PCOS & GLP-1 MEDICATIONS — 2026 GUIDE
Best GLP-1 for PCOS: Which Medication Actually Fits Your Symptoms, Budget & Timeline?
There is no single best GLP-1 for every woman with PCOS — but there is a best GLP-1 for your version of it. This guide breaks down exactly which medication fits which situation, what the clinical evidence actually shows, and how to access it affordably.
By The RX Index Research Team · Last updated: March 27, 2026 · Provider pricing last verified: March 27, 2026
Sources: 2023 International Evidence-Based PCOS Guidelines (Teede et al.); SURMOUNT-1 & SURMOUNT-5 (NEJM); FDA prescribing information; Truveta/Reuters (2025)
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
Bottom line
Semaglutide (Wegovy/Ozempic class) is the strongest first step for most women with PCOS — most PCOS-specific data, affordable access from $179/month, weekly injection. Tirzepatide (Mounjaro/Zepbound class) is the more powerful option when maximum weight loss matters most — it beat semaglutide in a 72-week head-to-head trial but costs more and has thinner PCOS-specific evidence. No GLP-1 is FDA-approved specifically for PCOS.
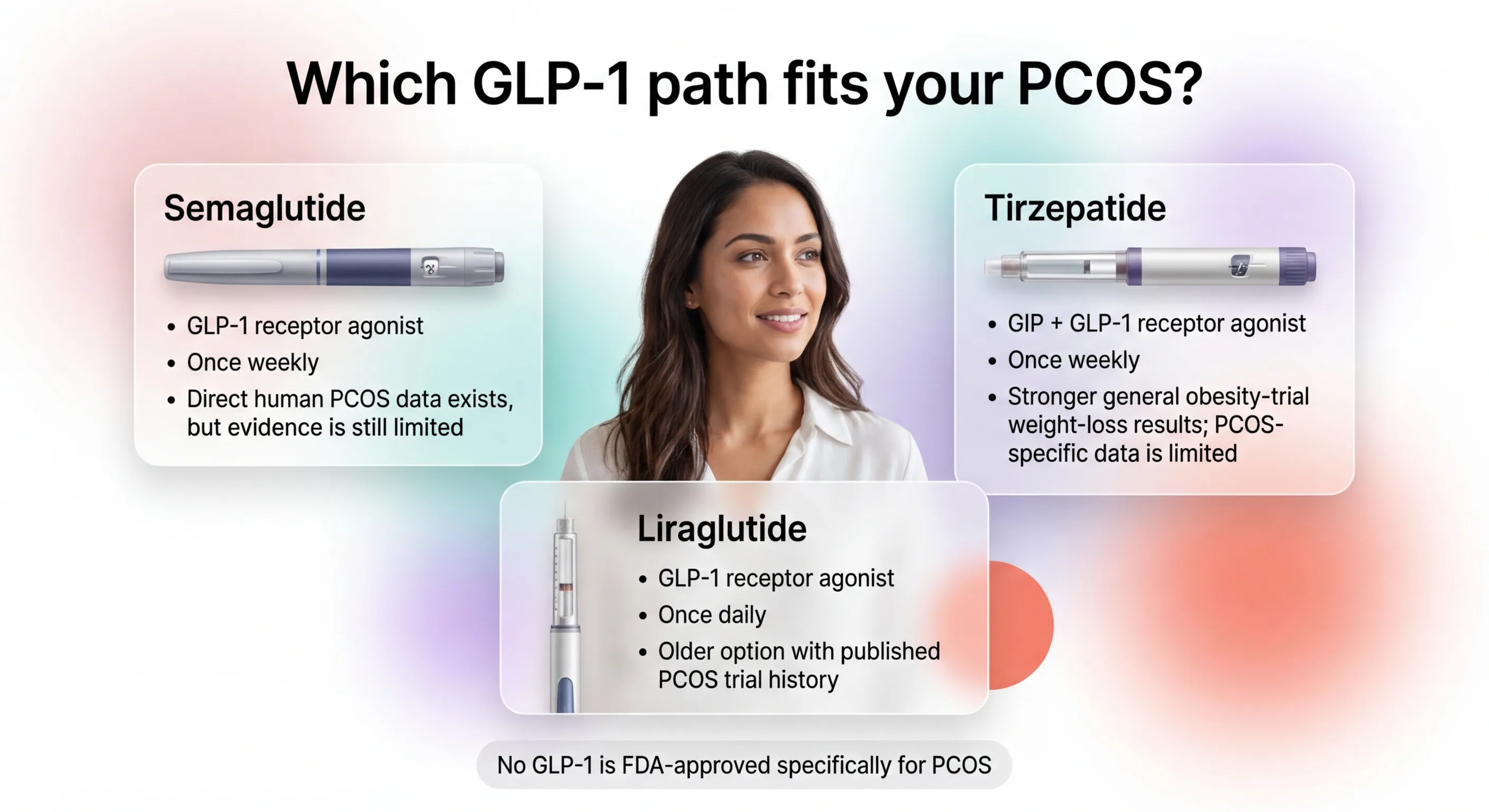
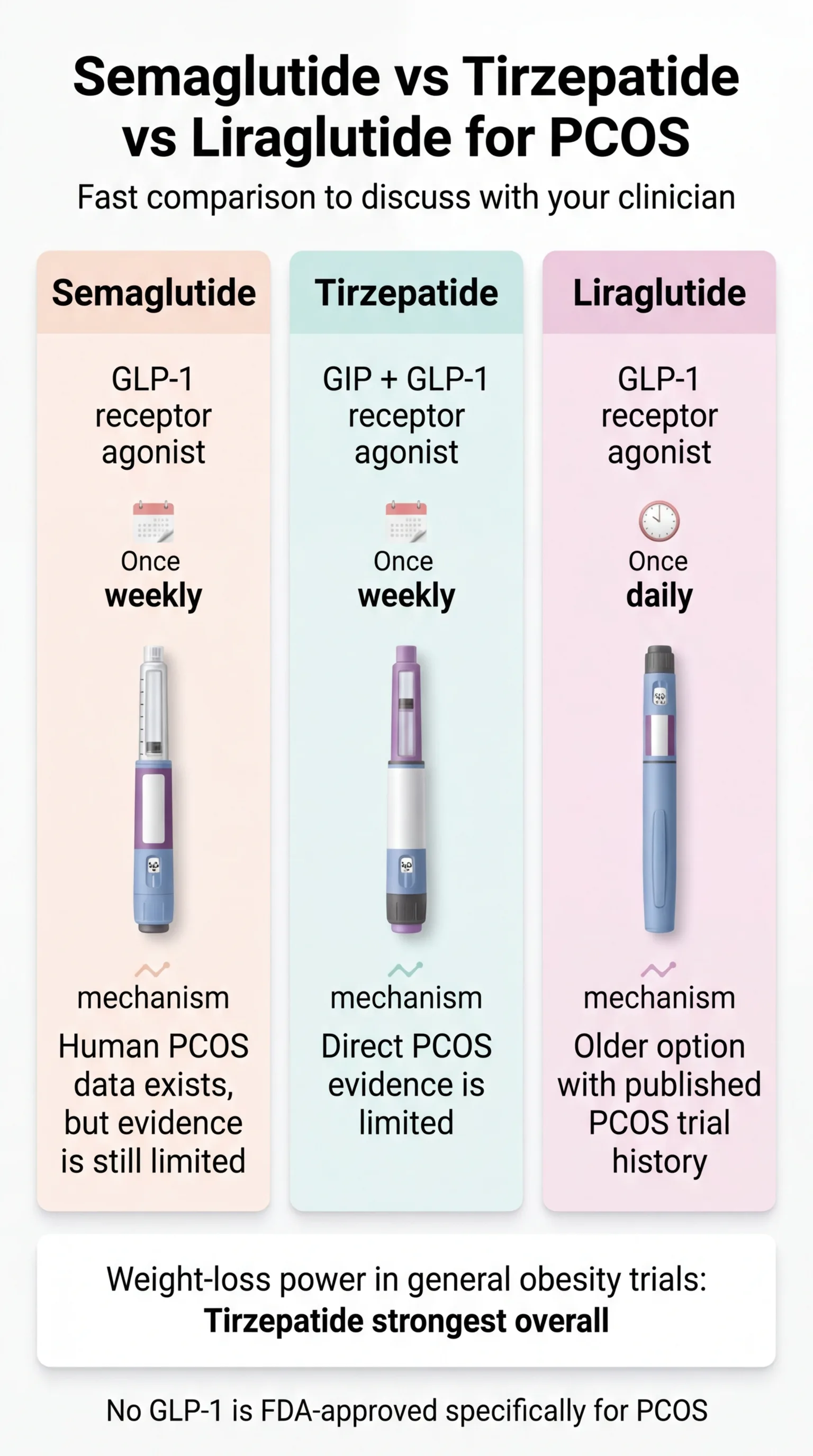
Semaglutide vs Tirzepatide vs Liraglutide for PCOS — Compared
Here's how the three GLP-1 options stack up for PCOS-specific outcomes — not general weight loss hype. PCOS outcomes.
| Semaglutide Wegovy / Ozempic | Tirzepatide Mounjaro / Zepbound | Liraglutide Saxenda / Victoza | |
|---|---|---|---|
| Best for | Most women with PCOS (strongest first step) | Severe insulin resistance / maximum weight loss | GLP-1 sensitive patients; can't tolerate semaglutide |
| How it works | GLP-1 receptor agonist | Dual GLP-1 + GIP agonist | GLP-1 receptor agonist |
| Direct PCOS evidence | Emerging — small PCOS studies + combination trial data | Limited — no PCOS-specific trials; Eli Lilly confirms no sponsored PCOS studies | Most direct PCOS trial history (multiple RCTs), older and less potent |
| Avg. weight loss | 12–17% of body weight at higher doses | 20–22.5% at higher doses (SURMOUNT-1, NEJM 2022) | 5–8% of body weight |
| Insulin resistance | Significant improvement in fasting insulin in PCOS studies | Strong general obesity improvement (no PCOS-specific data) | Moderate improvement |
| Effect on periods | Menstrual regularity restored in many patients | Expected based on metabolic improvement (limited PCOS data) | Some evidence of cycle improvement |
| Dosing | Weekly injection | Weekly injection | Daily injection |
| FDA-approved for | Type 2 diabetes (Ozempic); Obesity (Wegovy) | Type 2 diabetes (Mounjaro); Obesity (Zepbound) | Type 2 diabetes (Victoza); Obesity (Saxenda) |
| Affordable access | Yes — compounded from $179/mo (MEDVi); brand Wegovy pill from $149/mo (Ro) | From $299/mo for medication + Ro membership | Yes — compounded available |
| Biggest downside | GI side effects early on; weight regain after stopping | Higher cost; less PCOS-specific data | Significantly less weight loss than newer options |
