a clinically supported decision backed by strong comparative data.
Signs It's Time to Switch
You've plateaued for 8+ weeks. You're doing everything right — consistent doses, clean diet, regular movement — and the scale hasn't budged in two months. A plateau this long on your maximum tolerated semaglutide dose is a legitimate signal that your body may respond better to tirzepatide's dual mechanism.
Persistent side effects aren't improving. If nausea, vomiting, or constipation haven't settled after several months on semaglutide, tirzepatide's different receptor profile sometimes produces a better experience. Many patients report tirzepatide feels different — and often better — at equivalent efficacy levels.
You want more aggressive weight loss. Head-to-head trials consistently show tirzepatide produces greater average weight loss than semaglutide. For a 220-pound person, the difference in trial averages works out to roughly 14 additional pounds.
Your compounded semaglutide supply ended. FDA enforcement on compounding pharmacies has pushed many patients to change medications. Tirzepatide — whether through a telehealth provider or your insurance — is a strong alternative, and the switching protocol is straightforward.
Your insurance or coverage changed. Some plans now cover Zepbound more favorably than Wegovy. If your formulary shifted, the switch may save you money while getting you a more effective medication.
When You Should NOT Switch
If any of these apply, switching isn't the move right now:
- ✗Semaglutide is working well — steady progress, tolerable side effects, good lab numbers. Stay.
- ✗You've been on semaglutide less than 3–4 months. You likely haven't reached a therapeutic maintenance dose yet.
- ✗You have unresolved severe GI symptoms — persistent vomiting, dehydration, or suspected pancreatitis. These need clinical assessment first.
- ✗Personal or family history of medullary thyroid carcinoma (MTC) or MEN2. This is a conversation for your specialist.
- ✗Pregnancy or trying to conceive — timelines differ between the two drugs. Talk to your OB.
- ✗On oral hormonal contraceptives — tirzepatide can reduce their efficacy for 4 weeks after initiation and 4 weeks after each dose increase.
Semaglutide vs. Tirzepatide: Head-to-Head Data
This isn't opinion — it's trial data.
| Semaglutide (Wegovy) | Tirzepatide (Zepbound) | |
|---|---|---|
| Mechanism | GLP-1 receptor agonist | Dual GLP-1 + GIP receptor agonist |
| Avg. weight loss (obesity trials) | ~13.7% body weight, 72 wks (SURMOUNT-5) | ~20.2% body weight, 72 wks (SURMOUNT-5) |
| A1C reduction (diabetes trials) | ~1.5–1.8% | ~2.0–2.4% |
| Dosing range | 0.25 mg → 2.4 mg weekly | 2.5 mg → 15 mg weekly |
| Injection frequency | Once weekly | Once weekly |
| FDA-approved brands | Ozempic, Wegovy, Rybelsus | Mounjaro, Zepbound |
| Common side effects | Nausea, diarrhea, constipation | Nausea, diarrhea, constipation |
| Oral option? | Yes (Rybelsus, Wegovy pill) | Not yet |
| Manufacturer | Novo Nordisk | Eli Lilly |
Sources: SURMOUNT-5 (NEJM 2024), SURPASS-2 (NEJM 2021), STEP-1 trial, FDA prescribing information. Individual results vary.
