Medicare GLP-1 Bridge Program Explained: Who Qualifies, What It Costs, and How to Get It
We built this guide to be the only page you need. Whether you qualify for the Bridge, need to use regular Part D, or want alternatives while you wait — we'll walk you through every path and every decision, step by step.
| Your situation | Your path |
|---|---|
| BMI ≥ 35 (no other conditions needed) | ✅ You likely qualify for the Bridge |
| BMI ≥ 30 + heart failure, uncontrolled hypertension, or CKD Stage 3a+ | ✅ You likely qualify for the Bridge |
| BMI ≥ 27 + prediabetes, prior heart attack, prior stroke, or peripheral artery disease | ✅ You likely qualify for the Bridge |
| BMI below 27 or no qualifying conditions | ❌ Bridge won't apply — but you have other options |
| Not enrolled in Part D for 2026 | ❌ Must have Part D — see alternatives below |
| Already getting a GLP-1 for diabetes, heart disease, or sleep apnea through Part D | ⚠️ You use Part D, not the Bridge — your drug is already coverable |
What Is the Medicare GLP-1 Bridge Program?
The Medicare GLP-1 Bridge is a temporary demonstration program run by the Centers for Medicare & Medicaid Services (CMS). It provides eligible Medicare Part D beneficiaries with access to FDA-approved GLP-1 weight loss medications at a $50 monthly copay.
Here's the essential context: federal law has prohibited Medicare from covering medications prescribed solely for weight loss since 2003. That means for over two decades, Medicare generally did not cover GLP-1s when prescribed only for weight