Insurance Appeals · April 22, 2026
How to Appeal a GLP-1 Insurance Denial (2026): Exact Steps + Real Cases
By The RX Index editorial team — Last verified: April 22, 2026. Next scheduled refresh: May 22, 2026.
The short answer: Most GLP-1 insurance denials fall into one of four buckets, and the bucket decides whether this is winnable. If your denial is a paperwork problem, a prior-authorization criteria mismatch, a reauthorization fight, or the wrong indication on file, you have a real chance of overturning it. If it’s a true plan exclusion for weight-loss drugs, a standard appeal usually won’t work — you need a different play.
The wording on your denial letter decides which fix to run. Match it to the decoder below and you’re already ahead of the vast majority of patients who never file any appeal.
What we actually verified for this guide (primary sources, April 22, 2026)
- Federal appeal rights and timelines — HealthCare.gov internal appeals and external review
- Medicare Part D redetermination timing — CMS Part D Redetermination page
- Medicare GLP-1 Bridge eligibility, drugs, and timeframe — CMS Medicare GLP-1 Bridge page (CMS last modified March 10, 2026)
- Three real GLP-1 external review decisions read in full — NY DFS #202303-160505, NY DFS #202209-153866, and Michigan DIFS File 236103-001
- KFF appeal-rate data — KFF ACA Marketplace claims denials analysis
- Ro pricing, drug list, and insurance concierge scope — verified against Ro’s public pricing and coverage pages
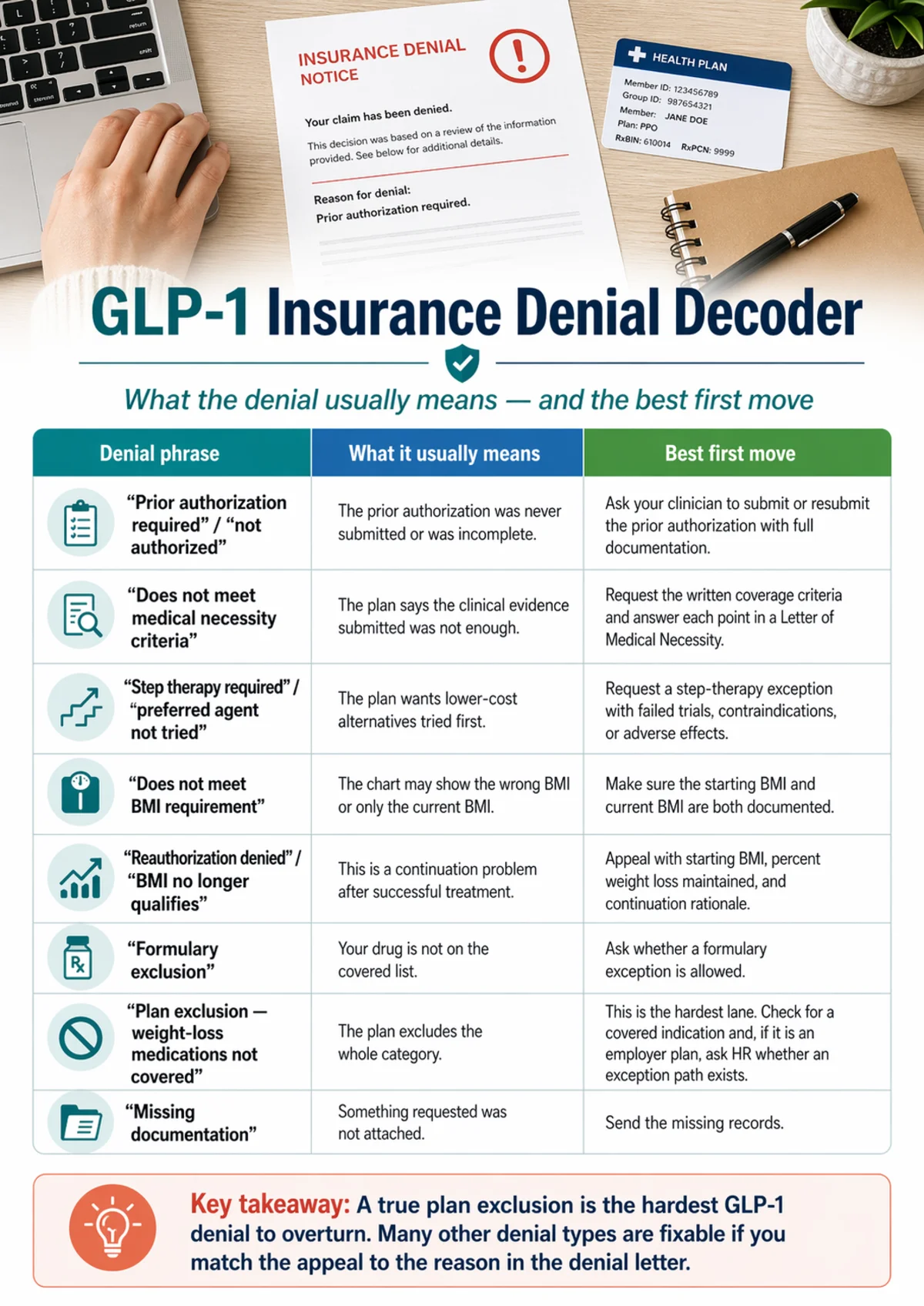
The GLP-1 Denial Decoder
Before you touch a keyboard, find the phrase on your denial letter in the left column. Your fix strategy lives on that row. Filing the wrong kind of appeal is one of the fastest ways to burn your refill window.