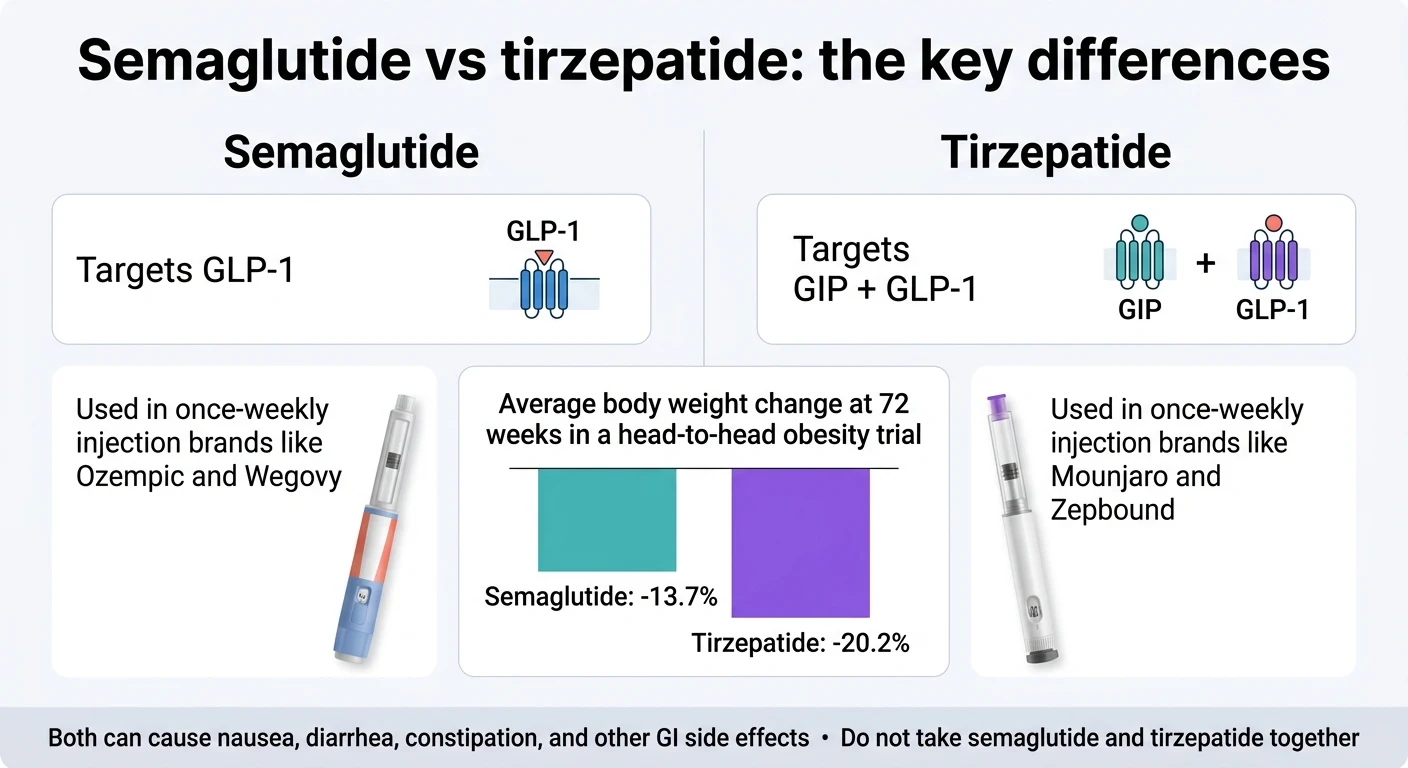
A real-world JAMA study of matched patients found that tirzepatide users were roughly twice as likely to achieve 10%+ weight loss compared to semaglutide users. SURMOUNT-5 confirmed tirzepatide's advantage: 20.2% vs. 13.7% body weight reduction at 72 weeks.
That said, some people genuinely do better on semaglutide. Tirzepatide's edge is statistical, not guaranteed. The “better” medication is whichever one your body responds to.
How to Switch from Semaglutide to Tirzepatide: 5 Steps
The switch is simpler than most people expect. No tapering required, no lengthy washout. For most patients, it's a short gap and a new pen.
Step 1: Talk to Your Provider — or Get a New One
If your current prescriber offers tirzepatide, start there. They already know your history, your dose, and how you've tolerated semaglutide. If they don't — or if you're on a compounded program that's ending — telehealth platforms can prescribe it after a medical evaluation. One thing people miss: if you have any planned surgeries requiring anesthesia, mention that before switching. Both medications slow gastric emptying, which affects anesthesia risk.
Step 2: Take Your Last Semaglutide Dose
Complete your current semaglutide injection on your regular schedule. No need to taper down to a lower dose first. Semaglutide has a half-life of about 7 days, so it starts clearing naturally.
Step 3: Wait — Then Start Tirzepatide
Most providers recommend starting tirzepatide about 3–10 days after your last semaglutide dose — commonly on your next scheduled injection day. The critical safety rule: do not take semaglutide and tirzepatide at the same time. The Zepbound label specifically states that coadministration with another GLP-1 receptor agonist is not recommended.