Sources: SURMOUNT-1 (NEJM, 2022); SURMOUNT-5 (NEJM, 2025); 2023 International Evidence-Based PCOS Guidelines (Teede et al.); Truveta/Reuters (2025); FDA prescribing information. Weight-loss percentages from obesity populations — not PCOS-specific studies. Evidence distinction labeled throughout.
Which one sounds like you?
- Classic PCOS with weight gain + insulin resistance → Start with semaglutide. Most accessible, most affordable, growing PCOS-specific evidence.
- BMI 35+ with pre-diabetes or severe insulin resistance → Consider tirzepatide for the strongest metabolic push.
- Already tried semaglutide, couldn't tolerate GI side effects → Try liraglutide's gentler daily dosing.
- Trying to conceive within 6 months → Read the fertility section first. This probably isn't the right time to start.
- Not sure? → Take our free 60-second PCOS GLP-1 matching quiz.
Which GLP-1 Is Best for PCOS? (By Your Specific Situation)
The question isn't really "which GLP-1 is best." It's "which GLP-1 is best for my PCOS." Your situation changes the answer entirely.
Best GLP-1 for PCOS and Insulin Resistance
This is the most common scenario. Estimates range from 50% to 80% of women with PCOS having clinically significant insulin resistance. That insulin resistance drives a vicious cycle: excess insulin tells your ovaries to overproduce androgens (testosterone), those androgens promote abdominal fat storage, and that additional fat worsens insulin resistance further.
GLP-1 medications break into this cycle at multiple points simultaneously.
Our take: Semaglutide is the better first move for most women with PCOS-driven insulin resistance. It has direct PCOS human data — including small studies and a combination trial with metformin — showing improved fasting insulin, lower testosterone, and restored menstrual regularity. If your insulin resistance is severe (A1C 5.7–6.4%, fasting insulin consistently elevated, or pre-diabetic), tirzepatide's dual-action mechanism may justify the higher cost.
Either way, this isn't vanity. This is metabolic medicine for a metabolic disorder.
If you have PCOS with insulin resistance and a BMI of 27+, you may be eligible for a GLP-1 through telehealth.
Best GLP-1 for PCOS Weight Loss
If your primary goal is moving the scale, tirzepatide wins on raw weight-loss power. In the SURMOUNT-5 head-to-head trial (NEJM, 2025), tirzepatide outperformed semaglutide (~20% vs ~14% body weight loss). But semaglutide at higher doses still delivers 12–17% body weight reduction — for a 200-pound woman, that's 24–34 pounds. Research shows even 5% body weight loss can help balance hormones and regulate menstrual cycles in PCOS.
Our take: If cost isn't the primary constraint and you need to lose 60+ pounds, tirzepatide is the stronger option. For everyone else, semaglutide is the more practical path that still delivers meaningful results.
Ready to stop reading and start losing?
