Medical disclaimer: This article is for informational purposes only and is not medical advice. Zepbound (tirzepatide) is a prescription medication. Always work with a licensed healthcare provider before starting, stopping, or switching any medication.
How to Switch From Semaglutide to Zepbound
Yes, you can switch from semaglutide to Zepbound. A common clinician-guided approach: take your last semaglutide dose on schedule, do not overlap the two drugs, and start Zepbound on your next weekly injection day. The labeled starting dose is 2.5 mg once weekly for 4 weeks — though some GLP-1–experienced patients are started at 5 mg by their prescriber.
There is no official semaglutide-to-Zepbound conversion chart (despite what some pages online claim). And for many people, the switch is worth it: in a 72-week head-to-head trial, Zepbound produced roughly 20.2% average body weight loss compared to 13.7% for semaglutide.
This guide covers timing, dose, cost across every access path, what to expect in the first month, and exactly what changes if you're switching from Ozempic, Wegovy, Rybelsus, or compounded semaglutide.
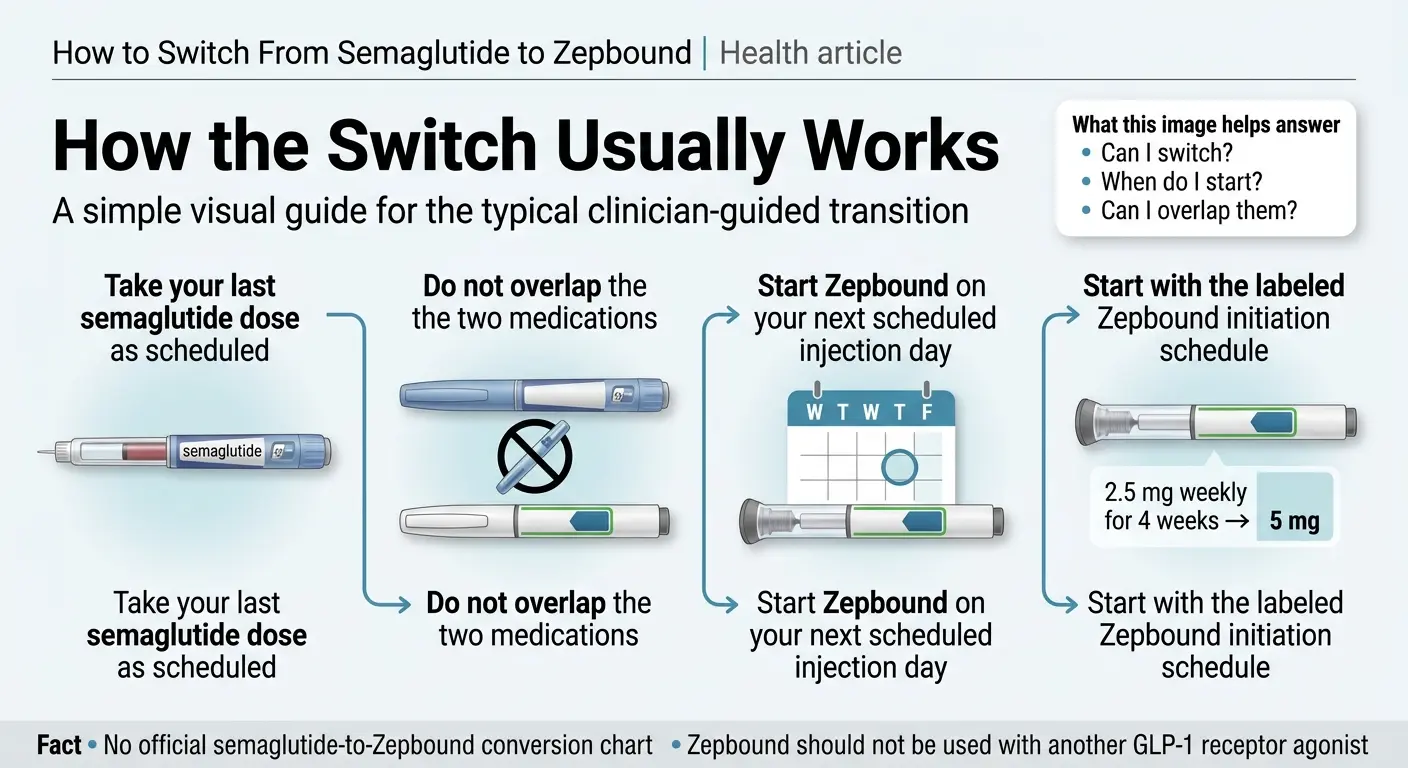
No official semaglutide-to-Zepbound conversion chart exists. Zepbound should not be used with another GLP-1 receptor agonist.
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
Quick Reference
All pricing verified April 2026 via Eli Lilly's official sources. Savings Card terms valid through December 31, 2026.
Eligibility confirmed within ~2 days. PA support included.
Why Are People Switching From Semaglutide to Zepbound?
Most people switch from semaglutide (Wegovy, Ozempic, or compounded) to Zepbound for one of four reasons: they've plateaued, they've seen the head-to-head clinical data, their insurance changed formularies, or their compounded semaglutide supply disappeared.