loss — so beneficiaries who wanted Wegovy or Zepbound for weight management alone usually needed a cash-pay path outside of Medicare. At list prices above $1,000 per month, that put treatment out of reach for most people on a fixed income.
The Bridge changes that — temporarily.
CMS announced the program on December 23, 2025, and released the detailed FAQ on March 3, 2026. It uses a special legal authority (Section 402 of the Social Security Amendments) to operate outside the normal Part D system. That's important because it means:
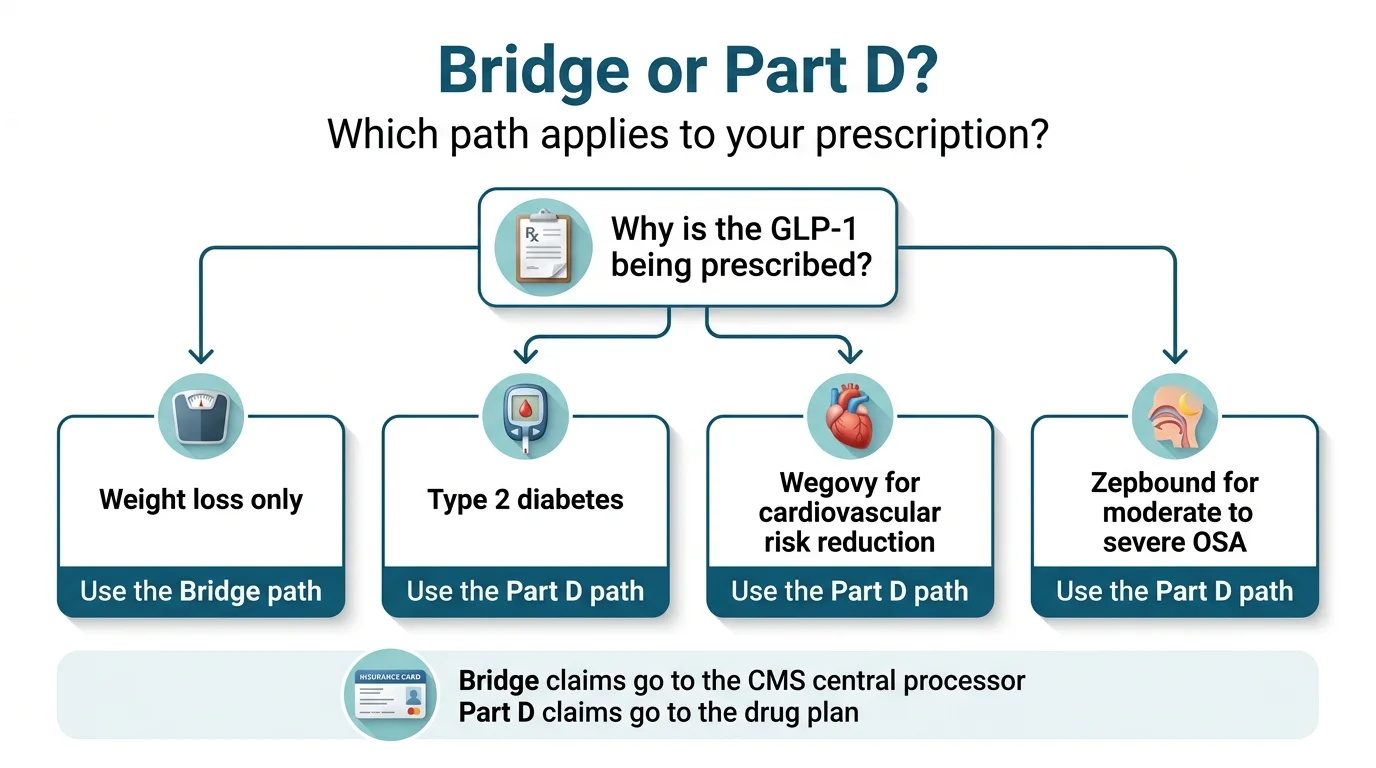
- Your Part D plan does not need to “opt in.” The Bridge is administered directly by CMS through a central processor.
- Your Part D plan is not directly involved in Bridge claims or payment. Bridge prior authorizations go to CMS's central processor, not your plan. Standard Part D coverage decisions still go through your plan as usual.
- Pharmacies do not need to opt in to the Bridge. CMS is still issuing operational guidance, but pharmacies are not required to enroll separately.
The Bridge runs from July 1 through December 31, 2026 — six months, not a day longer. After that, continued Medicare coverage for weight-loss GLP-1s depends on the BALANCE Model launching in Medicare for 2027 and your enrollment in a participating Part D plan. That transition is not automatic — we'll explain exactly why it matters later.
Do You Qualify for the Medicare GLP-1 Bridge?
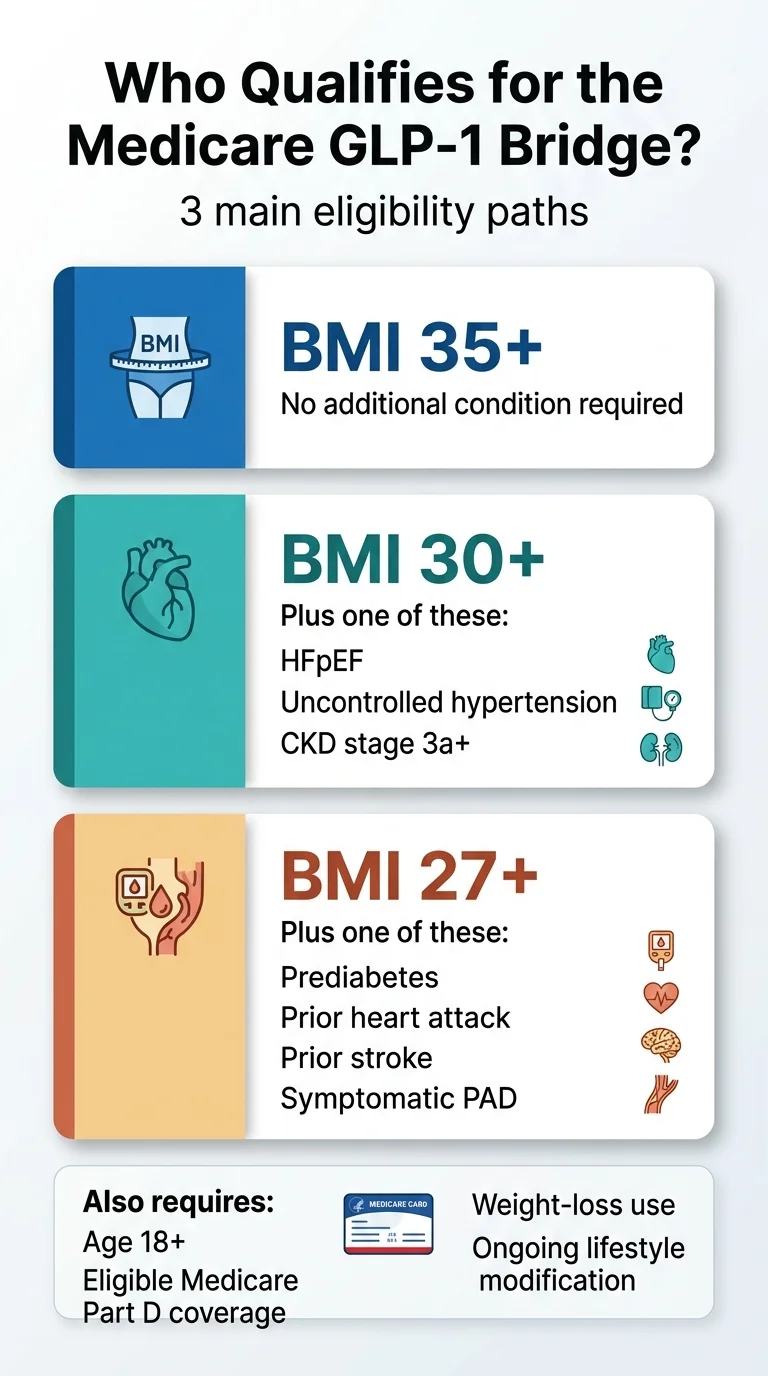