| Phrase on denial letter | What it really means | Winnable? | First move |
|---|---|---|---|
| “Prior authorization required” / “not authorized” | PA was never submitted or was incomplete | Very high | Get your clinician to submit (or resubmit) the PA with full documentation |
| “Does not meet medical necessity criteria” | Plan couldn’t see enough clinical evidence | High, with the right packet | Request the plan’s written medical policy, then write a Letter of Medical Necessity that answers each criterion point-by-point |
| “Step therapy required” / “preferred agent not tried” | Plan wants lower-cost alternatives documented first | High | File a step-therapy exception citing failures, contraindications, or adverse effects on the required drugs |
| “Does not meet BMI requirement” | Chart may show the wrong BMI or only current BMI | High if BMI data is wrong or incomplete | Confirm your starting BMI is documented, not just current; have clinician update chart and resubmit |
| “Reauthorization denied” / “BMI no longer qualifies” | Continuation problem after successful treatment | Winnable with the right framing | Appeal with starting BMI, percent weight loss maintained, and obesity-as-chronic-disease logic (see Cases 1 and 2 below) |
| “Formulary exclusion” | Your specific drug isn’t on the plan’s covered list | Moderate | Request a formulary exception with a clinical reason the listed alternative is inadequate |
| “Plan exclusion — weight-loss medications not covered” | Contract excludes the whole category | Low for standard appeal | Check for a covered indication first (T2D, established CVD, OSA). If employer plan, ask HR about an exception path. See the exclusion section below. |
| “Off-label use” | Drug prescribed outside FDA-approved indication | Winnable only if a covered indication applies | Re-prescribe under the correct indication if clinically appropriate |
| “Missing documentation” | Something the plan requested wasn’t attached | Very high | Send what’s missing. Often not a real denial at all. |
The phrase on your denial letter picks your lane. Coverage and appeal rights depend on your specific plan.
The only row to pump the brakes on is “plan exclusion.” A true exclusion is the hardest denial to beat with a standard appeal. Save your energy for the three paths that still work — we cover them in the plan exclusion section below.
Not sure which bucket you’re in?
Take the free 60-second GLP-1 path quiz →Before you spend a week writing an appeal, call your plan and request the specific medical policy number and criteria applied to your denial in writing. Your rights, the deadline clock, and the fix all flow from that document.
Why we built this guide this way
Formal appeal rates on denied Marketplace claims ran below 1% in 2024, and insurers upheld the denial 66% of the time when patients did appeal. That looks grim. But the same KFF data shows why. Most appeals fail on process problems — wrong category, missed deadlines, generic letters, missing evidence.
We pulled real publicly available external-review rulings to show you the patterns that change outcomes. No made-up success rates. No “80% of appeals succeed” folklore. Just what actually moved real independent reviewers. Whether this is worth your time depends almost entirely on which denial bucket you’re in.
What should you do in the first 24 hours?
The first day is about gathering evidence — not writing essays. You need the denial letter, the exact reason the plan used, the written coverage criteria it applied, and your deadline clock. Don’t start drafting an appeal until you have all four.
The 6-item day-one checklist
Save the denial letter
Paper, PDF, or portal screenshot — all of it. This is your clock-starting document and the first item in your appeal packet.
Write down the date you received it
This starts your appeal clock. The deadline in the letter controls, not the date the insurer issued the denial.
Call the insurer and request the written medical policy
Under federal rule (45 CFR 147.136), the denial notice must describe the standard used and how to request the underlying rules. The plan must provide relevant claim documents free of charge on request.
Pull your Summary Plan Description (SPD) or Evidence of Coverage (EOC)
Commercial and employer plans hide the rules that govern your appeal in here. Request it from HR or your benefits portal.