The clinical case is real. Semaglutide activates one hormone receptor (GLP-1) to suppress appetite and regulate blood sugar. Zepbound activates two — GLP-1 and GIP. That dual mechanism is why the clinical numbers consistently favor tirzepatide:
- SURMOUNT-5 trial (NEJM, 2025): Zepbound produced 20.2% average body weight loss vs. 13.7% for Wegovy over 72 weeks. 31.6% of Zepbound patients lost at least 25% of their body weight, compared to 16.1% on Wegovy.
- JAMA real-world study (Rodriguez et al., 2024): Among 18,000+ matched patients, tirzepatide users lost roughly 15.3% body weight at 12 months, compared to 8.3% for semaglutide users.
Many patients also report that Zepbound does a better job silencing "food noise" — those intrusive thoughts about eating that semaglutide reduced but didn't eliminate. This is anecdotal, not proven in controlled trials, but it shows up consistently in patient forums.
The honest tradeoff, upfront
Zepbound does not have semaglutide's cardiovascular risk reduction indication. Wegovy is FDA-approved to reduce the risk of heart attack, stroke, and cardiovascular death in certain adults. Zepbound is not. If reducing cardiovascular risk is a primary reason you're on semaglutide, that matters — your prescriber should weigh in before you switch.
"I was super nervous about switching. I am seeing WAY better results and way less side effects." — Reddit user, r/tirzepatidecompound
Plateaued on semaglutide?
Ro can start your switch, including prior authorization support.
How to Switch From Semaglutide to Zepbound in 5 Steps
Switching is a structured but straightforward process. Most of the anxiety comes from conflicting information online — not from the actual switch being complicated.
Talk to Your Prescriber
This isn't a disclaimer — it's the literal first step. Your prescriber needs to confirm Zepbound is appropriate for your indication, decide your starting dose, handle prior authorization if you're going through insurance, and write the prescription. If you're using a telehealth provider like Ro, this conversation happens over messaging — no in-person visit needed.
Take Your Last Semaglutide Dose on Schedule
No taper needed. Just take your final dose as planned and note the date. Semaglutide has a half-life of approximately 7 days, meaning it stays active in your system and declines gradually. That built-in buffer works in your favor — you won't suddenly lose appetite suppression the day after your last shot.
Start Zepbound on Your Next Injection Day
Begin Zepbound approximately one week after your last semaglutide dose — on your next regular injection day. This keeps your weekly rhythm intact and avoids overlapping two GLP-1 medications. Zepbound's prescribing information states it should not be coadministered with another GLP-1 receptor agonist. Don't take both in the same week.
Begin at the Correct Starting Dose
Zepbound's labeled initiation dose is 2.5 mg once weekly for 4 weeks, then 5 mg. Your prescriber may start you at 5 mg if you tolerated high-dose semaglutide well and have no history of significant GI side effects. This is individualized clinical judgment — not something to self-prescribe based on an internet chart.
Track Your First Month Closely
Keep a simple log of appetite changes, GI side effects, energy levels, and weight (weekly, not daily). This gives your prescriber real data for your first follow-up and helps calibrate your titration schedule. If something feels off — persistent vomiting, severe abdominal pain, or signs of dehydration — contact your prescriber. Don't just push through.
What Dose of Zepbound Should You Start On?
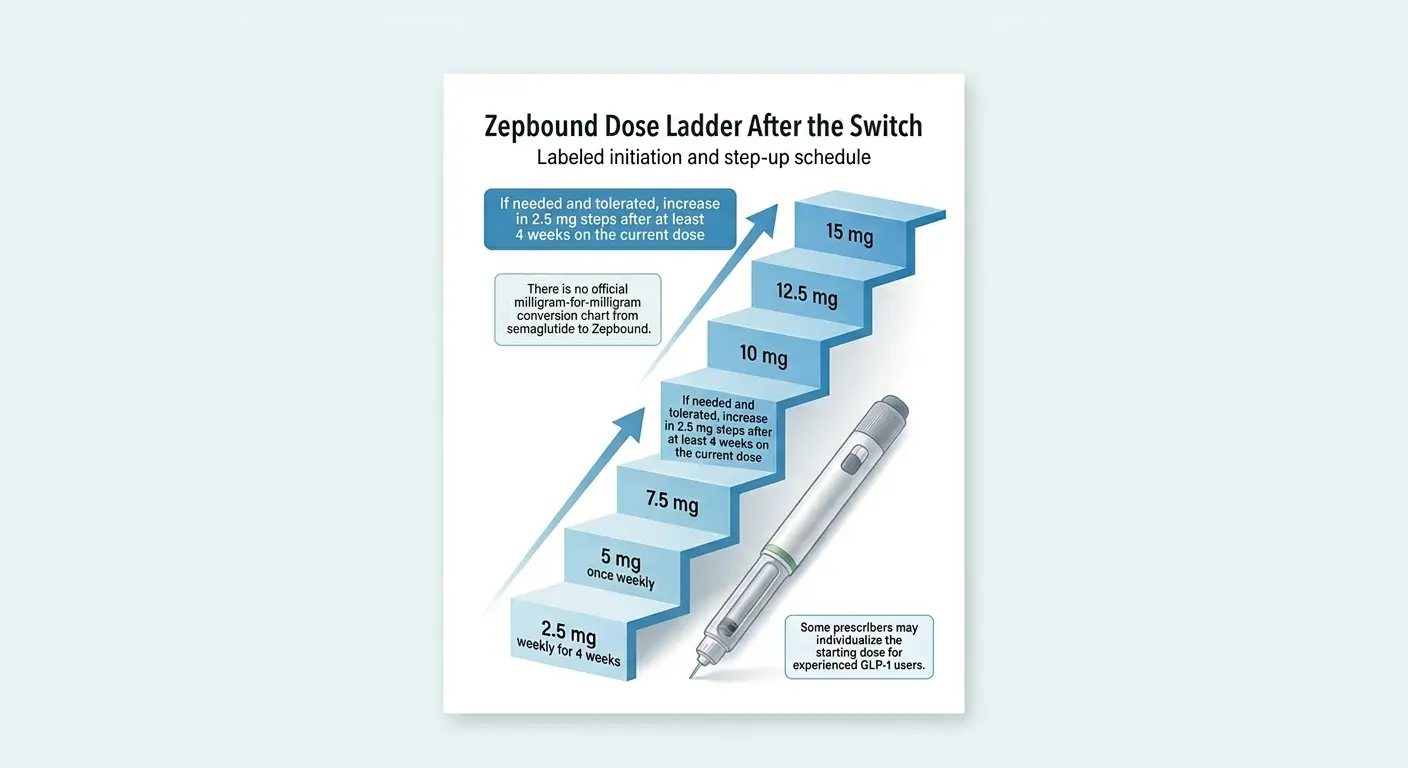
There is no official milligram-for-milligram conversion chart from semaglutide to Zepbound. Some prescribers may individualize the starting dose for experienced GLP-1 users.