Step 4: Start Tirzepatide at 2.5 mg
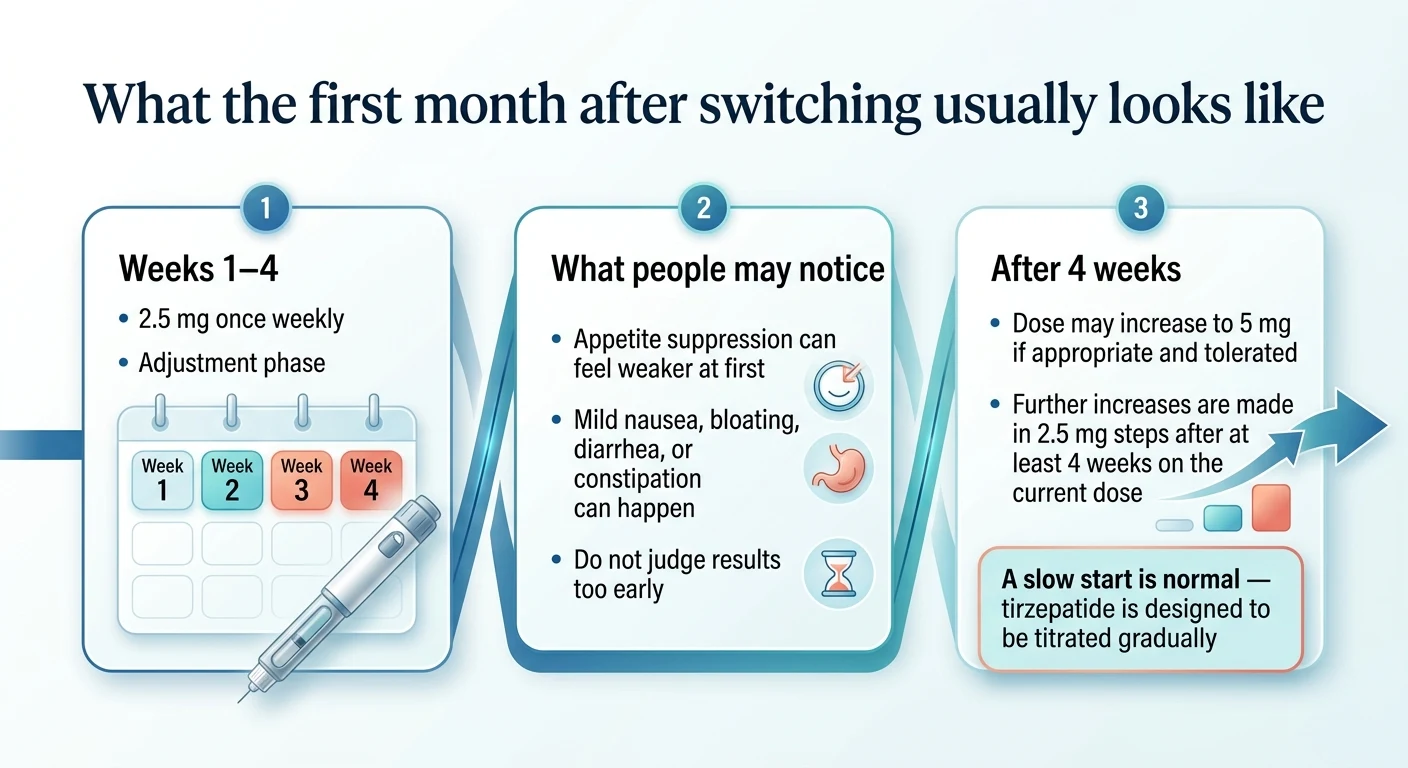
The label-based starting dose is 2.5 mg once weekly for 4 weeks — even if you were on 2.4 mg Wegovy (the maximum semaglutide dose). Tirzepatide is a different drug with a different receptor combination. Your body needs to adjust to the GIP component it's never encountered before. Some providers may start at 5 mg if you tolerated high-dose semaglutide well — but that's a clinical conversation, not the default.
Step 5: Follow the Titration Schedule
Tirzepatide dose increases every 4 weeks based on how you're responding. Not all patients need 15 mg — clinical trials show meaningful results at 10 mg and 12.5 mg. Your provider adjusts based on your weight loss trajectory, side effects, and goals.
Tirzepatide Titration Schedule
| Timeframe | Dose | What Most People Experience |
|---|---|---|
| Weeks 1–4 | 2.5 mg | Adjustment period. Mild nausea possible. You may feel hungrier than on semaglutide — this is temporary. |
| Weeks 5–8 | 5 mg | Appetite suppression picks up. Most initial GI effects settle down. |
| Weeks 9–12 | 7.5 mg | Weight loss typically resumes or accelerates. "Food noise" often quieter than on semaglutide. |
| Weeks 13–16 | 10 mg | Strong appetite suppression. Many patients find their maintenance dose here. |
| Weeks 17–20 | 12.5 mg | Enhanced efficacy. Some providers hold here if progress is strong. |
| Weeks 21+ | 15 mg (max) | Maximum dose. Not everyone needs to reach this level. |
Is There a Semaglutide to Tirzepatide Dose Conversion?