Ask your prescribing clinician for your records
Starting BMI, current BMI, comorbidity diagnoses with ICD-10 codes, and a list of prior weight-management interventions with dates and outcomes.
Note whether you're currently on the medication
If you're mid-course on a GLP-1 and getting cut off, a clinician statement certifying that delay could seriously jeopardize health may support an expedited review — 72-hour response instead of the standard clock.
The phone-call script
Use this verbatim when you call your insurer
“I’m calling about denial [reference number]. I need three things in writing: the specific medical policy applied to this denial, the criteria I didn’t meet, and the deadline to file an internal appeal. Federal rule requires the plan to provide claim documents on request. Can you email or fax them today?”
The person answering the phone isn’t the medical reviewer. Get what you need and move on.
How to appeal a GLP-1 insurance denial in 7 steps
A GLP-1 insurance appeal is won or lost in the packet, not the phone calls. The right sequence: read the denial verbatim, get the written criteria, fix factual errors, build evidence around the plan’s stated reason, file the correct appeal type for your plan, track every deadline, and escalate correctly if the first appeal fails.
Read the denial reason word-for-word.
"Not medically necessary" and "step therapy not met" are not the same problem. The phrase on the letter picks your lane.
Get the written coverage criteria.
Without the plan's own stated criteria in front of you, you can't write a rebuttal that actually answers them.
Fix factual errors first.
Often the denial is based on something simple — wrong BMI in the chart, wrong diagnosis code, missing A1C, PA submitted under obesity when the patient has documented T2D. If the error is fixable in five minutes, do that before filing a formal appeal.
Build the packet around the stated denial reason.
Quote the denial language at the top of your appeal letter. Then walk through the plan's criteria and show, with objective records, why each one is met. Appeals that mirror the plan's own language hit harder than generic ones.
File the right appeal for your plan type.
Commercial and ACA plans run internal → external review. Medicare Part D runs redetermination → IRE reconsideration → ALJ hearing. Medicaid runs a fair hearing. Self-funded employer plans are ERISA. The wrong filing goes nowhere.
Track every deadline and confirm receipt.
Certified mail or portal submission with a timestamp. Missing the deadline forfeits your rights.
If the first appeal loses, escalate to the next level.
A first loss is not the end. External review overturns a meaningful share of denials that reach it, and the process is free or under $25 on most ACA-compliant plans.
What goes in a strong GLP-1 appeal packet?
A strong packet takes the insurer’s stated reason and rebuts it point-by-point with objective evidence. A weak packet describes how the patient feels. A strong packet answers the plan’s criteria with numbers, dates, ICD-10 codes, and guideline citations.
The appeal packet checklist