Best GLP-1 for PCOS If You're Already on Metformin
This isn't an either/or. A 2025 randomized trial (Zheng et al.) showed that semaglutide combined with metformin outperformed metformin alone on weight loss, insulin resistance, menstrual cyclicity, and even pregnancy rates in women with PCOS-related infertility. The low hypoglycemia risk makes the combination safe.
Our take: If metformin alone isn't moving the needle, adding a GLP-1 is the evidence-based next step — not replacing everything, just augmenting what you already have.
Best GLP-1 for PCOS If Lower Cost Matters Most
Brand-name Wegovy or Zepbound without insurance runs $900–$1,100+ per month. The practical path for cash-pay patients is compounded semaglutide through a telehealth provider — prepared by state-licensed pharmacies based on a valid prescription. The FDA does not review or approve compounded medications, which is an important distinction from FDA-approved brand-name products.
Starting prices range from $179/month all-in through MEDVi to $149/month for medication through Ro (plus membership fee). More on provider pricing in the pricing section.
Best GLP-1 for Lean PCOS
If you have PCOS without significant weight to lose, the evidence for GLP-1 use is thinner. Preclinical research suggests GLP-1 medications may work through additional mechanisms beyond weight loss — including reducing ovarian inflammation and lowering androgen levels directly — but this is not yet confirmed in large human trials.
Our take: If you have lean PCOS, work with an endocrinologist rather than going through telehealth. This is a clinician-first lane. The evidence isn't strong enough yet for us to confidently recommend a specific telehealth provider.
Best GLP-1 for PCOS If You Hate Injections
An oral semaglutide option now exists. Ro offers a Wegovy pill starting at $149/month for medication (plus the Ro membership). Eli Lilly's oral GLP-1 (orforglipron) is also expected to reach the market soon. MEDVi offers GLP-1 tablets starting at $249/month. The trade-off: oral GLP-1s may produce somewhat less dramatic weight loss than injectables.
If needles have been the thing stopping you, that barrier is gone.
You Haven't Failed — Your PCOS Metabolism Has Been Working Against You
If you've done the diets, the workouts, the metformin, the birth control pills — and the scale barely moves — you are not failing. Your metabolism is fighting you. PCOS-driven insulin resistance creates a self-reinforcing loop that diet and exercise alone often cannot break. This is not a character flaw. It's endocrinology.
As Dr. Melanie Cree, a pediatric endocrinologist at Children's Hospital Colorado who has studied GLP-1s in PCOS patients for over a decade, put it: "Primary therapies used for PCOS symptoms haven't changed in nearly 50 years." That's not because women with PCOS haven't tried hard enough. It's because the available tools weren't good enough.
GLP-1 medications target appetite, insulin sensitivity, and the metabolic dysfunction at the root of PCOS simultaneously — something previous treatment options couldn't do at this scale. The 2023 International PCOS Guidelines now state that GLP-1s like semaglutide and liraglutide could be considered for women with PCOS and higher weight alongside lifestyle changes. More than 90,000 women with PCOS received a GLP-1 prescription during a recent study period tracked by Truveta across more than 445,000 PCOS patients.
"I finally feel like a normal person when it comes to hunger and cravings."
Here's the honest part: GLP-1 medications are not a cure for PCOS. They manage it — effectively — but the benefits last as long as you're taking the medication. Research shows that when people stop, about two-thirds of the weight lost tends to return. That means you're looking at long-term treatment, not a quick fix.
But consider the reframe: if you had high blood pressure, you wouldn't call it "cheating" to take medication. PCOS is a chronic metabolic condition. The cost of not treating it — higher risk of type 2 diabetes, cardiovascular disease, endometrial cancer, and infertility — is far more expensive in the long run.
If you've been fighting PCOS weight for years and metformin hasn't been enough, checking your eligibility takes about 5 minutes.
What the Research Actually Shows About GLP-1s for PCOS
Not cherry-picked studies. Here's what the evidence actually looks like — including where it's solid, where it's thin, and where it's being actively studied.
How GLP-1s Actually Work on PCOS (Not Just Weight Loss)
This matters. GLP-1 medications aren't just "weight loss drugs" that happen to help PCOS. They target the metabolic machinery that drives PCOS symptoms.
Here's the cycle: insulin resistance → excess insulin → ovaries overproduce androgens (testosterone) → androgens promote abdominal fat storage → more fat worsens insulin resistance → repeat. This loop is why diet and exercise alone often can't break through for women with PCOS.
GLP-1 medications interrupt this cycle at multiple points simultaneously. They improve how your body responds to insulin. They reduce appetite through direct action on brain receptors. They slow gastric emptying. And they promote the kind of clinically significant weight loss (10%+ of body weight) that can meaningfully shift hormonal balance.
Preclinical research also suggests GLP-1 receptor agonists may have direct anti-inflammatory effects in ovarian tissue and may help lower androgen levels through mechanisms beyond weight loss alone. This is still being studied in humans — and it's one reason researchers are particularly excited about this drug class for PCOS.
The 2023 International PCOS Guidelines
The most authoritative guidance on PCOS treatment — the 2023 International Evidence-Based Guidelines (Teede et al.), endorsed by the American Society for Reproductive Medicine — states that GLP-1 receptor agonists such as liraglutide and semaglutide could be considered for adults with PCOS and higher weight, alongside lifestyle intervention. The guideline emphasizes effective contraception when pregnancy is possible, gradual dose escalation, and shared decision-making about side effects, potential long-term use, and high risk of weight regain after discontinuation.
The Direct PCOS Evidence
Semaglutide:
- An Italian pilot study treated 27 obese women with PCOS who hadn't responded to lifestyle changes with low-dose subcutaneous semaglutide for 3 months. Nearly 80% achieved at least 5% body weight loss (mean: ~17 pounds), with improved blood sugar and more regular menstrual cycles. Minimal adverse effects.
- A 2025 randomized trial (Zheng et al.) showed semaglutide plus metformin outperformed metformin alone for weight, insulin sensitivity, and menstrual cyclicity in overweight/obese women with PCOS-related infertility.
- Recent meta-analyses of GLP-1 receptor agonists in PCOS populations have found reductions in weight, BMI, fasting insulin, and testosterone — though overall certainty of evidence is rated low to moderate.
Tirzepatide:
- No PCOS-specific clinical trials have been published. Eli Lilly confirmed it has not sponsored clinical studies of tirzepatide specifically in PCOS, and no PCOS subgroup analyses were performed.
- However, the general obesity trial data is the strongest of any GLP-1. SURMOUNT-1 (NEJM, 2022) showed up to 22.5% body weight reduction at the highest dose. SURMOUNT-5 (NEJM, 2025) showed it beat semaglutide head-to-head.
Liraglutide:
- The earliest GLP-1 studied in PCOS populations, with multiple randomized controlled trials showing positive results for weight, insulin resistance, and hormonal markers.
- A meta-analysis of 8 randomized trials compared GLP-1 receptor agonists (primarily liraglutide) to metformin in women with PCOS, showing weight loss and testosterone reductions.