No validated chart exists
Any site giving you a clean “1 mg semaglutide = X mg tirzepatide” conversion is making it up. Semaglutide and tirzepatide have different mechanisms, different titration schedules, and different potency profiles. Clinical experts who've published switching guidance — including the BILH GLP-1RA Conversion Guide and Whitley et al. in Clinical Diabetes — are clear that these drugs are not milligram equivalents.
The practical question is not “What's the equivalent dose?” but “What is the safest starting dose for my switch?” For most people, that answer is 2.5 mg once weekly for 4 weeks, then titration based on tolerability and response.
Approximate clinical equivalencies based on A1C effect in diabetes trials exist in the published literature. They're useful for understanding where you'll likely end up after months of titration — not where you start:
| Your Semaglutide Dose | Approx. Maintenance Range (Tirzepatide) | Your Starting Dose |
|---|---|---|
| 0.25 mg (starter) | 2.5 mg | 2.5 mg |
| 0.5 mg | 2.5–5 mg | 2.5 mg |
| 1.0 mg | 5–7.5 mg | 2.5 mg |
| 1.7 mg (Wegovy) | 7.5–10 mg | 2.5 mg |
| 2.0 mg (Ozempic max) | 10–12.5 mg | 2.5 mg |
| 2.4 mg (Wegovy max) | 10–15 mg | 2.5 mg |
Adapted from Whitley HP et al., Clinical Diabetes 2023; BILH GLP-1RA Conversion Guide. Approximate ranges based on glycemic effect in T2D populations — not FDA-verified conversions and not a substitute for clinical judgment.
See the pattern? The right column is 2.5 mg across the board. Think of it as getting on an escalator at the ground floor — you'll ride it up over months to the dose that works for your body.
Why the First Weeks Can Feel Like a Step Backward
If you were on 2.4 mg Wegovy, you're going from a high-potency medication down to an initiation dose. That means the first 4–8 weeks may feel like a regression — weaker appetite suppression, more food noise, maybe even some weight fluctuation. The key thing to internalize now: this is not tirzepatide failing. It's tirzepatide starting. By week 12, most patients report equal or stronger appetite control than they had on semaglutide.
What the First Month Actually Feels Like
Expect an adjustment period, not instant results. The first month on tirzepatide after semaglutide is a re-entry phase — your body is adapting to a new drug at a low dose.
Week 1 (Tirzepatide 2.5 mg)
You might feel… almost nothing. At 2.5 mg, many patients report minimal appetite suppression — especially coming from a higher semaglutide dose. Some experience mild nausea or bloating. Others feel hungrier than they have in months. This is normal. The dose is intentionally low.
Weeks 2–4
Your body is adjusting to tirzepatide's dual mechanism (GLP-1 + GIP). Most initial GI effects begin to settle. Appetite suppression is still modest. Weight may hold steady or fluctuate slightly. The most common complaint: “I'm more hungry and have way more food noise.” Keep your protein intake high (30g+ per meal), eat smaller portions, and stay hydrated. This phase passes.
Weeks 5–8 (First Dose Increase to 5 mg)
This is where most patients start feeling the medication kick in. Appetite suppression noticeably increases. Many patients describe this as the moment tirzepatide starts to feel “different” from semaglutide: stronger satiety, less food noise, and a feeling of fullness that's less about nausea and more about genuine disinterest in eating.
Weeks 9–16 (Titrating Through 7.5 mg → 10 mg)
Weight loss typically accelerates here. Side effects are usually minimal by this point. Energy levels often improve as your body adapts and the weight comes off. This is where the clinical trial data starts showing tirzepatide pulling ahead of semaglutide's trajectory.
Month 4–6 and Beyond
Full therapeutic effect. Most patients who switched due to a plateau report that their weight loss has not only resumed but exceeded their semaglutide pace. Average body weight reduction of 15–22% is achievable at maintenance dose over 9–12 months of consistent use.
Side Effects When Switching from Semaglutide to Tirzepatide
If you tolerated semaglutide, there's a good chance you'll tolerate tirzepatide — especially with the slow dose escalation.
Both medications cause similar GI side effects. A large real-world study of over 18,000 patients found that rates of GI side effects were similar between tirzepatide and semaglutide users, with no statistically significant difference. In the prospective switch study, only about 13% of patients switching directly to tirzepatide 5 mg reported GI events, and just 2% stopped the medication because of them.
| Side Effect | On Semaglutide | On Tirzepatide | Notes |
|---|---|---|---|
| Nausea | Common | Common (25–29% in Zepbound trials) | Usually dose-dependent, settles over time |
| Diarrhea | Common | Common | Mild and temporary for most |
| Constipation | Common | Common | Increase fiber and water |
| Vomiting | Less common | Less common | Report persistent vomiting to your provider |
| Temporary appetite return | N/A | Possible during transition | Due to starting at a lower dose |
| Injection site reactions | Rare | Rare | Rotate injection sites |
Source: Zepbound prescribing information (Eli Lilly), SURPASS-2 safety data.