The labeled Zepbound initiation dose is 2.5 mg once weekly for 4 weeks, followed by an increase to 5 mg. From there, titration increases by 2.5 mg increments every 4+ weeks: 5 mg → 7.5 mg → 10 mg → 12.5 mg → 15 mg.
Some GLP-1–experienced patients — particularly those who tolerated max-dose semaglutide with minimal side effects — are started at 5 mg. This is within clinical practice norms but is not the default label recommendation.
Why 2.5 mg can feel "too low": If you were on 2.4 mg Wegovy or 2.0 mg Ozempic, dropping to 2.5 mg Zepbound can feel like going backward. Your appetite may temporarily feel less suppressed. This is normal and expected. Most patients who feel underwhelmed at 2.5 mg report significant improvement once they reach 5 mg or 7.5 mg.
| Your Situation | Starting Dose to Discuss | Why |
|---|---|---|
| Tolerated semaglutide well, minimal GI issues | Ask about 5 mg | Lower risk of restarting at the bottom |
| Had significant nausea/GI on semaglutide | Lean toward 2.5 mg | Different drug, but GI sensitivity may carry |
| Anxious about the switch | 2.5 mg | Safer baseline, build confidence |
| Coming off a lower semaglutide dose (0.25–0.5 mg) | 2.5 mg | Standard initiation |
| Want the labeled, lowest-risk approach | 2.5 mg | What Lilly's prescribing info recommends |
Is There a Semaglutide to Zepbound Conversion Chart?
No official, validated milligram-for-milligram conversion chart exists between semaglutide and Zepbound. Several pages currently ranking for this query publish "suggested equivalent dosages" or "dose conversion tables." These are unofficial.
Lilly's prescribing information gives a titration schedule — 2.5 mg for 4 weeks, then escalate — not an equivalence map to semaglutide. The FDA has not published one either. And there's a good reason: semaglutide and tirzepatide work through fundamentally different mechanisms (single vs. dual receptor), so milligram comparisons don't translate meaningfully.
Ask these instead of "what's the equivalent dose?"
- Should I start at 2.5 mg or 5 mg based on my semaglutide history?
- How quickly can I titrate up if 2.5 mg feels inadequate?
- What's the realistic timeline to reach a therapeutic dose?
"Did it make a difference in appetite control, cravings, or weight loss? Is it worth the higher cost?" — Reddit, r/Zepbound
Cost is the deciding factor?
Check current Zepbound pricing and coverage options on Ro.
When Should You Start Zepbound After Your Last Semaglutide Dose?
The practical answer: start Zepbound on your next scheduled injection day, typically about 7 days after your last semaglutide dose. This is the most common clinician-guided approach and avoids both overlapping the drugs and creating an unnecessary gap.
You do not need a 4–5 week "full washout." This claim circulates online and is based on a misunderstanding of semaglutide's pharmacokinetics. You're not adding the two drugs together at peak levels — you're starting a low dose of a different drug as the first one tapers off naturally.
| Claim | Reality |
|---|---|
| You must wait 4–5 weeks for a full washout | Not a standard clinical recommendation for most patients |
| You can overlap them for a week to avoid a gap | No — Zepbound's label says don't coadminister with another GLP-1 agonist |
| You need to taper semaglutide before switching | Usually not — just take your last dose and start Zepbound when scheduled |
| Start Zepbound the very next day | Too aggressive for most — waiting until your next injection day is standard |
What if your schedule is irregular? If you missed your last semaglutide dose or you're not on a strict weekly cadence, tell your prescriber. They'll help you pick a reasonable start date based on when your last actual dose was.