| Item | Why it matters | Who provides it |
|---|---|---|
| Patient appeal cover letter | Frames the appeal, lists attachments, names the deadline | You |
| Letter of Medical Necessity (LMN) | The core clinical argument — the highest-leverage document in the packet | Your prescribing clinician |
| Denial letter(s) | Documents what you're appealing | You (keep the original) |
| Plan's written medical policy | What the appeal is measured against | Insurer (on request) |
| BMI history with dates | Objective eligibility evidence — starting AND current BMI both required | Clinician / chart |
| Comorbidity diagnoses with ICD-10 codes | Supports medical necessity | Clinician |
| Prior failed therapies with dates | Required for step-therapy rebuttals | Clinician / pharmacy records |
| Lab results (A1C, lipids, BP) | Objective disease burden | Clinician / lab |
| Guideline citations (AHA/ACC, Obesity Medicine Association, Endocrine Society) | Shows your request aligns with standard of care | You / clinician |
| Manufacturer clinical support materials | Novo Nordisk and Eli Lilly both publish appeal-support documents | Manufacturer resources |
| Proof of delivery | Certified mail receipt or portal timestamp — protects you if plan claims nonreceipt | You |
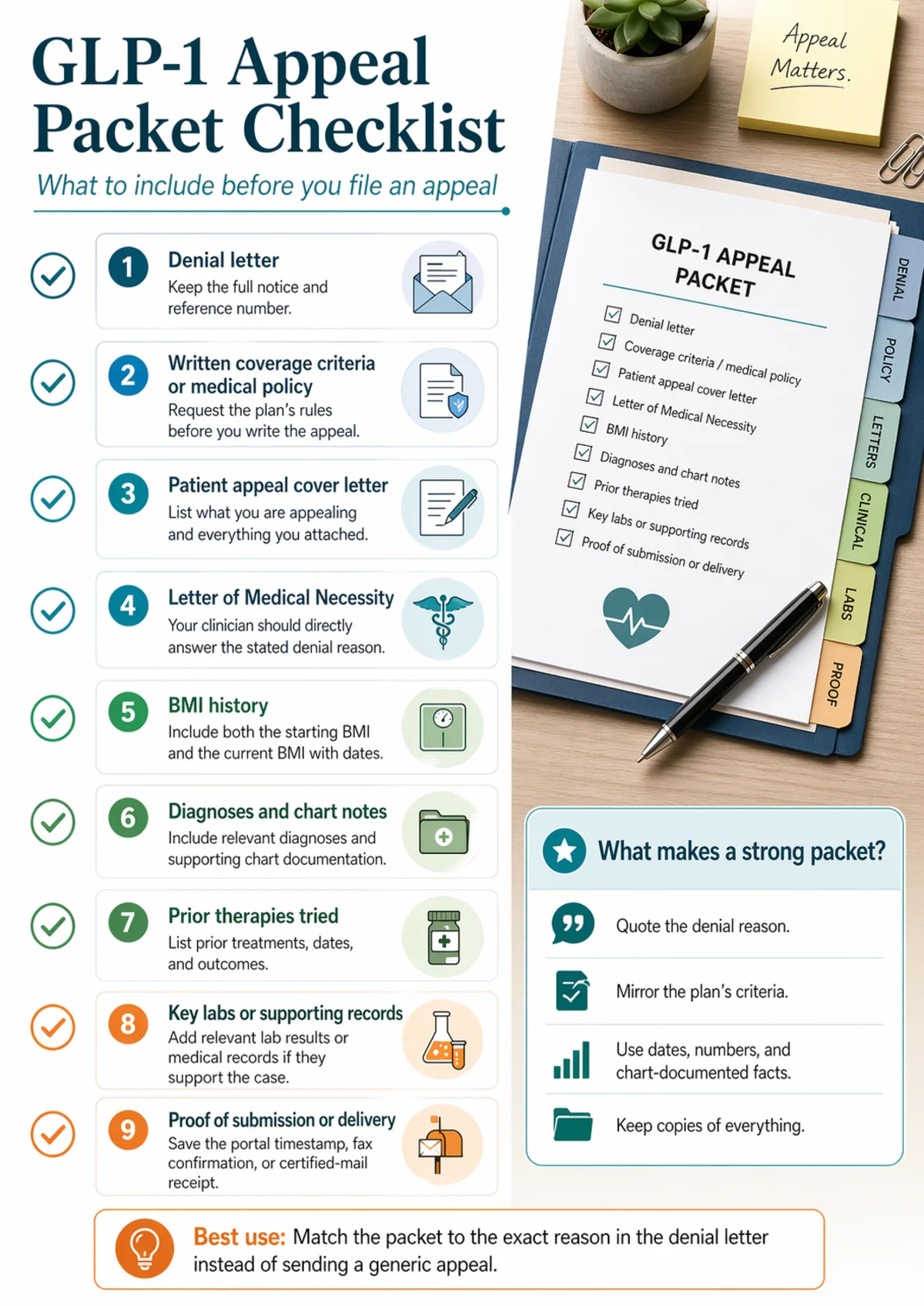
Match the packet to the exact reason in the denial letter. A generic appeal almost never wins.
What the Letter of Medical Necessity must actually say
The LMN is the single highest-leverage document in the packet. A generic LMN fails. A letter that rebuts the specific denial reason with objective data and guideline citations is what overturns denials. A strong GLP-1 LMN contains, at minimum:
- Patient identifiers and the reference number from the denial letter
- Starting BMI and current BMI with dates. Documenting the starting number is a recurring feature of overturned continuation cases.
- Comorbidities with ICD-10 codes — T2D (E11.9), hypertension (I10), OSA (G47.33), hyperlipidemia (E78.5), obesity (E66.01 or E66.9)
- Prior therapy history — every intervention tried, with dates, duration, and outcome
- A direct rebuttal to the stated denial reason — quote the plan’s exact words, then answer each criterion
- Guideline citations — AHA/ACC/TOS obesity management, Obesity Medicine Association, Endocrine Society, and relevant trials (STEP, SELECT)
- The specific ask — drug, dose, duration, and the ICD-10 code supporting the indication
- Clinician signature, credentials, contact, and NPI
What NOT to put in an LMN
- Vague narrative (“the patient has struggled with weight for years”)
- Self-reported history without chart documentation
- Emotional language with no clinical substance
- Citations to blog posts or telehealth marketing pages
Real GLP-1 appeal cases: what actually got overturned?
Real public external-review decisions are the closest thing to X-ray vision into how independent reviewers decide these cases. We read three publicly documented GLP-1 rulings from state insurance regulators in full. Two got overturned. One got upheld. The patterns tell you more than any generic appeal guide ever will.