The 2026 Systematic Review
A 2026 systematic review published in the European Journal of Endocrinology analyzed 11 randomized controlled trials of GLP-1 receptor agonists for PCOS. It found modest short-term BMI reduction, but rated the overall certainty of evidence as low and noted insufficient evidence for several important outcomes.
What this means for you: The evidence is promising and growing rapidly, but it's not yet at the level of 20-year, large-scale definitive proof. You're not making a reckless choice — the 2023 guidelines support it — but you should understand the research community is still building the complete picture.
Evidence Confidence Summary
| Outcome | Evidence Level |
|---|---|
| Weight loss in women with PCOS | Moderate (semaglutide) / Strong general data (tirzepatide) |
| Insulin resistance improvement | Moderate |
| Menstrual regularity | Moderate (semaglutide/liraglutide) / Limited (tirzepatide) |
| Testosterone/androgen reduction | Moderate |
| Fertility improvement | Early/promising — not a fertility drug |
| Long-term PCOS outcomes | Insufficient data |
| Safety in pregnancy | Not established — must stop before TTC |
Semaglutide vs Tirzepatide for PCOS: The Full Breakdown
Weight Loss
Tirzepatide wins. The SURMOUNT-5 trial showed ~20% body weight reduction for tirzepatide vs ~14% for semaglutide over 72 weeks. At the highest doses in SURMOUNT-1, tirzepatide patients lost up to 22.5% of their body weight. For a 200-pound woman with PCOS, that's roughly 40–45 pounds on tirzepatide vs 28–34 pounds on semaglutide. Both are clinically significant. Tirzepatide just goes further.
Insulin Resistance
Both improve insulin sensitivity. Tirzepatide's dual GLP-1 + GIP mechanism may provide additional metabolic benefits, though these haven't been studied in PCOS populations specifically. Semaglutide has more published data in PCOS populations showing fasting insulin improvement and testosterone reduction.
Our take: For severe insulin resistance (pre-diabetic range), tirzepatide's dual mechanism and stronger overall metabolic data give it the edge. For moderate insulin resistance, semaglutide's direct PCOS data and lower cost make it the more practical starting point.
Periods, Ovulation, and Hormonal Balance
Semaglutide has direct evidence of restoring menstrual regularity and reducing androgens in women with PCOS. Multiple studies have documented these outcomes. Tirzepatide's effects on reproductive hormones in PCOS are expected based on metabolic improvement — but we don't have published PCOS-specific data confirming it yet.
Cost and Access
- Compounded semaglutide: From $179/month (MEDVi) — no membership fee
- Brand-name Wegovy pill through Ro: From $149/month for medication + Ro membership ($45 first month, $145/month after)
- Brand-name Zepbound through Ro: From $299/month for medication + Ro membership
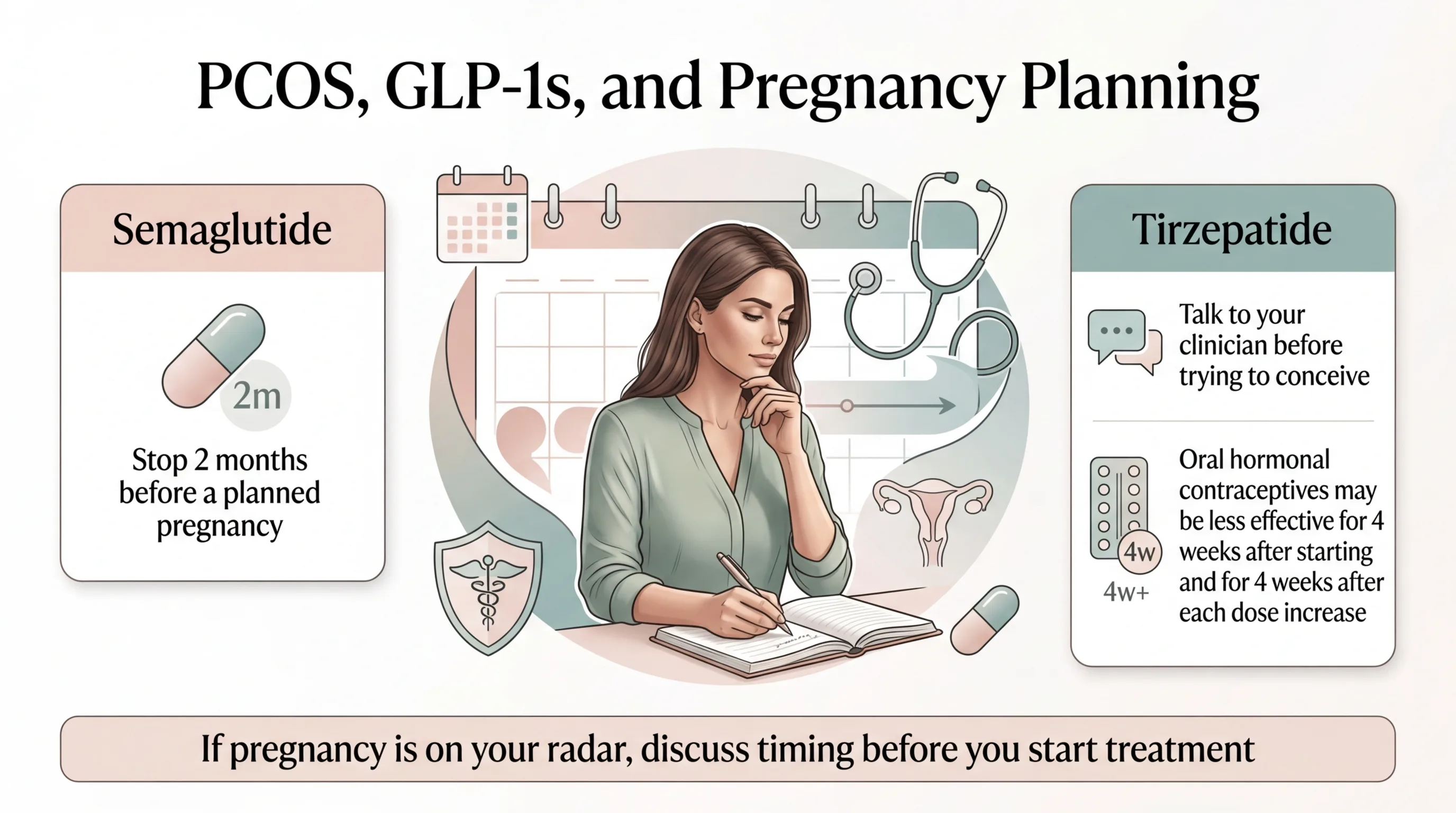
Pregnancy and Fertility Timing
- Semaglutide (Wegovy): FDA labeling advises stopping at least 2 months before a planned pregnancy.
- Tirzepatide (Zepbound): FDA labeling advises discontinuing when pregnancy is recognized. Also warns that oral hormonal contraceptives may be less effective for 4 weeks after starting tirzepatide and 4 weeks after each dose increase — use a non-oral backup method during those windows.