CMS published specific eligibility criteria in the March 2026 FAQ, and they're more detailed than most news articles let on. There are three distinct tiers, and you only need to meet one of them — plus baseline requirements that apply to everyone.
Requirements That Apply to Everyone
- Enrolled in Medicare Part D for 2026 — either a standalone Prescription Drug Plan (PDP) or a Medicare Advantage plan with drug coverage (MA-PD).
- Special Needs Plans (SNPs), employer/union group waiver plans (EGWPs), and LI NET are all eligible.
- Not eligible: private fee-for-service plans, Section 1876 cost contract plans, Section 1833 health care prepayment plans, PACE organizations, fallback plans, and religious fraternal benefit plans — unless you're also enrolled in a standalone PDP.
- Dual-eligible beneficiaries (enrolled in both Medicare and Medicaid) can qualify if they're in an eligible Part D plan type.
- The medication must be prescribed for weight loss — specifically, “to reduce excess body weight and maintain weight reduction in combination with current and ongoing lifestyle modification including structured nutrition and physical activity.”
Tier 1: BMI of 35 or Higher
This is the simplest path. If your Body Mass Index is 35 or above at the time you start GLP-1 therapy, you qualify with no additional diagnosis required.
For reference: a person who is 5'6“ and weighs 217 pounds has a BMI of approximately 35. A person who is 5'10“ and weighs 244 pounds has a BMI of approximately 35. Your doctor attests to your BMI and confirms you're committed to ongoing lifestyle modification. That's it.