When to Call Your Provider
Contact your clinician right away if you experience:
- !Severe or persistent abdominal pain (possible pancreatitis sign)
- !Vomiting that won't stop or signs of dehydration
- !Vision changes
- !Signs of allergic reaction (rash, swelling, difficulty breathing)
How to Minimize Side Effects During the Switch
- →Eat smaller, more frequent meals. Five to six small meals beats three large ones during dose increases.
- →Prioritize protein. 30g+ per meal helps preserve muscle and manage hunger during the low-dose phase.
- →Stay hydrated. 64+ ounces of water daily. GLP-1 medications slow gastric emptying, and dehydration makes every GI side effect worse.
- →Avoid heavy, fatty, or fried foods during the first week of each dose increase.
- →Don't skip doses. Consistency helps your body adapt faster.
Does Tirzepatide Actually Work Better Than Semaglutide?
On average, yes — and the data is strong enough that this isn't a marketing claim. But “better on average” doesn't mean “better for everyone.”
The Head-to-Head Data
SURMOUNT-5 (NEJM 2024)
The first head-to-head trial comparing both drugs specifically for obesity. At 72 weeks, tirzepatide produced 20.2% average body weight reduction vs. 13.7% for semaglutide. This is the single most relevant study for weight-loss patients considering the switch.
SURPASS-2 (NEJM 2021)
The landmark trial in patients with type 2 diabetes. Tirzepatide was superior to semaglutide 1 mg for both A1C reduction and body weight. Patients on tirzepatide saw greater waist circumference decreases — 7.24 inches vs. 5.12 inches for semaglutide.
Real-world JAMA data
A matched cohort study of over 18,000 patients found tirzepatide users were roughly twice as likely to achieve 10%+ weight loss compared to semaglutide users. This reflects actual clinical practice, not just controlled trial conditions.
What the Numbers Mean for You
If you weigh 220 pounds:
- Semaglutide's 13.7% average (SURMOUNT-5) = ~30 pounds lost
- Tirzepatide's 20.2% average (SURMOUNT-5) = ~44 pounds lost
- That's roughly 14 additional pounds on average
These are averages. Some patients respond better to semaglutide. Some see equivalent results on both. The trial data tells you the odds favor tirzepatide, but your body gets the final vote.
Blood Sugar Control (For Readers with Type 2 Diabetes)
If you're managing diabetes: tirzepatide has shown A1C reductions up to 2.4% in clinical trials, compared to 1.5–1.8% for semaglutide at comparable doses. A retrospective study of patients who switched from semaglutide 1.0 mg to tirzepatide 10 mg showed a significant additional A1C reduction of 0.7% within 3 months.
How Much Does Tirzepatide Cost? (2026 Pricing)
With insurance, copays can be $25–150/month. Self-pay through LillyDirect starts at $299/month. Compounded options through telehealth start in the $250–400/month range.
| Access Path | Type | Starting Price | What's Included |
|---|---|---|---|
| Ro Body Program | FDA-approved Zepbound + insurance support | $45 first month, then $145/mo membership + medication | Insurance concierge, coaching, progress tracking |
| LillyDirect (self-pay) | FDA-approved Zepbound | $299/mo (2.5 mg) | Manufacturer direct, Lilly-approved pharmacy |
| MEDVi | Compounded + FDA-approved options | Varies by medication | Physician eval, medication, shipping, provider access |
| Eden | Compounded + brand-name | ~$249–349/mo | Board-certified providers, coaching |
| SkinnyRx | Compounded | ~$199–299/mo | Telehealth consult, medication, shipping |
| Retail pharmacy (brand) | FDA-approved Zepbound | ~$1,086/mo list price | Prefilled pen, pharmacy pickup, insurance may cover |
All prices verified April 2026. Compounded tirzepatide is not FDA-approved. Always verify current pricing directly with providers.
Three Paths to Tirzepatide — Pick Yours
Path 1: You have insurance
Start with Ro. Their insurance concierge checks whether your plan covers Zepbound and handles prior authorization paperwork. If approved, your copay could be significantly lower than cash-pay. If brand-name coverage is denied, Ro also offers compounded options as a backup.
Let Ro Check Your Zepbound Coverage →Path 2: FDA-approved, no insurance
LillyDirect's self-pay program ships Zepbound directly to your door starting at $299/month for 2.5 mg. No middleman, no compounding pharmacy — brand-name medication from Lilly-approved pharmacies. Higher doses run $399–449/month.