Important: These are real public cases verified against source documents. Public appeal decisions skew toward people who fought far enough to reach external review. Treat them as pattern evidence, not a promise.
Case #1 — Fidelis Care, Wegovy continuation, BMI 54 → 24.4
An adult female with obesity, fatty liver, and PCOS had been approved for Wegovy at a starting BMI of 54. She reached her goal at a current BMI of 24.4. Fidelis denied continuation because her current BMI was “below 25.”
The external reviewer overturned the denial. The decision cited Endocrine Society guidelines recommending continuation of weight-loss medications when patients have maintained at least 5% body weight loss, noted the high risk of regaining weight and developing T2D without Wegovy, and rejected the logic that success on the drug should be grounds to stop it.
What changed the outcome: The reviewer treated obesity as a chronic condition requiring ongoing management. The packet made that argument with specific numbers and a named clinical guideline.
Source: NY DFS Public Appeal #202303-160505 · Decision year: 2023 · Appeal agent: MCMC, LLC
Case #2 — Oxford, Wegovy continuation, 187 → 163 lbs
A female patient aged 60–69 had been on Wegovy for roughly six months. Starting weight 187 pounds, current weight 163 — more than 5% loss, maintained. Oxford denied continuation.
The external reviewer overturned. The decision cited AHA/ACC/The Obesity Society guidelines on pharmacotherapy for BMI ≥30 (or ≥27 with comorbidities) and noted that 5%+ maintained weight loss supports continuation under both FDA approval and national guidelines. The reviewer concluded the health plan “did not act reasonably with sound medical judgment in the best interest of the patient.”
What changed the outcome: Objective weight documentation, a 5%+ loss threshold matching published guidelines, and an appeal that put starting BMI, current BMI, and maintained loss in front of the reviewer.
Source: NY DFS Public Appeal #202209-153866 · Decision year: 2022 · Appeal agent: IPRO
Case #3 — BCBSM, Zepbound for OSA (the honest counterexample)
A Michigan patient on Zepbound had lost over 36 pounds with A1C improving from 5.9 to 5.1. When her insurer dropped all GLP-1s prescribed for weight loss, her clinician re-submitted under Zepbound’s FDA-approved obstructive sleep apnea indication (documented severe OSA). BCBSM still denied. The Michigan DIFS Director upheld the denial on external review.
The reasoning: Zepbound was listed as a “not covered” drug under the plan’s own contract, and a true non-covered-benefit exclusion is a contractual question, not a medical-judgment question — so the drug wasn’t covered regardless of the FDA-approved indication invoked.
What this tells you: An FDA-approved indication on a different diagnosis is a legitimate strategy for some plans — but it cannot override a contractual exclusion for the drug itself. The appeal has to line up with what your specific plan actually covers in writing.
Source: Michigan DIFS External Review File No. 236103-001, decided 2025
What the patterns tell you
For continuation denials (Cases 1 and 2): document starting BMI alongside current BMI, cite 5%+ maintained weight loss, and frame obesity as a chronic condition requiring ongoing pharmacotherapy.
For plan-exclusion denials (Case 3): even a strong clinical case can lose when the plan contract excludes the drug itself. You need a different play — covered in the plan exclusion section below.
If your BMI is lower now because the drug worked — can you still appeal?
Often, yes. Independent reviewers have repeatedly overturned these denials when the packet frames the situation correctly. Cases 1 and 2 above are textbook examples — one patient went from BMI 54 to 24.4 and still won continuation.
The reframe that wins these appeals
Most insurers write reauthorization rules assuming weight loss means the problem is solved. But obesity medicine guidelines from the Endocrine Society, the Obesity Medicine Association, and AHA/ACC/TOS treat obesity as a chronic condition that usually requires ongoing pharmacotherapy to maintain results. That framing needs to be explicit in your packet.
What to put in the packet
- Starting BMI with the date it was measured (not just current BMI)
- Percent of starting body weight lost and maintained (the 5% threshold is in multiple published guidelines)
- A citation to maintenance-therapy guidelines — Endocrine Society, AHA/ACC/TOS, Obesity Medicine Association
- A clinician statement that stopping the medication is expected to lead to weight regain and return of comorbidity risk
- Any improvements in comorbidities — A1C reductions, blood pressure improvements, lipid changes
Appeal deadlines and routes by plan type
The single worst mistake on this whole page is missing your deadline. Look at your denial letter for the exact date, and confirm receipt of everything you send.