The Verdict
Start with semaglutide unless you have a specific reason to need tirzepatide's extra weight-loss power or more aggressive metabolic action. You can always switch later — and semaglutide gets you started at a lower cost with more PCOS-specific evidence backing you up.
Ready to see which option fits your situation?
GLP-1 vs Metformin for PCOS: Which Works Better?
Metformin has been the workhorse PCOS medication for over 20 years. It improves insulin sensitivity, is inexpensive (often $4–$15/month), has extensive long-term safety data, and is explicitly recommended in the 2023 PCOS Guidelines for women with BMI ≥ 25. The catch: metformin's impact on weight is modest — most women lose 2–5 pounds. For someone who needs to lose 30, 50, or 80 pounds to see real metabolic improvement, metformin alone often isn't enough.
GLP-1 medications deliver dramatically more weight loss (12–22% of body weight vs 1–3% for metformin) and appear to produce stronger improvements in insulin resistance, testosterone levels, and menstrual regularity. The 2025 combination study showed that semaglutide plus metformin was superior to metformin alone across nearly every measured outcome.
Practical takeaway:
- Haven't tried metformin yet: It's still a reasonable first step, especially if cost is a major barrier.
- On metformin and it's not enough: Adding a GLP-1 is the evidence-based next step. The combination is safe.
- Can't tolerate metformin: A GLP-1 is a legitimate alternative, not a last resort.
If metformin hasn't been enough on its own, you don't need to wait. A telehealth provider can evaluate whether adding a GLP-1 makes sense for your situation — and you can keep taking metformin alongside it.
Are GLP-1 Drugs Approved for PCOS?
No. No GLP-1 medication is FDA-approved specifically for the treatment of PCOS.
Wegovy (semaglutide) and Zepbound (tirzepatide) are FDA-approved for chronic weight management in adults with obesity (BMI ≥ 30) or overweight (BMI ≥ 27) with at least one weight-related condition. Ozempic and Mounjaro are FDA-approved for type 2 diabetes.
Here's the important nuance: if you have PCOS and meet the obesity/overweight criteria — which most women seeking GLP-1 treatment for PCOS do — a prescription for Wegovy or Zepbound can be written on-label for chronic weight management. What's off-label is prescribing specifically for the PCOS indication itself. This distinction matters for insurance coverage.
Off-label prescribing is legal, common in medicine, and in this case supported by the 2023 International PCOS Guidelines.
Novo Nordisk (maker of Ozempic/Wegovy) has no plans to pursue a PCOS-specific FDA indication. Eli Lilly (maker of Mounjaro/Zepbound) has not sponsored PCOS-specific studies. This means FDA approval for PCOS is unlikely in the near term — off-label prescribing will remain the primary path.
For a deeper breakdown of insurance strategies, see our full guide: How to Get Insurance to Cover GLP-1.
Branded vs Compounded GLP-1 for PCOS: What You Need to Know
This is where a lot of confusion and misinformation lives. Let's be clear about what each option actually is.
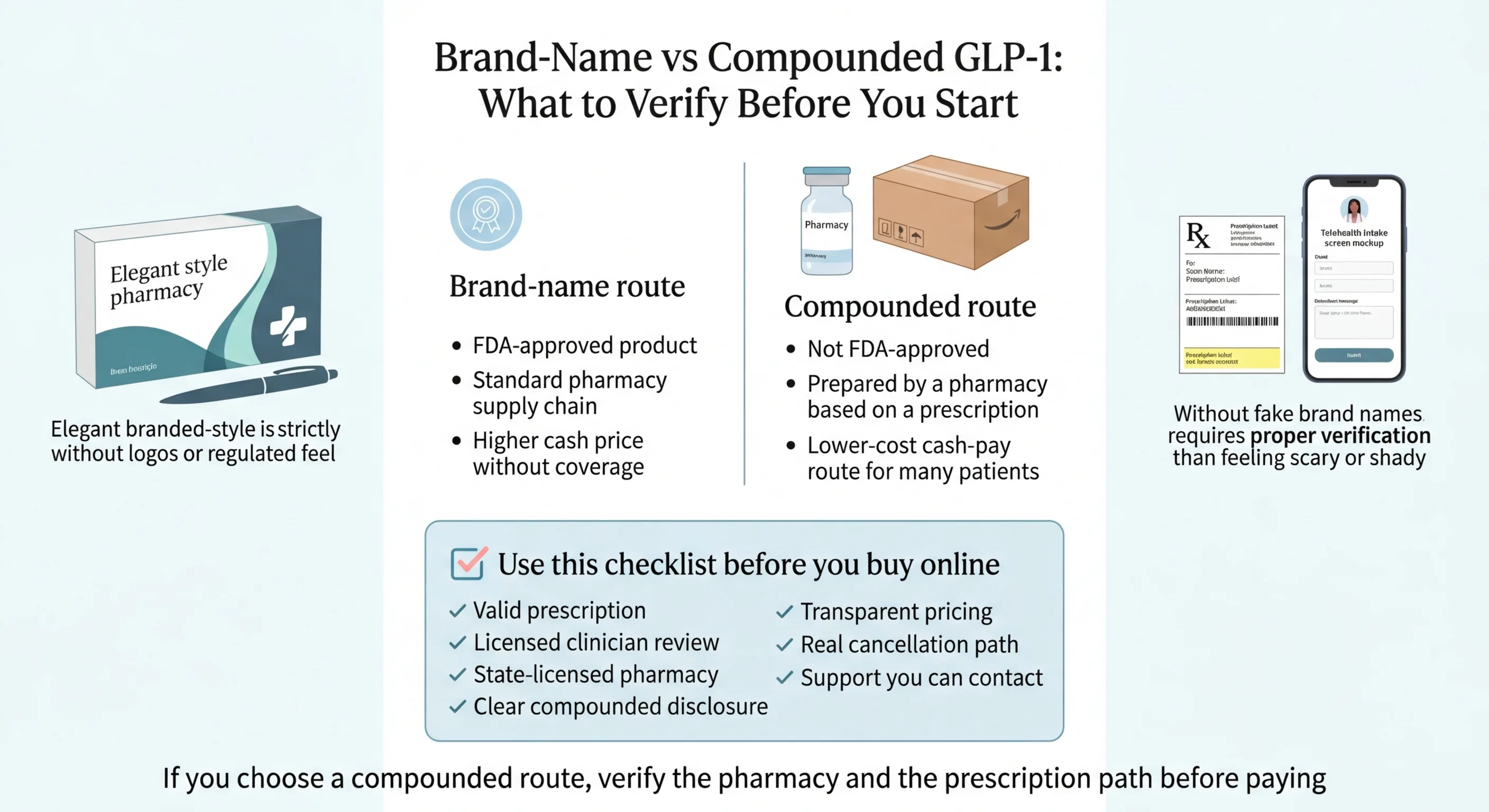
FDA-approved brand-name products (Wegovy, Ozempic, Zepbound, Mounjaro) are manufactured by pharmaceutical companies, reviewed and approved by the FDA for safety and effectiveness, and available through standard pharmacies. They are the gold standard. They are also expensive without insurance.