What if you already have Zepbound in the fridge? Don't start it early out of excitement. Wait until you've had the prescriber conversation. Room-temperature storage for single-dose pens and single-dose vials is up to 21 days (up to 86°F); the multi-dose KwikPen may be stored at room temperature for up to 30 days once in use. Check the label for your specific device.
Switch Rules by Your Current Semaglutide Type
"Switching from semaglutide to Zepbound" is actually four different conversations depending on what you're currently taking.
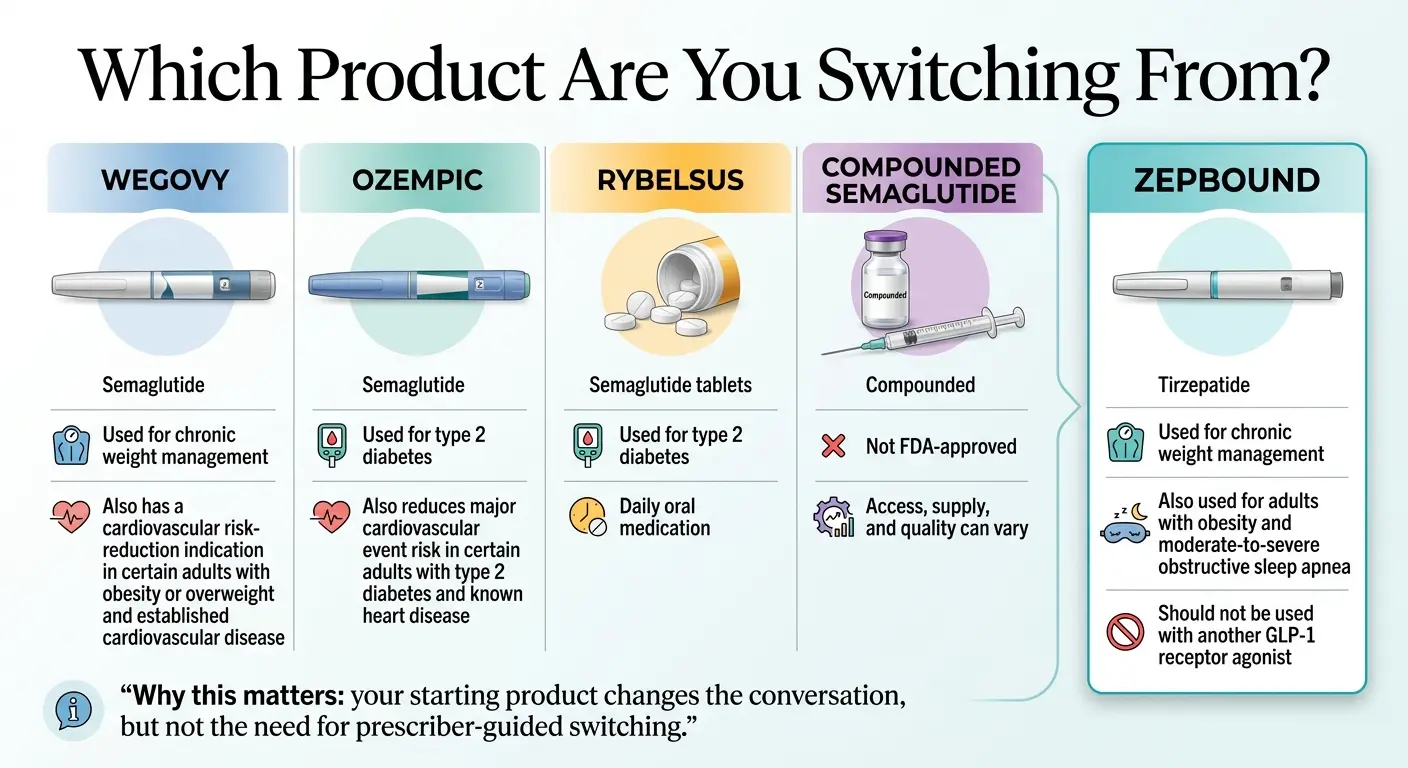
"Why this matters: your starting product changes the conversation, but not the need for prescriber-guided switching."
If You're Switching From Wegovy to Zepbound
This is the most straightforward switch. Both are FDA-approved for chronic weight management. Last Wegovy dose → wait ~7 days → start Zepbound 2.5 mg or 5 mg.
Key detail: Wegovy's maintenance dose is 2.4 mg. Zepbound starts at 2.5 mg. These are NOT equivalent — different drugs, different mechanisms. You're starting a new medication at its initiation dose and will titrate up.
Insurance note: If your plan covers Wegovy, it may or may not cover Zepbound — they're made by different manufacturers (Novo Nordisk vs. Eli Lilly) with different formulary positions. Check before you switch.
If You're Switching From Ozempic to Zepbound
Ozempic is FDA-approved for type 2 diabetes, not weight loss. The timeline and dosing process are identical to the Wegovy scenario.
Important question most pages skip: If your primary reason for semaglutide is type 2 diabetes — not weight loss — discuss whether Mounjaro (not Zepbound) is the right tirzepatide product. Mounjaro is Eli Lilly's tirzepatide approved for type 2 diabetes. Same active ingredient, different FDA indication — and the indication matters for insurance coding and coverage.