| Plan type | Internal appeal deadline | Insurer response window | Next escalation |
|---|---|---|---|
| Fully-insured commercial | Usually 180 days | 30 days pre-service; 60 days post-service; 72 hrs urgent | State external review |
| Self-funded employer (ERISA) | Typically 180 days | 30 days pre-service; 60 days post-service; 72 hrs urgent | External review + employer-level exception request |
| ACA marketplace | 180 days | 30 days pre-service; 60 days post-service; 72 hrs urgent | State or federal external review (via MAXIMUS) |
| Medicare Part D | 65 days for redetermination | 7 days standard; 72 hrs expedited | IRE reconsideration → ALJ → Medicare Appeals Council → Federal Court |
| Medicaid | State-dependent (often 90–120 days) | State-dependent | State fair hearing |
External review: Under the ACA, if your internal appeal is denied, you have a federally guaranteed right to external review by an Independent Review Organization with no financial tie to your insurer. The review is free, or capped at $25 for most ACA-compliant plans. Standard decisions come no later than 45 days; urgent cases within 72 hours. The decision is binding on the insurer.
Expedited appeals: Request expedited review when a delay could seriously jeopardize your life, health, or ability to regain function. Your clinician needs to certify urgency in writing. Expedited decisions must come within 72 hours for commercial, ACA, and Medicare plans.
What if your plan excludes weight-loss drugs entirely?
The honest admission: If your denial letter genuinely says the drug is excluded from plan benefits, a standard medical-necessity appeal is probably not going to save you. Most guides dance around this. We won’t — because sending you into a months-long fight that ends where it started serves no one.
“Usually doesn’t win” isn’t the same as “quit.” Three paths still work.
Path 1 — Re-prescribe under a covered indication
If you have one of these diagnoses, your clinician may be able to prescribe a GLP-1 under an FDA-approved indication your plan does cover:
- Type 2 diabetes → Ozempic, Mounjaro, Rybelsus carry FDA approval for T2D and are covered by most plans
- Established cardiovascular disease → Wegovy FDA-approved (March 2024) to reduce CV event risk in adults with established CVD and overweight or obesity
- Moderate-to-severe obstructive sleep apnea → Zepbound FDA-approved for OSA in adults with obesity (though as Case #3 shows, this doesn’t beat a drug that’s contractually excluded)
- MASH → Wegovy FDA-approved for metabolic dysfunction-associated steatohepatitis in eligible adults
Path 2 — Employer-level benefit exception (self-funded plans only)
On a self-funded employer plan, the plan administrator can’t say yes — only the employer can. This path is massively underused.
- Ask HR who has authority over individual exceptions and what the escalation process is
- Request the SPD and any written exception criteria
- For future plan years, submit a formal benefits request at open enrollment — this is how GLP-1 coverage gets added in response to employee demand
Path 3 — Push into external review if any part involves medical judgment
If the denial blends exclusion reasoning with any clinical reasoning (“not covered for your diagnosis,” “plan covers this drug for certain conditions but not others”), external review can sometimes pull the case into medical-judgment territory. Case #3 shows this doesn’t always work when the drug itself is contractually excluded — but if your letter is mixed, file for external review and let the IRO decide.
Not sure if your plan actually excludes the drug or just requires a PA you haven’t completed?
Check my GLP-1 coverage with Ro — free report → (sponsored affiliate link, opens in a new tab)Ro’s free GLP-1 Insurance Coverage Checker calls your insurer and emails a personalized report: whether each FDA-approved GLP-1 is covered, the estimated copay, and whether prior authorization is required. Free to use before you write a single word of an appeal. We earn a commission if you enroll through our link, at no cost to you.
| Ro service detail | Verified (April 22, 2026) |
|---|---|
| Free coverage checker | Yes — Ro calls your insurer and emails a personalized coverage report. |
| Ro Body membership | $39 for the first month; $149/month ongoing; or as low as $74/month with annual plan. |
| Medication cost | Billed separately from membership. Depends on insurance or cash-pay option. |
| Cash-pay FDA-approved GLP-1s | Wegovy pen, Wegovy pill, Foundayo pill, Zepbound KwikPen, Ozempic. |
| Insurance-eligible GLP-1s through Ro | Zepbound pen, Wegovy pen, Ozempic. |
| Insurance concierge | Yes — submits PA paperwork, fights denials, resubmits appeals, can switch between clinically appropriate FDA-approved GLP-1s if one is denied. |
| Government insurance | Ro cannot coordinate coverage for most government plans. FEHB members can access the concierge. |
What if the first appeal loses?
A first loss is not the end. Most plan types have a second level, and external review overturns a meaningful share of what comes to it.
Commercial / ACA plans: External review by an IRO — free or ≤$25, binding on the insurer, 45 days standard / 72 hours urgent.