Compounded medications are prepared by state-licensed pharmacies based on a prescription from a licensed provider. The FDA does not review or approve compounded medications for safety or effectiveness. They are a common and growing access route for cash-pay patients — including many women with PCOS — who can't afford brand-name pricing.
If you go the compounded route, use this safety checklist:
- ✓A real prescription is required (not just a questionnaire)
- ✓The pharmacy is state-licensed and verifiable
- ✓The provider clearly discloses that the medication is compounded and not FDA-approved
- ✓Pricing is transparent with no hidden fees
- ✓There's a licensed clinician reviewing your health profile before prescribing
- ✓There's a clear cancellation path and customer support
How to Get GLP-1 for PCOS Online Safely
You know which medication you want. Now how do you actually get it — especially when insurance probably won't cover it for PCOS?
The Insurance Reality in 2026
Starting in 2026, several major insurers including Blue Cross Blue Shield, Cigna, and UnitedHealthcare have tightened GLP-1 coverage. Many plans now only cover these medications for type 2 diabetes, not weight management alone.
However: PCOS and obesity frequently co-occur. If you have a BMI ≥ 30 (or ≥ 27 with documented comorbidities like insulin resistance, hypertension, or high cholesterol), your provider can often code for the obesity indication rather than PCOS specifically. This is a legitimate coding pathway. Ro specifically includes insurance coverage navigation as part of their membership.
Strategy: Have your provider document your BMI, fasting insulin, A1C, and lipid panel. Apply for Wegovy or Zepbound under the obesity/overweight indication. If denied, appeal with the lab documentation. See our full guide: How to Appeal a GLP-1 Denial.
Provider Comparison for PCOS Patients
| Ro | MEDVi | |
|---|---|---|
| Best for | FDA-approved brand-name treatment; insurance navigation; women who want Wegovy or Zepbound | Cash-pay compounded semaglutide; lowest out-of-pocket starting cost |
| Medication type | FDA-approved (Wegovy pill, Wegovy pen, Zepbound, Ozempic) | Compounded semaglutide injections and tablets |
| Starting price | Medication from $149/mo (Wegovy pill intro) + $45 first month membership, $145/mo after | $179/mo all-in (no membership fee) |
| Insurance help | Yes — dedicated insurance concierge included | No — cash-pay only |
| Clinician review | Within ~2 business days | Included in the intake process |
| Membership/contracts | $45 first month, $145/mo ongoing (only charged if eligible) | No membership, no contract |
| Pharmacy | Brand-name FDA-approved pharmacies | State-licensed compounding pharmacies |
| Cancel anytime | Yes | Yes |
| State availability | All 50 states + D.C. (some program details vary by state) | Select states — confirm availability before starting |
Best FDA-Approved / Insurance Path — Ro
Ro is the strongest route for women who want FDA-approved GLP-1 treatment, who may have insurance that could cover it, or who simply want brand-name medication from a regulated supply chain. The Ro Body membership costs $45 for the first month and $145/month after that. Medication is billed separately.
What makes Ro stand out for PCOS patients specifically: their insurance concierge handles the paperwork and fights for coverage on your behalf.
The honest trade-off: Ro is not the cheapest path if you're paying entirely out of pocket. If rock-bottom monthly cost is your only priority and you're comfortable with compounded medication, MEDVi starts lower. But Ro gives you the best shot at insurance coverage — and if that works, it becomes the cheapest path by far.
"I was thrilled to not have to fight for my coverage." — Hannah, Ro member
Best Lower-Cost Compounded Cash-Pay Path — MEDVi
MEDVi is the strongest route for women who know they're paying cash, want no membership fees, and are comfortable with compounded medication. Compounded semaglutide injections start at $179/month. Tablets start at $249/month. No membership fee. No contract. Price includes physician review, treatment plan, and shipped medication. Over 500,000 patients have used MEDVi according to their site.
The honest trade-off: MEDVi does not offer FDA-approved brand-name medication or insurance billing. If your priority is brand-name treatment or getting insurance to cover the cost, Ro is the better path. But if you're paying cash and want the simplest, lowest-cost starting point for compounded semaglutide, MEDVi removes the friction.
"Very easy and convenient for a very busy working lady." — MEDVi patient
Other Ways to Reduce Cost
- HSA / FSA: GLP-1 prescriptions qualify as eligible medical expenses. MEDVi specifically notes HSA/FSA approval.
- Manufacturer savings: Novo Nordisk and Eli Lilly offer patient assistance programs for brand-name products.
- Medicare: Standard Medicare generally does not cover GLP-1s prescribed only for weight loss. A Medicare GLP-1 Bridge program is scheduled to begin July 1, 2026 — check current status before relying on Medicare coverage.
- Employer benefits: Some employers are adding GLP-1 coverage. Ask your HR team.
What Does GLP-1 Cost for PCOS Without Insurance?
Real numbers. No asterisks. Pricing verified March 27, 2026.
| Route | Starting Monthly Cost | What's Included | Notes |
|---|---|---|---|
| Ro — Wegovy pill (cash pay) | ~$149/mo med + $45–$145/mo membership | Insurance concierge, clinician, medication | Intro pricing; higher doses cost more |
| Ro — Wegovy pen (cash pay) | ~$199/mo med + $45–$145/mo membership | Insurance concierge, clinician, medication | Intro pricing; higher doses cost more |
| Ro — Zepbound (cash pay) | ~$299/mo med + $45–$145/mo membership | Insurance concierge, clinician, medication | Tirzepatide; intro pricing |
| MEDVi — Compounded injections | $179/mo all-in | Physician review, medication, shipping | No membership fee; refills $299 |
| MEDVi — Compounded tablets | $249/mo all-in | Physician review, medication, shipping | No membership fee |
| Brand-name without insurance or savings | $900–$1,100+/mo | Medication only; no provider support | Not recommended as a cash-pay path |
Watch out for:
- Intro price vs. ongoing refill price (always check)
- Membership fees billed separately from medication
- Lab requirements that add cost
- Shipping fees
- Cancellation friction — both Ro and MEDVi allow cancellation
Can GLP-1 Help With PCOS Fertility, Ovulation, or Periods?
This is one of the most emotionally loaded questions on this page. Let's handle it carefully.
The Promising Part
GLP-1 medications can improve fertility indirectly — and there's growing evidence for it. By improving insulin resistance, reducing weight, and lowering androgen levels, GLP-1s can help restore menstrual regularity and ovulation. Multiple studies have documented improved cycle regularity in women with PCOS taking semaglutide or liraglutide.
A 2025 randomized trial showed that semaglutide combined with metformin improved menstrual cyclicity and pregnancy rates compared to metformin alone in women with PCOS-related infertility.