If You're Switching From Rybelsus to Zepbound
Rybelsus is oral semaglutide — a daily tablet for type 2 diabetes. You're going from a daily pill to a weekly injection and from a single-receptor drug to a dual-receptor drug.
Semaglutide itself still has a roughly 1-week half-life regardless of how it's administered. Because Rybelsus is taken daily rather than weekly, the scheduling discussion feels different — your prescriber will set the specific transition timing.
If You're Switching From Compounded Semaglutide to Zepbound
This switch has an extra layer. Compounded semaglutide is not FDA-approved. After the FDA resolved the semaglutide shortage and compounding rules tightened through 2025, many people's compounded supply ended or became unreliable.
The switching protocol (timing, starting dose) is the same. What's different is access — you'll need a prescriber relationship and will need to navigate insurance or self-pay from scratch. See our dedicated guide: How to Switch From Compounded Semaglutide to Zepbound →
How Much Does Zepbound Cost in 2026?
Cost is the make-or-break question for most switchers. Here's every current access path, verified April 2026.
| Access Path | 2.5 mg/mo | 5 mg/mo | 7.5–15 mg/mo | Notes |
|---|---|---|---|---|
| Lilly self-pay (vials) | $299 | $399 | $449 | Must refill within 45 days for promo pricing. Vials require syringe draw. |
| Lilly self-pay (KwikPen) | — | — | $449 | KwikPen promo launched Feb 2026. Easier than vials, same price. |
| Commercial insurance + Savings Card | As low as $25 | As low as $25 | As low as $25 | Eligible commercially insured patients. Up to $1,300/year savings cap. Card valid through Dec 31, 2026. |
| Commercial insurance, no Savings Card | Varies | Varies | Varies | Many plans require prior authorization. |
| Retail pharmacy (no discount) | ~$1,086 | ~$1,086 | ~$1,086 | List price. Discount programs may reduce cost. |
| Medicare GLP-1 Bridge | See note | — | — | Jul 1–Dec 31, 2026. KwikPen only. $50 copay for eligible beneficiaries. Outside Part D. |
| Ro (telehealth) | Included | Included | Included | $45 first month, $145/mo ongoing. Insurance concierge + PA support included. |
Sources: pricinginfo.lilly.com, zepbound.lilly.com/coverage-savings, ro.co, cms.gov. All pricing verified April 7, 2026. Subject to program terms.
HSA and FSA eligible: Zepbound is a prescription medication, so HSA/FSA funds can typically be used for purchase.
Comparison to what you're paying now: On Lilly's self-pay path, Zepbound vials start at $299/month — often below what patients were paying for Wegovy through similar self-pay programs.
Will My Insurance Cover the Switch to Zepbound?
Many commercial insurance plans cover Zepbound, but most require prior authorization. If you're already on semaglutide and switching due to a plateau or inadequate response, prior authorization often goes smoothly because you have a documented treatment history.
What your prescriber needs to document for prior auth:
- You've been on semaglutide at dose X for Y months
- You've experienced [plateau / inadequate weight loss / intolerable side effects / supply disruption]
- Switching to tirzepatide (Zepbound) is medically appropriate for your condition
- BMI and relevant comorbidities
Many commercial plans have a pathway for "step therapy failure" documentation. Some telehealth providers, including Ro, handle prior authorization as part of their standard workflow.
If your claim is denied: You can appeal. And if insurance truly won't cover Zepbound, Lilly's self-pay path starting at $299/month is the fallback — no insurance required.
Medicare note: Traditional Medicare Part D generally does not cover Zepbound for weight loss as of April 2026. However, CMS has announced the Medicare GLP-1 Bridge, running July 1, 2026 through December 31, 2026. The Bridge includes Zepbound KwikPen only (not vials), with a $50 copay for eligible beneficiaries. The Bridge operates outside Part D.
Is Zepbound Actually Better Than Semaglutide?
On average, yes — for weight loss. But "better on average" is not the same as "better for every person."
What the data says: The SURMOUNT-5 trial is the only completed head-to-head comparison of tirzepatide vs. semaglutide for weight loss (NEJM, 2025):
- Zepbound: ~20.2% average body weight loss over 72 weeks
- Wegovy: ~13.7% average body weight loss over 72 weeks
- 31.6% of Zepbound patients lost ≥25% body weight vs. 16.1% on Wegovy
- Side effect profiles were comparable
For perspective: if you weigh 220 pounds, the average difference is approximately 44 pounds lost on Zepbound vs. 30 pounds on Wegovy. That 14-pound gap is clinically meaningful.
When it may not be worth switching
- You're losing weight steadily on semaglutide and haven't plateaued
- Your cardiovascular risk profile makes Wegovy's CV indication especially important
- Zepbound isn't covered by your insurance and the cost difference is prohibitive
- You have severe GI sensitivity and worry about adjusting to a new medication
What to Expect in the First 4 to 8 Weeks After Switching
The most common post-switch queries are "is 2.5 mg Zepbound doing anything?" and "I feel hungrier after switching — is this normal?" Yes and yes.