Path 3: Cash-pay, compounded option
MEDVi offers both compounded and FDA-approved GLP-1 medications, with physician evaluation and ongoing provider access included. 4.4 stars on Trustpilot from thousands of reviews.
See MEDVi's Current Tirzepatide Options →Compounded vs. FDA-Approved: What You Need to Know
FDA-approved tirzepatide (Mounjaro, Zepbound) has been tested for safety, effectiveness, and manufacturing quality through rigorous clinical trials. It comes in prefilled pens at fixed, verified doses.
Compounded tirzepatide is prepared by licensed compounding pharmacies when prescribed by a provider. It is not FDA-approved — the FDA does not verify the safety, effectiveness, or quality of compounded drugs before they are marketed. The regulatory landscape around compounded GLP-1s has tightened considerably in 2026.
Switching from Compounded Semaglutide to Tirzepatide
If your compounded semaglutide supply was disrupted, take a breath. You have clear options.
The switching protocol is the same regardless of whether your semaglutide was compounded or brand-name. Stop the medication, wait about a week, start tirzepatide at 2.5 mg under your provider's plan.
One wrinkle: compounded semaglutide doses don't always match standard FDA-approved dose levels. When you connect with a new provider for tirzepatide, tell them your exact compounded dosing — the concentration on the vial label, the number of units you drew, and the milligram equivalent. This helps them make a more informed decision about your tirzepatide starting dose.
What to Do Right Now If Your Compounded Supply Is Ending
- 1Don't panic-buy from unverified sources. The FDA has issued multiple warnings about fraudulent GLP-1 products sold online. Stick with licensed, reputable providers.
- 2Check your insurance. You may qualify for brand-name coverage you didn't have before. Ro's concierge can check this for you.
- 3Consider the self-pay FDA-approved path. LillyDirect now offers Zepbound starting at $299/month — closer to compounded pricing than most people realize.
- 4Bring your compounded prescription details to your new provider — vial concentration, units per dose, injection frequency. This is critical for them to assess your history accurately.
Brand-Name Switching Scenarios
Ozempic to Mounjaro
Same switching protocol. Both are FDA-approved for type 2 diabetes. The main variable is insurance: check whether Mounjaro is on your plan's formulary before switching, as coverage can differ significantly from Ozempic.
Wegovy to Zepbound
Both are FDA-approved for weight management. Zepbound coverage for obesity is less established than Wegovy at many insurers — so verify before you switch. If your plan covers it, this is the strongest clinical upgrade available: same injection routine, potentially better results.
Can You Switch Back?
Yes. The process works in reverse. Finish your last tirzepatide dose, wait about a week, and start semaglutide on your next injection day. Your provider determines your re-entry dose. Some patients try tirzepatide and find they prefer semaglutide — the goal is finding the medication that delivers the best results for your body while being tolerable long-term.
I Switched from Semaglutide to Tirzepatide and I'm Not Losing Weight
If you're in the first 8 weeks, don't panic. If you're past week 12 on an adequate dose and nothing has changed, it's time to reassess.
Weeks 1–8 (2.5 mg → 5 mg)
You're on initiation and early titration doses. These are intentionally low. Weight loss at this stage is modest or flat for most patients — even those who will eventually see excellent results. Think of this as building a foundation.
Weeks 9–16 (7.5 mg → 10 mg)
This is typically when weight loss accelerates. If you're still flat at the end of this window, bring it up with your provider. They may continue titrating, review your diet and activity, or check thyroid function and other metabolic markers.
Past 16 weeks on 10 mg+ with no progress
Tirzepatide may not be the right fit for you. That's okay. Not every medication works for every body, and returning to semaglutide — or exploring other options — is a legitimate clinical decision.
Key insight: Do not abandon tirzepatide after 4 weeks at 2.5 mg and conclude it doesn't work. You haven't given it a real chance yet. The clinical trials that showed 20% body weight loss ran for 72 weeks. The medication rewards patience and consistent titration.
How to Maximize Your Results After Switching
Tirzepatide is powerful — but it's not magic. The clinical trials that produced those 20% body weight loss numbers weren't medication-only. Every participant also followed a reduced-calorie diet and increased physical activity.
Protein Is Non-Negotiable
Aim for 30g+ of protein per meal. Good sources: chicken, turkey, fish, Greek yogurt, eggs, tofu, cottage cheese, protein shakes. This is the single highest-leverage dietary habit during the switch.