Women on GLP-1s have reported surprise pregnancies — including some who were on birth control. This is likely related to improved ovulation from metabolic improvement, combined with the fact that GLP-1s slow gastric emptying, which may affect how oral medications (including birth control pills) are absorbed.
The Critical Safety Rules
GLP-1 medications are not proven safe during pregnancy. There are no sufficient human studies confirming safety during conception or pregnancy. The rules differ by medication:
- Semaglutide (Wegovy): FDA labeling advises stopping at least 2 months before a planned pregnancy.
- Tirzepatide (Zepbound): FDA labeling advises discontinuing when pregnancy is recognized. The Zepbound label warns that oral hormonal contraceptives may be less effective for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase — use a non-oral backup contraceptive method during those periods.
- Conservative recommendation: Many reproductive endocrinologists suggest a 2–3 month washout period before trying to conceive, regardless of which GLP-1 you're on.
What This Means for Your Timeline
- Planning pregnancy within 6 months: Talk to your reproductive endocrinologist before starting a GLP-1. The timing matters.
- 12+ months from trying to conceive: Starting a GLP-1 now to optimize your metabolic health could actually improve your fertility outcomes when you're ready. Use effective contraception — and if you're on tirzepatide, use a non-oral backup method during the first 4 weeks and after each dose increase.
- Not planning pregnancy: Use contraception while on GLP-1 treatment. The improved ovulation means pregnancy risk increases, even if you've had irregular cycles for years.
GLP-1 medications are not fertility drugs. They don't replace clomiphene, letrozole, or IVF. But they may be the best metabolic preparation tool for PCOS patients approaching fertility treatment.
What to Realistically Expect: GLP-1 Results for PCOS at 3, 6, and 12 Months
Setting expectations correctly is the difference between sticking with treatment and quitting during the hard early weeks.
Month 1–2: The Adjustment Phase
Your appetite drops noticeably. The "food noise" — that constant background hum of thinking about what to eat next — starts to quiet. This is the change women with PCOS describe as the most dramatic.
Weight loss is modest during titration: typically 2–5 pounds. GI side effects (nausea, bloating) are at their worst but usually manageable. Don't panic if the scale doesn't move much yet — the medication is building in your system.
Month 3–4: The Acceleration Point
Weight loss accelerates to meaningful levels — many women are down 5–10% of their starting body weight. Blood sugar is stabilizing. Energy is improving.
Some women report their period returning or becoming more regular for the first time in months or years. The Italian PCOS pilot study documented mean weight loss of approximately 17 pounds after just 3 months of low-dose semaglutide, with nearly 80% of participants achieving at least 5% body weight loss.
Month 6: The Metabolic Shift
Average weight reduction of 10–15% of starting body weight on semaglutide; potentially higher on tirzepatide. Fasting insulin levels measurably improved. Testosterone may be notably lower on lab work. Menstrual regularity is often well established.
Many women describe this as the point where PCOS stops running their life.
Month 12+: The New Baseline
Maximum weight loss is typically achieved between 12–18 months. Continued use is generally recommended for sustained results — but some women transition to a lower maintenance dose or augment with metformin and lifestyle modifications.
Picture yourself 6 months from now with stable blood sugar, regular cycles, and 25+ fewer pounds of metabolic burden. The eligibility check takes 5 minutes.
GLP-1 Side Effects With PCOS: Honest, Not Scary
Most women tolerate GLP-1s well, especially with gradual dose titration. But you should know what to expect.
Common Side Effects (>10% of users)
Nausea, diarrhea, constipation. These are the big three. Most intense during the first few weeks and during dose increases. Standard mitigation: start at the lowest dose, don't rush to increase, eat small meals, avoid high-fat foods, stay hydrated. Most women report these improve significantly within the first month.
Less Common (1–10% of users)
Vomiting, abdominal pain, headache, fatigue, injection site reactions (redness, itching).
Rare but Serious
Pancreatitis, gallbladder problems, thyroid tumors (seen in animal studies; FDA includes a boxed warning about medullary thyroid carcinoma risk). Report severe abdominal pain immediately.
PCOS-Specific Considerations
- Hair thinning: Some women report hair shedding on GLP-1s. This is typically telogen effluvium caused by rapid weight loss, not the medication itself. It's usually temporary. Since PCOS already causes hair concerns, this can feel alarming — but it's generally a separate issue.
- Disordered eating risk: GLP-1s suppress appetite significantly. For women with PCOS who have a history of disordered eating — which is more common in this population than most people realize — the appetite suppression can mask or interact with existing patterns. Discuss openly with your provider before starting.
- Malnutrition: When appetite drops, so does food intake. Protein deficiency is a real concern. Working with a provider who monitors your nutrition is important.
- Muscle loss: A portion of weight lost on GLP-1s is lean mass. Prioritize protein intake (aim for 0.7–1.0g per pound of goal body weight) and resistance training to preserve muscle.
What Happens If You Stop Taking a GLP-1 With PCOS?
The honest answer: you'll likely regain most of the results.
A 2022 study of semaglutide showed that when participants stopped treatment, they regained about two-thirds of their prior weight loss. Blood pressure returned to baseline. Lipid levels worsened. For PCOS specifically, this likely means weight regain, return of insulin resistance, potential return of irregular cycles, and possible return of increased androgen symptoms (acne, hair growth, etc.).
The reframe: Many chronic conditions require ongoing medication. Nobody questions whether someone with hypothyroidism should stay on levothyroxine. PCOS is a lifelong metabolic condition, and treating it with ongoing medication is a reasonable, evidence-based approach. Some women eventually step down to a lower maintenance dose. Others use GLP-1s to achieve a target weight and then transition to metformin plus lifestyle modifications for maintenance.
The longer you wait to address PCOS-driven insulin resistance, the harder the cycle becomes to break.
Who Should NOT Use a GLP-1 for PCOS Right Now
Not everyone should start a GLP-1. If any of these apply to you, talk to your doctor first — or consider a different path:
- You're pregnant or actively trying to conceive. Wegovy labeling advises stopping at least 2 months before planned pregnancy; Zepbound advises discontinuing when pregnancy is recognized. See the fertility section.
- Personal or family history of medullary thyroid cancer (MTC) or MEN2 syndrome. This is a contraindication on the FDA label.
- History of pancreatitis. GLP-1s may increase risk.
- Severe gastroparesis. GLP-1s slow gastric emptying further.
- Active eating disorder. The appetite suppression effects require careful clinical management in this context.
- Lean PCOS with no clear metabolic indication. The evidence is thinner here. See an endocrinologist.
If any of these describe you, you're not out of options. Metformin, inositol (particularly the 40:1 myo-inositol to D-chiro-inositol ratio), berberine, and lifestyle modifications all have evidence for PCOS management.
If none of the above apply to you — and you have PCOS with insulin resistance or a BMI of 27+ — you're a reasonable candidate to discuss GLP-1 treatment with a provider.