Week 1
Your last semaglutide dose is still declining. You've taken your first Zepbound injection. Most people feel relatively normal. Some notice mild nausea, usually less severe than when they first started semaglutide. If you came from a high semaglutide dose, appetite suppression may feel slightly weaker — this is temporary.
Week 2
GI side effects, if they occur, typically peak here. Common reports: mild nausea, stomach discomfort, occasional constipation. These tend to be milder than the initial semaglutide startup. Appetite suppression should be returning. Some patients notice Zepbound's dual mechanism feels 'different' — not just less hunger, but less mental fixation on food.
Weeks 3–4
Side effects resolving for most people. Appetite control normalizing or improving. If you started at 2.5 mg, you'll likely increase to 5 mg at the 4-week mark if tolerated. Many patients describe 5 mg as when Zepbound 'kicks in' for real.
Weeks 5–8
Titration continues. Weight loss trajectory establishing. The dual GLP-1/GIP mechanism is fully engaged. Most patients who were initially skeptical report noticeable differences by this point.
| Normal | Contact your prescriber |
|---|---|
| Mild nausea in weeks 1–2 | Persistent vomiting that prevents eating for 24+ hours |
| Slightly increased appetite initially | Severe abdominal pain |
| Minor constipation or soft stool | Signs of dehydration (dark urine, dizziness) |
| Injection site redness | Allergic reaction symptoms |
| Feeling 'underwhelmed' at 2.5 mg | Rapid, unexplained changes in vision |
"I recently switched to Zepbound after stalling on semaglutide. Week one has been rough — the food noise came back hard." — Reddit, r/Zepbound
Some people do have a rocky first week or two. But many patients report that by week 3–4, things improve — often significantly. The key is not to panic during the transition window.
Fastest Legitimate Ways to Get Zepbound
The answer depends on your insurance status and how much administrative friction you're willing to handle.
| Access Path | Best For | Monthly Cost | PA Support? | Timeline |
|---|---|---|---|---|
| Ro | Most people — especially if you need insurance help | $45 first month, $145 ongoing + medication cost | Yes — insurance concierge included | Eligibility confirmed ~2 days; medication ships after PA |
| Your current prescriber + LillyDirect | People who already have a doctor and want self-pay | $299–$449/mo (vials) | You handle PA yourself | Depends on prescriber availability |
| Local obesity medicine specialist | People who want in-person care and monitoring | Insurance copay or $299–$449/mo self-pay | Varies by practice | Depends on appointment availability |
| PCP or endocrinologist | People already in the system who just need a new Rx | Insurance copay or self-pay | Usually yes, but may be slow | Often 2–4 weeks for non-urgent appointments |
Our recommendation for most readers: For people who want an integrated telehealth route with prior-authorization help, Ro is one of the cleaner options we verified. It handles the two biggest friction points — getting the prescription written quickly and navigating prior authorization — as part of its standard workflow.
Ro does not work for Medicare, Medicaid, or government plans.
Prefer another telehealth option?
MEDVi also offers GLP-1 prescriptions including Zepbound — another licensed provider to consider.
What Not to Do When Switching From Semaglutide to Zepbound
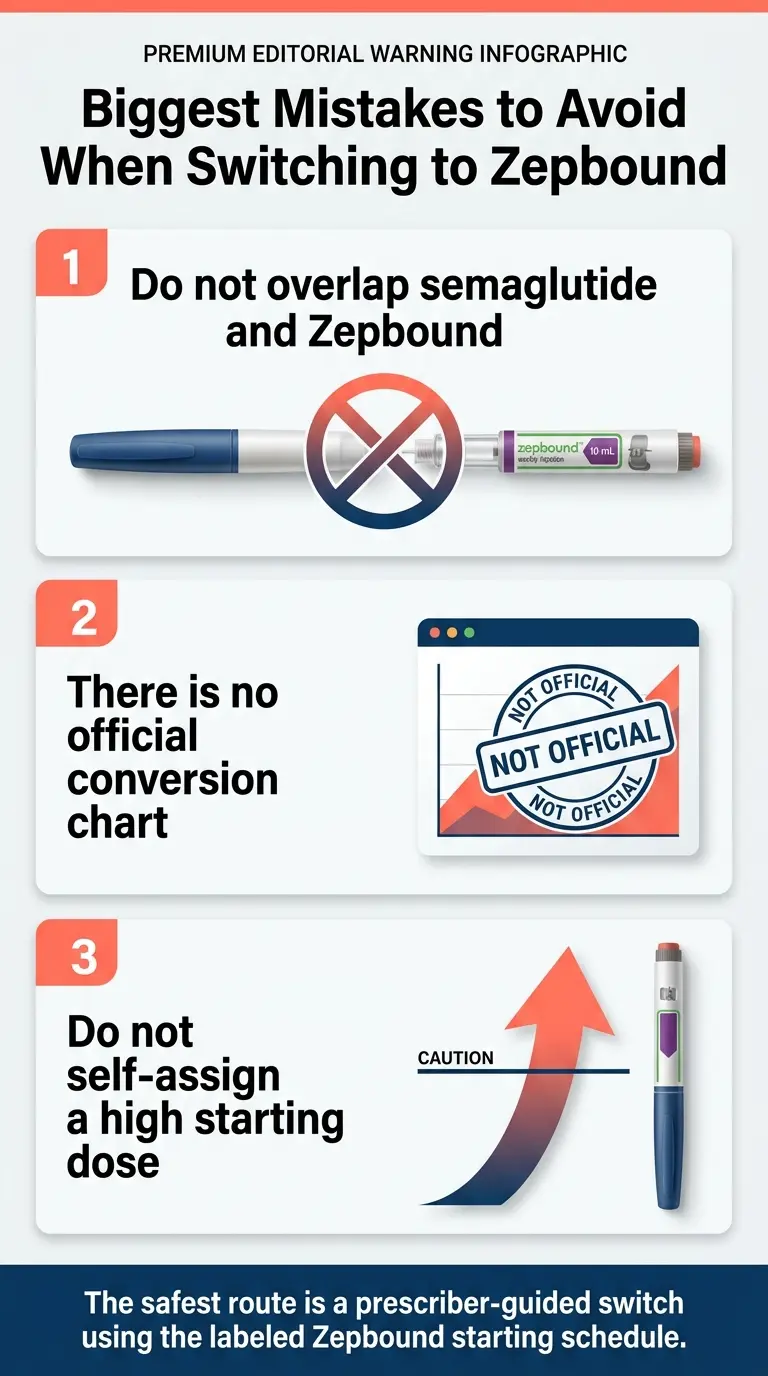
Don't overlap the drugs.