Tier 2: BMI of 30 or Higher + Specific Heart or Kidney Conditions
If your BMI is 30 or above but below 35, you can qualify if you also have one or more of the following:
- Heart failure with preserved ejection fraction (HFpEF)
- Uncontrolled hypertension — defined as systolic BP above 140 mm Hg or diastolic above 90 mm Hg while on two or more antihypertensive medications
- Chronic kidney disease (CKD) stage 3a or above
Tier 3: BMI of 27 or Higher + Specific Cardiovascular or Metabolic Conditions
If your BMI is 27 or above but below 30, you can qualify if you have one or more of the following:
- Prediabetes (as defined by American Diabetes Association guidelines)
- Previous myocardial infarction (heart attack)
- Previous stroke
- Symptomatic peripheral artery disease
Quick BMI Reference
| Height | BMI 27 (Tier 3) | BMI 30 (Tier 2) | BMI 35 (Tier 1) |
|---|---|---|---|
| 5'2" | ~148 lbs | ~164 lbs | ~191 lbs |
| 5'4" | ~157 lbs | ~174 lbs | ~204 lbs |
| 5'6" | ~167 lbs | ~186 lbs | ~217 lbs |
| 5'8" | ~177 lbs | ~197 lbs | ~230 lbs |
| 5'10" | ~188 lbs | ~209 lbs | ~244 lbs |
| 6'0" | ~199 lbs | ~221 lbs | ~258 lbs |
BMI is measured at the time of initiating GLP-1 therapy, not at your all-time highest weight.
What GLP-1 Medications Are Covered Under the Bridge?
This is simpler than you might expect — and also more limited.
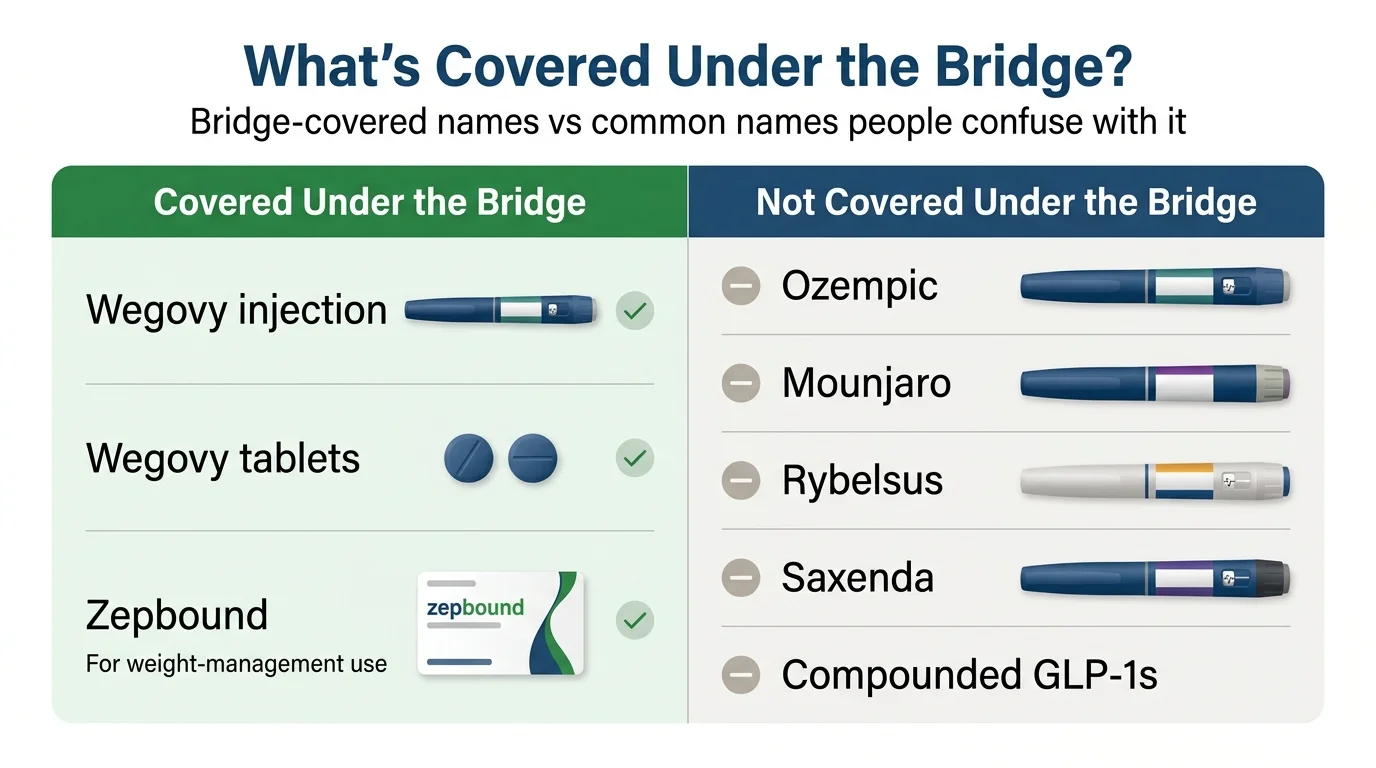
Covered Under the Bridge
| Medication | Active Ingredient | Form |
|---|---|---|
| Wegovy ✓ | Semaglutide | Injection |
| Wegovy ✓ | Semaglutide | Oral tablet |
| Zepbound ✓ | Tirzepatide | Injection |
That's the complete list. Three products, two active ingredients, all FDA-approved specifically for weight loss.