Strength Training Preserves Muscle
Resistance training 2–3× per week signals your body to preserve muscle while shedding fat. Bodyweight exercises, resistance bands, or dumbbells at home are enough.
Stay Hydrated — More Than You Think
Target 64+ ounces of water daily. GLP-1 medications slow gastric emptying. Dehydration makes every GI side effect worse.
Track Your First 90 Days
Weigh yourself weekly (same day, same time). Track your appetite 1–10. Note any side effects. This data is invaluable for your provider at follow-up appointments.
Don't Let Perfect Be the Enemy of Progress
Some weeks the scale won't move. The trajectory over months is what matters — not day-to-day fluctuations. The medication does the heavy lifting on appetite; your job is protein, movement, hydration, and patience.
What to Ask Your Doctor Before Switching
Walking into a provider appointment with specific questions gets you a better plan and faster answers:
- 1Based on my history with semaglutide, should I start tirzepatide at 2.5 mg or is 5 mg reasonable?
- 2Should I wait longer than one week between medications given my current side effects?
- 3Do you recommend any blood work or monitoring before or after the switch?
- 4If I have type 2 diabetes: how should I adjust blood sugar monitoring during the transition?
- 5Does my insurance cover Zepbound, and what's the prior authorization process?
- 6What's the plan if tirzepatide doesn't work for me — can I switch back?
- 7I'm on oral hormonal contraceptives — do I need backup contraception during initiation?
- 8Are there any medications I'm taking that interact differently with tirzepatide?
Copyable Message Template for Your Provider
Hi [Provider Name],
I'm currently on [semaglutide dose] ([Ozempic/Wegovy/compounded]) and I'd like to discuss switching to tirzepatide. My reasons: [plateau for X weeks / side effects / want stronger results / insurance change / compounded supply disrupted].
Questions I'd like to cover:
1. Should I start tirzepatide at 2.5 mg or could 5 mg work for me given my tolerance history?
2. Can I start on my next scheduled injection day, or should I wait longer?
3. Do I need any labs before starting?
4. What should I monitor during the first month?
My current weight is [X], my height is [X], and I [do/do not] have type 2 diabetes. I've been on semaglutide for [X months] and my current side effects are [none / mild nausea / etc].
What People Are Saying About the Switch
Paraphrased from real community posts on Reddit, Mayo Clinic Connect, and patient forums — representative of the most common switching experiences.
“I stalled at 180 on semaglutide for three months. Switched to tirzepatide, and in the first 12 weeks I dropped another 18 pounds. Wish I’d switched sooner.”
— Paraphrased from r/tirzepatidecompound
“The first couple weeks on 2.5 were rough — I was way hungrier than I’d been on Wegovy. But once I hit 5 mg, the appetite suppression came back stronger than before.”
— Paraphrased from r/Mounjaro
“I had terrible nausea on semaglutide that never fully went away. On tirzepatide, the side effects have been way more manageable. Different drug, different experience.”
— Paraphrased from Mayo Clinic Connect
Where to Get Tirzepatide Prescribed Online
For FDA-Approved Tirzepatide with Insurance Support
Ro Body Program
Ro is the strongest option if you have insurance or want FDA-approved medication. Their program includes an insurance concierge that checks your Zepbound coverage and handles prior authorization, plus coaching, progress tracking, and compounded options as a backup if brand-name coverage is denied. Ro doesn't offer the absolute lowest cash-pay price — but because it includes FDA-approved access, insurance work, and clinical support built for patients switching between GLP-1 medications, it's the most complete option for exactly what you're doing.
Check Your Zepbound Coverage on Ro →For Cash-Pay or Flexible Options
MEDVi
MEDVi has expanded beyond compounded medications to now include FDA-approved GLP-1 options. They offer physician evaluation, medication access, and ongoing provider support through a cash-pay model with no long-term contracts. 4.4 stars on Trustpilot from thousands of reviews. Check current pricing and available medications directly — their platform continues to evolve.
See Current MEDVi Tirzepatide Options →
Not Sure Which Path Is Right?
Answer a few questions about your goals, insurance, and budget — get matched with the right medication and provider in 60 seconds. No commitment, no spam.