Zepbound should not be coadministered with another GLP-1 receptor agonist. Not for one week, not for one dose, not 'just to bridge.' The prescribing information is unambiguous.
Don't self-prescribe your starting dose based on internet charts.
There is no official semaglutide-to-Zepbound conversion. Starting yourself at 10 mg or 15 mg because you were on max-dose Wegovy is not how this works. Zepbound initiation at 2.5 mg for 4 weeks is the label recommendation.
Don't confuse Zepbound and Mounjaro.
Same active ingredient (tirzepatide), different products. Zepbound is FDA-approved for weight management. Mounjaro is approved for type 2 diabetes. The distinction matters for insurance coding and FDA compliance.
Don't assume your first week tells the full story.
Starting at 2.5 mg after months on high-dose semaglutide can feel anticlimactic. Give it at least 4–8 weeks before judging the switch.
Don't skip the insurance/pricing research until after you've switched.
If your prescriber writes a Zepbound Rx and your pharmacy runs it at retail price (~$1,086), you'll get sticker shock. Check: Does your plan cover Zepbound? Have you enrolled in the Savings Card? Would LillyDirect self-pay be cheaper?
Questions to Ask Your Prescriber Before You Switch
Walk into your prescriber conversation with these questions and you'll get more useful answers than 90% of patients:
- 1Based on my history with semaglutide, should I start Zepbound at 2.5 mg or 5 mg?
- 2Should I take my first Zepbound dose on my next scheduled injection day, or do you want a different gap?
- 3Am I switching to the right tirzepatide product? (Zepbound for weight, Mounjaro for diabetes)
- 4What should I expect in weeks 1–4 so I don't panic?
- 5What's the plan if 2.5 mg feels weak — how quickly can we titrate?
- 6Can you help with prior authorization, or do I need to handle that?
- 7What's my cheapest legitimate access path — insurance, LillyDirect, or something else?
Side Effects, Warning Signs, and When to Pause
Common GI side effects (usually mild, usually temporary):
- Nausea (most common in weeks 1–2, often milder than initial semaglutide startup)
- Diarrhea or constipation
- Stomach discomfort or bloating
- Decreased appetite (this is the point — but it can feel too intense at first)
Practical management:
- Eat smaller meals during weeks 1–2
- Stay well-hydrated — dehydration makes nausea significantly worse
- Prioritize protein even when appetite is low — muscle preservation matters
- Avoid high-fat or greasy meals, which amplify GI effects
Red flags — contact your prescriber:
- Vomiting severe enough to prevent any food or liquid intake for 24+ hours
- Severe or worsening abdominal pain (pancreatitis risk is rare but real)
- Signs of dehydration: very dark urine, dizziness on standing, rapid heartbeat
- Allergic reaction: rash, itching, swelling, difficulty breathing
- Any vision changes
Important safety information
- Pregnancy: The Zepbound label states the drug may cause fetal harm. Discontinue when pregnancy is recognized. Tirzepatide may also affect absorption of oral contraceptives — discuss with your prescriber.
- Thyroid / MEN2 warning: Zepbound carries a boxed warning about risk of thyroid C-cell tumors observed in animal studies. It is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2).
How We Verified This Page
The RX Index is an independent editorial publisher covering GLP-1 medications and telehealth providers. We earn commissions from some providers linked on this page. Our editorial recommendations are based on independent research, verified pricing, and clinical accuracy — not compensation.
| Claim on This Page | Source | Verified |
|---|---|---|
| Starting dose: 2.5 mg weekly for 4 weeks | Zepbound prescribing information (FDA) | Apr 7, 2026 |
| Do not coadminister with another GLP-1 agonist | Zepbound prescribing information (FDA) | Apr 7, 2026 |
| No official semaglutide→Zepbound conversion chart | Lilly labeling / FDA — no such document exists | Apr 7, 2026 |
| SURMOUNT-5: ~20.2% vs ~13.7% weight loss | NEJM, 2025 | Apr 7, 2026 |
| Self-pay: $299 / $399 / $449 by dose | pricinginfo.lilly.com/zepbound | Apr 7, 2026 |
| Savings Card: as low as $25 per fill | zepbound.lilly.com/coverage-savings | Apr 7, 2026 |
| CMS Bridge: Jul 1–Dec 31, 2026; KwikPen; $50 copay | cms.gov | Apr 7, 2026 |
| Ro Body: $45 first month, $145 ongoing | ro.co/weight-loss/pricing | Apr 7, 2026 |
What can change: Pricing, Savings Card terms, insurance formularies, CMS demonstration program details, and provider workflows all shift regularly. We check this page monthly and update the "Last verified" timestamp every time we re-confirm. Last verified: April 7, 2026.