Medicare Part D: IRE reconsideration → ALJ hearing → Medicare Appeals Council → Federal Court.
Medicaid: State fair hearing (administrative law judge, independent of the managed-care organization).
Self-funded ERISA plans: External review is available; civil action under ERISA is theoretically possible but rarely practical at the individual-prescription level.
What to change in round two
Don’t just resubmit the first packet. Address anything new the Level 1 denial raised. Request a peer-to-peer review between your clinician and the plan’s medical director — some denials get resolved at that conversation rather than proceeding to formal external review.
Peer-to-peer script for your clinician
“Dr. [medical director], I’m requesting approval of [medication] for [patient]. Patient has BMI [X] with [comorbidities, each with ICD-10 code]. Patient has failed or had contraindications to [prior therapies with dates]. Denial cited [plan’s exact language]. Clinical basis for necessity: [two sentences]. Supporting evidence: [SELECT trial for CV risk, STEP trials for obesity outcomes], AHA/ACC/TOS and Obesity Medicine Association guidelines. Requesting approval at [dose] for [duration].”
If the appeal is a real dead end
Sometimes the honest answer is that the appeal path is blocked. If that’s where you are, stop spending energy on the fight and switch to a working access path.
Option 1 — Manufacturer assistance programs
Novo Nordisk offers savings cards and patient assistance for Wegovy and Ozempic. Eli Lilly's Lilly Cares foundation provides income-qualified assistance — check lillycares.com for current details.
Option 2 — Manufacturer direct cash-pay
NovoCare delivers cash-pay Wegovy at manufacturer-published prices. LillyDirect offers Zepbound (vials starting at $299/month) and Foundayo (starting at $149/month) with free delivery.
Option 3 — FDA-approved GLP-1s via telehealth at manufacturer-matched pricing
Telehealth platforms including Ro match NovoCare and LillyDirect pricing on FDA-approved brand-name GLP-1s and bundle provider care and insurance concierge support.
Option 4 — Open enrollment leverage for next plan year
Your single most powerful long-term lever is annual open enrollment. Submit a formal benefits request to HR, cite the total cost-of-care argument, and build a coalition of coworkers with the same concern.
Not sure which path fits your situation?
Get my personalized GLP-1 action plan →Free quiz covers your denial reason, plan type, starting BMI, and what you’ve already tried. Returns a tailored action plan. No sign-up required.
Common mistakes that kill a GLP-1 appeal
Missing the deadline. The single most unforgivable mistake. Use a calendar reminder the day you receive the denial.
Appealing in the wrong category. Filing a medical-necessity appeal against a plan exclusion. The Denial Decoder at the top of this page exists for a reason.
Using a generic LMN. Most losing appeals use a clinician letter that describes the patient without addressing the plan's specific stated denial reason.
Self-reported history without chart documentation. "Patient reports trying Phentermine" rarely wins. "Patient prescribed Phentermine 37.5 mg on [date], discontinued [date] due to [reason], documented in chart" often does.
Current BMI without starting BMI in continuation appeals. Reviewers need both numbers to see the trajectory. Cases 1 and 2 were won in part because starting BMI was documented alongside current BMI.
Failing to request the plan's written medical policy before appealing. You can't rebut criteria you've never read.
Not saving proof of delivery. Certified mail receipt or portal timestamp. Always.
Writing the whole appeal yourself without the clinician involved. Patient-filed appeals work legally, but the clinical argument has to come from your prescriber.
Assuming the first denial is final. Every ACA-compliant plan has internal and external appeal rights built in.
Frequently asked questions
How long do I have to appeal a GLP-1 insurance denial?
Commercial and ACA plans typically allow up to 180 days to file an internal appeal. Medicare Part D gives 65 days for redetermination. Medicaid fair-hearing deadlines vary by state but are often 90 to 120 days. Your denial letter must state the exact deadline under federal rule -- check the letter rather than relying on a generic answer.
Can I appeal if my BMI is lower now because the medication worked?
Often, yes. Public external-review decisions consistently overturn continuation denials where the packet documents starting BMI, 5% or more maintained weight loss, and obesity-as-chronic-disease guidelines from the Endocrine Society, AHA/ACC/TOS, and Obesity Medicine Association. Two of the three real cases we covered on this page were continuation denials that got overturned on exactly this basis.
Can my doctor appeal for me?
Yes. You can appoint your clinician as an authorized representative using a simple authorization form. Whether a patient or a representative files, the appeal timelines under federal rule are the same -- what matters is filing on time with a strong clinical packet.
What if Wegovy, Zepbound, or Mounjaro is excluded from my plan?