Get Your Personalized GLP-1 Switch Plan — Free →How We Verified This Guide
- •FDA prescribing information for Zepbound (tirzepatide), Mounjaro, Wegovy, and Ozempic
- •SURMOUNT-5 — Tirzepatide vs. semaglutide head-to-head for obesity (NEJM 2024)
- •SURPASS-2 — Tirzepatide vs. semaglutide for type 2 diabetes (NEJM 2021)
- •STEP-1 — Semaglutide for obesity
- •Published switching guidance: Whitley HP et al., Clinical Diabetes 2023; BILH GLP-1RA Conversion Guide; Almandoz J et al., Clinical Diabetes 2020
- •Real-world data: JAMA matched cohort study; prospective switch study (Diabetes, Obesity and Metabolism)
- •FDA safety communications on compounded GLP-1 medications
- •Provider pricing verified directly on Ro, MEDVi, Eden, SkinnyRx, and LillyDirect websites as of April 2026
We are an affiliate partner with some providers listed on this page. When you sign up through our links, we may earn a commission at no additional cost to you. This never influences our rankings, recommendations, or editorial content. This article is reviewed monthly. Last verified: April 1, 2026.
This page is not medical advice. It is an evidence-based educational resource. Always consult a licensed healthcare provider before starting, stopping, or switching any medication.
Frequently Asked Questions
Can I switch from semaglutide to tirzepatide on my next injection day?
Yes. Take your last semaglutide dose, then start tirzepatide about 3–10 days later, commonly on your next scheduled injection day. Most providers do not require a formal washout period.
Do I need to taper off semaglutide before switching?
No tapering is needed. Complete your current dose on schedule and switch directly. Semaglutide has a roughly 7-day half-life and clears naturally over the following weeks.
What tirzepatide dose should I start on after semaglutide?
The label-based starting dose is 2.5 mg once weekly for 4 weeks. Some providers may discuss starting at 5 mg for patients who tolerated high-dose semaglutide well, but this is a clinical decision — not the default.
Is there an equivalent semaglutide to tirzepatide dose?
No validated dose-equivalence chart exists. These drugs use different mechanisms and titration schedules and are not milligram equivalents. Any site giving you a clean mg-to-mg conversion is making it up.
Can I take semaglutide and tirzepatide at the same time?
No. The Zepbound label states that coadministration with another GLP-1 receptor agonist is not recommended. Do not overlap these medications.
What if I switched and feel hungrier on 2.5 mg?
This is normal and temporary. You're going from a high semaglutide dose to a low tirzepatide initiation dose. Appetite suppression typically returns and often strengthens by weeks 5–8 as the dose increases.
Will I regain weight during the switch?
Weight regain during the transition is uncommon. A brief plateau or minor fluctuation during the first 2–4 weeks is possible as your tirzepatide dose builds up, but this resolves as you titrate.
Is tirzepatide better than semaglutide for weight loss?
On average, yes. In the SURMOUNT-5 head-to-head trial, tirzepatide produced 20.2% body weight loss vs. 13.7% for semaglutide at 72 weeks. Individual results vary — some people do better on semaglutide.
Does insurance cover switching from Wegovy to Zepbound?
Coverage varies widely by plan. Zepbound coverage for weight loss is less established than Wegovy at some insurers. Ro's insurance concierge can check your specific coverage before you switch.
How long until I see results after switching?
Most patients notice renewed appetite suppression by weeks 5–8 and meaningful weight loss by weeks 9–16. Maximum benefit is typically seen after 9–12 months of consistent use.
Do I need to worry about oral contraceptives when starting tirzepatide?
Yes. Tirzepatide can reduce the effectiveness of oral hormonal contraceptives for 4 weeks after initiation and 4 weeks after each dose increase. Use a backup method or discuss non-oral contraception with your provider.
Can I switch from oral semaglutide (Rybelsus) to tirzepatide injections?
Yes. The switching principle is the same. Your provider will consider your current Rybelsus dose and plan your tirzepatide start date. Transition timing may differ slightly since you're going from a daily oral to a weekly injection.
What if my doctor won't prescribe tirzepatide?
Options include seeking a second opinion, trying a telehealth platform like Ro that specializes in GLP-1 prescriptions, or asking your provider specifically what concerns they have — it may be addressable.
Is tirzepatide safe long-term?
Tirzepatide has been studied for up to 176 weeks (about 3.4 years) in clinical trial extensions. Both tirzepatide and semaglutide carry the same boxed warning about thyroid C-cell tumors (observed in rodent studies) and similar contraindications. No new long-term safety signals have emerged beyond what was identified in the registration trials.
Should I switch just because tirzepatide has better trial results?
Not necessarily. If semaglutide is giving you consistent results, tolerable side effects, and good lab numbers, switching may not be worth the cost difference and adjustment period. Switch when there's a reason — not because of hype.
Still not sure which GLP-1 program is right for you?
Free 60-second quiz that matches you with the right medication, provider, and pricing for your situation. No commitment, no spam — just your personalized next step.
Take the Free GLP-1 Matching Quiz →