FAQ: Switching From Semaglutide to Zepbound
Can you switch from semaglutide to Zepbound immediately?
Not the same day you take your last semaglutide dose. The common approach is to start Zepbound on your next scheduled injection day — typically about 7 days later. Your prescriber confirms the exact timing based on your situation.
How long should you wait after semaglutide before starting Zepbound?
About one week — your next regular injection day — is a common clinician-guided approach. You do not need a 4–5 week full washout despite what some pages claim. Semaglutide has a ~7-day half-life and declines gradually, providing a natural buffer.
What dose of Zepbound do you start with after semaglutide?
The labeled starting dose is 2.5 mg once weekly for 4 weeks, followed by 5 mg. Some prescribers start GLP-1–experienced patients at 5 mg. There is no official dose-equivalence chart between semaglutide and Zepbound.
Is there a semaglutide to Zepbound conversion chart?
No official milligram-for-milligram conversion chart exists between semaglutide and Zepbound. The medications work through different receptor mechanisms, making direct dose comparisons misleading. Unofficial charts found online are not validated by Lilly or the FDA.
Can you take semaglutide and Zepbound together?
No. Zepbound's prescribing information states it should not be used with another GLP-1 receptor agonist, including semaglutide products like Wegovy and Ozempic.
Is Zepbound more effective than semaglutide for weight loss?
On average, yes. The SURMOUNT-5 head-to-head trial showed approximately 20.2% body weight loss with Zepbound vs. 13.7% with Wegovy over 72 weeks. Individual results vary — some patients respond better to semaglutide.
How much does Zepbound cost without insurance in 2026?
Through LillyDirect self-pay: $299/month for 2.5 mg, $399/month for 5 mg, and $449/month for 7.5–15 mg (vials or KwikPen at higher doses). Retail pharmacy list price without discounts is approximately $1,086/month.
Can Medicare patients get Zepbound in 2026?
Traditional Medicare Part D generally does not cover Zepbound for weight loss. CMS has announced a GLP-1 Bridge demonstration program running July 1, 2026 through December 31, 2026, which includes Zepbound KwikPen for eligible beneficiaries.
If I'm on Ozempic for diabetes, should I ask about Mounjaro instead of Zepbound?
Potentially. Mounjaro (tirzepatide) is FDA-approved for type 2 diabetes, while Zepbound is approved for weight management. If diabetes is your primary indication, Mounjaro may be more appropriate and may have different insurance coverage. Your prescriber can advise.
What if I'm switching from compounded semaglutide?
The switching protocol — timing and starting dose — is the same. The difference is primarily on the access side: you'll need a prescriber to write a Zepbound Rx and you'll need to navigate insurance or self-pay from scratch.
Will I regain weight during the switch?
Significant regain is uncommon when the transition happens within the standard ~7-day window. Semaglutide's long half-life means it's still declining in your system as Zepbound takes effect. A prolonged gap between medications is the main risk — which is why the 'next injection day' approach is commonly recommended.
Can I switch back to semaglutide if Zepbound doesn't work for me?
Yes. The switch is reversible. If Zepbound's side effects are unmanageable or you prefer semaglutide for other reasons, your prescriber can transition you back using a similar approach — finishing one medication before starting the other.
Still weighing options?
Not Sure Which GLP-1 Program Is Right for You?
Take our free 60-second GLP-1 matching quiz. We'll ask about your current medication, insurance status, goals, and budget, then give you a personalized recommendation — not a generic list.
Get Your Personalized GLP-1 Action Plan →6 questions · 60 seconds · Free
Ready to start your switch?
Insurance concierge + prior auth support included
Another licensed telehealth provider for Zepbound
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
Related Guides
Published by The RX Index, an independent editorial publisher covering GLP-1 medications and telehealth providers.
Last verified: April 7, 2026
Sources: FDA prescribing information for Zepbound and Wegovy, SURMOUNT-5 (NEJM 2025), Rodriguez et al. (JAMA Internal Medicine 2024), Almandoz et al. (Clinical Diabetes 2020), Eli Lilly pricing pages, CMS.gov, Ro.co.
Related guides
- How to Switch From Semaglutide to Mounjaro (2026): Timing, Doses, Cost
- How to Switch from Semaglutide to Tirzepatide
- How to Switch From Compounded Semaglutide to Tirzepatide (2026)
- How to Get GLP-1 Without Insurance in 2026: Real Prices [Verified]
- Zepbound vs Wegovy for Weight Loss (2026): Real Prices + Verdict