Questions to Ask Your Doctor About GLP-1 for PCOS
Whether you're going through telehealth or seeing an endocrinologist in person, walking in prepared makes the conversation more productive. Save or screenshot this list.
Before starting:
- Based on my labs (insulin, A1C, lipids, testosterone), am I a good candidate for a GLP-1?
- Would you recommend semaglutide or tirzepatide for my specific PCOS presentation?
- Should I continue metformin alongside the GLP-1, or switch?
- What's the right starting dose and titration schedule for me?
- How will we monitor my progress — which labs, how often?
About access and cost:
- Can you code this under obesity or insulin resistance rather than PCOS for insurance purposes?
- If insurance denies coverage, will you help with the appeal?
- Are you comfortable prescribing compounded semaglutide if brand-name isn't financially feasible?
About fertility (if relevant):
- Given my fertility timeline, when should I stop the GLP-1 before trying to conceive?
- What contraception do you recommend while I'm on this medication?
About monitoring:
- How will you track whether the GLP-1 is actually improving my PCOS markers (not just weight)?
- What should I do about protein intake and nutrition while my appetite is suppressed?
- At what point would we consider changing the dose or switching medications?
How We Compared These GLP-1 Options
Medication comparison: Based on peer-reviewed clinical trials (cited throughout), the 2023 International Evidence-Based PCOS Guidelines, FDA prescribing information, and Truveta/Reuters real-world data analyzing over 445,000 PCOS patients. We label the evidence confidence level for each claim.
Provider comparison: Pricing verified directly from Ro and MEDVi websites on March 27, 2026. We verify pricing monthly and update the "last verified" date when we do.
Affiliate disclosure: This page contains affiliate links to Ro and MEDVi. If you click and sign up, we may receive a commission. This is how we fund the research. It does not influence our rankings, our recommendations, or the evidence we present.
What we are not: We are not doctors. This is research journalism, not medical advice. Every decision about GLP-1 treatment should be made with your healthcare provider based on your individual health profile.
Frequently Asked Questions: GLP-1 for PCOS
Which GLP-1 is best for PCOS and insulin resistance?
Semaglutide is the strongest practical first step — it has emerging PCOS-specific data showing improved fasting insulin, lower testosterone, and cycle regularity, plus the broadest affordable access routes. Tirzepatide may deliver stronger metabolic results based on its dual mechanism and superior general obesity data, but it has no published PCOS-specific trial data and costs more. Liraglutide has the longest PCOS trial history but produces less weight loss than either newer option.
Are GLP-1 drugs FDA-approved for PCOS?
No GLP-1 is FDA-approved specifically for PCOS. However, Wegovy and Zepbound are FDA-approved for chronic weight management in adults who meet the obesity/overweight criteria — which most women with PCOS seeking GLP-1 treatment do. The PCOS indication itself remains off-label. The 2023 International PCOS Guidelines state that GLP-1s could be considered for women with PCOS and higher weight.
Semaglutide or tirzepatide for PCOS?
For most women: start with semaglutide. More PCOS-specific data, broader access, lower cost. Consider tirzepatide if you need maximum weight loss (60+ lbs) or have severe insulin resistance that hasn't responded to semaglutide.
Can I take a GLP-1 and metformin together for PCOS?
Yes. The combination is safe and may be more effective than either alone. A 2025 study showed semaglutide plus metformin outperformed metformin alone for weight, insulin resistance, and menstrual cyclicity in PCOS patients. Low hypoglycemia risk with the combination.
What does GLP-1 cost for PCOS without insurance?
Compounded semaglutide starts at $179/month all-in through MEDVi (no membership fee). Brand-name Wegovy pill through Ro starts at $149/month for medication plus a separate Ro membership ($45 first month, $145/month after). Brand-name without any savings or insurance runs $900–$1,100+/month. HSA and FSA funds can be used toward either route.
Does insurance cover GLP-1 for PCOS?
Rarely for PCOS specifically. However, if you meet obesity criteria (BMI ≥ 30 or ≥ 27 with comorbidities), your provider may be able to code for that indication instead. Ro includes insurance navigation as part of their membership.
Can GLP-1 help with PCOS fertility?
Indirectly, yes. By improving insulin resistance, reducing weight, and lowering androgens, GLP-1s can restore ovulation and menstrual regularity. But they are not fertility drugs. Wegovy's label advises stopping at least 2 months before planned pregnancy; Zepbound's label advises discontinuing when pregnancy is recognized. Use effective contraception while on treatment — and if you're on tirzepatide, use a non-oral backup method during the first 4 weeks and after dose increases.
Are compounded GLP-1 programs legitimate?
Legitimate ones are. Look for: a real prescription requirement, a state-licensed pharmacy, clear disclosure that the medication is compounded and not FDA-approved, transparent pricing, and a licensed clinician review. The FDA advises caution and recommends only using compounded medications from state-licensed pharmacies with a valid prescription.
What happens if I stop taking a GLP-1 with PCOS?
Research shows about two-thirds of weight lost tends to return after discontinuation. Metabolic improvements also tend to reverse. Most experts recommend viewing GLP-1 treatment for PCOS as long-term, similar to other chronic condition medications.
Is there an oral GLP-1 option for PCOS?
Yes. Ro offers a Wegovy pill (oral semaglutide) starting at $149/month for medication, plus the Ro membership fee ($45 first month, $145/month after). MEDVi offers GLP-1 tablets starting at $249/month all-in. Oral options may produce somewhat less dramatic weight loss than injectables but remove the injection barrier entirely.
Does GLP-1 help with PCOS acne, hair loss, or excess hair growth?
Indirectly — by lowering testosterone through improved insulin resistance and weight loss, some women see improvement in androgen-driven symptoms like acne, hirsutism, and scalp hair thinning. This isn't a guaranteed outcome and depends on how much of your symptom burden is androgen-driven vs. other factors.
Still Not Sure Which GLP-1 Program Is Right for Your PCOS?
Every woman's PCOS is different — different phenotype, severity of insulin resistance, budget, fertility timeline, comfort level with injections vs oral, and insurance situation. You've read the evidence. You've seen the pricing. The only thing left is matching the right option to your situation.
That's why we built a free matching quiz. Five questions about your PCOS, your goals, and your constraints — and it recommends the GLP-1 option and access route that fits you best.
Or if you've already decided:
Sources
2023 International Evidence-Based PCOS Guidelines (Teede et al.), endorsed by the American Society for Reproductive Medicine · SURMOUNT-1 (NEJM, 2022) · SURMOUNT-5 (NEJM, 2025) · Zheng et al. (2025) semaglutide + metformin RCT · 2026 systematic review, European Journal of Endocrinology · FDA prescribing information for Wegovy, Zepbound, Saxenda · Truveta/Reuters PCOS prescribing data (2025) · Provider pricing verified from Ro and MEDVi directly, March 27, 2026.
This page was researched and written by The RX Index Research Team. This is research journalism, not medical advice. Last updated: March 27, 2026.