A standard medical-necessity appeal usually will not beat a true plan exclusion. Your three real options are: re-prescribe under a covered FDA-approved indication (type 2 diabetes, established cardiovascular disease, moderate-to-severe obstructive sleep apnea) if clinically appropriate; request an employer-level exception if your plan is self-funded; or push the denial into external review if any part of it involves medical judgment rather than pure contract language.
What if my Zepbound was denied after prior approval?
Continuation denials after prior approval are common and winnable with the right packet. Include starting BMI, the drug's clinical response for you (weight loss and comorbidity improvements), and a citation to maintenance-therapy guidelines from the Endocrine Society and AHA/ACC/TOS. See Cases 1 and 2 on this page for the patterns that got two such denials overturned.
What is the difference between an internal appeal and an external review?
An internal appeal is your first challenge to the denial, reviewed by the insurance company's own clinical staff. An external review is a second-chance review by an Independent Review Organization (IRO) with no financial tie to your insurer. External review is free or capped at $25 on most ACA-compliant plans, and the IRO's decision is binding on the insurer.
What if I have Medicare Part D?
Medicare runs its own process: coverage determination, then redetermination (65 days to file), then Independent Review Entity reconsideration, then Administrative Law Judge hearing, then Medicare Appeals Council, then Federal Court. Expedited appeals decide within 72 hours. The Medicare GLP-1 Bridge runs July 1, 2026–December 31, 2027 (18 months), providing eligible beneficiaries access to Wegovy (injection and tablets), Zepbound KwikPen, and Foundayo for weight reduction at $50/month. Bridge eligibility requires specific BMI and comorbidity criteria per CMS. BALANCE will not launch for Medicare Part D in 2027 — the 80% participation threshold was not met.
What if I have Medicaid?
Every state Medicaid program must offer a fair hearing -- an administrative hearing usually before an independent administrative law judge. Deadlines and rules vary by state. As of January 2026, KFF reported that 13 state Medicaid fee-for-service programs covered GLP-1s for obesity treatment; managed-care coverage may differ. Check your state's current formulary before assuming coverage.
Related guides
- Employer GLP-1 coverage 2026: dead end or fixable?
- Does CVS Caremark cover Wegovy? 2026 formulary and PA guide
- Does TRICARE cover GLP-1 medications in 2026?
- How to ask your employer to cover GLP-1s: script and strategy
- GLP-1 providers that accept HSA and FSA in 2026
- Best telehealth providers for GLP-1 access in 2026
How we built this guide
We’re The RX Index editorial team — a pricing intelligence and comparison resource for GLP-1 telehealth providers. We are not attorneys, licensed insurance agents, or medical providers. This page is informational, not legal, medical, or insurance advice.
What we did: Pulled appeal timelines from HealthCare.gov, CMS, and 45 CFR 147.136 directly. Verified three public GLP-1 external-review decisions against source documents. Cross-checked KFF’s claims-denial analysis. Verified Ro’s pricing, drug list, and concierge scope against Ro’s public pages. Confirmed Medicare GLP-1 Bridge design against CMS’s live page (last CMS modification March 10, 2026).
What we didn’t do: No “medically reviewed by” tag. No compounded GLP-1 providers cited on this page. No testimonials we couldn’t verify.
Refresh schedule: monthly on pricing and provider offers; quarterly on federal and state rules; immediate on any CMS or FDA update. To report an error: contact us.
Primary sources
- HealthCare.gov — Internal Appeals
- HealthCare.gov — External Review
- CMS — Medicare Part D Redetermination
- CMS — Medicare GLP-1 Bridge
- NY DFS — Public Appeal #202303-160505 (overturned)
- NY DFS — Public Appeal #202209-153866 (overturned)
- Michigan DIFS — External Review File No. 236103-001 (upheld)
- KFF — Claims Denials and Appeals in ACA Marketplace Plans in 2024
- KFF — Medicaid coverage of and spending on GLP-1s
- 45 CFR § 147.136
- Lilly Cares Foundation
Last verified: April 22, 2026. Next scheduled refresh: May 22, 2026. The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We earn affiliate commissions when readers sign up with Ro through our links. We do not earn commissions from NovoCare, LillyDirect, or Lilly Cares links. Our editorial analysis is applied before commercial considerations. GLP-1 medications carry a boxed warning about the risk of thyroid C-cell tumors in rodents; do not use if you or your family have a history of MTC or MEN 2 syndrome. Information on this page does not constitute medical, legal, or insurance advice. Consult your prescribing clinician about your specific situation, and consult a licensed attorney or insurance professional for case-specific questions about appeal rights, ERISA, or state insurance law.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 60 seconds · no signup