NOT Covered Under the Bridge
| Medication | Why Not? |
|---|---|
| ✗ Ozempic (semaglutide) | FDA-approved for type 2 diabetes, not weight loss |
| ✗ Mounjaro (tirzepatide) | FDA-approved for type 2 diabetes, not weight loss |
| ✗ Rybelsus (oral semaglutide) | FDA-approved for type 2 diabetes, not weight loss |
| ✗ Saxenda (liraglutide) | Not included in Bridge-eligible products |
| ✗ Compounded semaglutide or tirzepatide | Not FDA-approved products |
The Ozempic Question
We know this comes up constantly: “Ozempic and Wegovy are the same active ingredient — can I get Ozempic through the Bridge?” No. Despite containing the same active ingredient (semaglutide), Ozempic and Wegovy are different FDA-approved products with different approved indications. Ozempic is approved for type 2 diabetes. Wegovy is approved for weight management. The Bridge only covers medications prescribed for weight loss, and only covers the specific products listed above.
The Indication Matters More Than the Drug Name
Here's something most articles miss: the same medication can be covered through different pathways depending on why it's prescribed.
- Wegovy for weight loss → Medicare GLP-1 Bridge (July–December 2026)
- Wegovy for cardiovascular risk reduction in adults with established CV disease → regular Medicare Part D (if your plan covers it)
- Zepbound for weight loss → Medicare GLP-1 Bridge
- Zepbound for obstructive sleep apnea in adults with obesity → regular Medicare Part D (if your plan covers it)
How Much Does the Medicare GLP-1 Bridge Really Cost?
The headline number is $50 per month. Eligible beneficiaries pay a flat $50 copay at the pharmacy, regardless of the medication or dose — no tiered pricing, no coinsurance percentage, no deductible to meet first.
But the financial picture is more nuanced than one number.
What the $50 does
- Gives you a one-month supply of Wegovy or Zepbound
- Is the same flat amount regardless of which phase of Part D coverage you're in
- Applies equally whether you're getting the lowest or highest dose
What the $50 does NOT do
- Does not count toward your Part D deductible. Bridge payments exist in a separate financial universe from your regular drug costs.
- Does not count toward your $2,100 annual Part D out-of-pocket spending cap (TrOOP). If you rely on reaching that cap for catastrophic coverage on other expensive medications, Bridge payments won't help you get there.
- Low-Income Subsidy (Extra Help) does not apply. Even if you currently pay $0 for your other Part D medications, you'll still owe the full $50 per month under the Bridge. Over six months, that's $300.
How to Get the Medicare GLP-1 Bridge: Step by Step
The Bridge doesn't work like a normal Part D prescription. Your insurance company isn't involved. There's a different process, and understanding it now — before July — puts you ahead of what will likely be a flood of applicants on launch day.
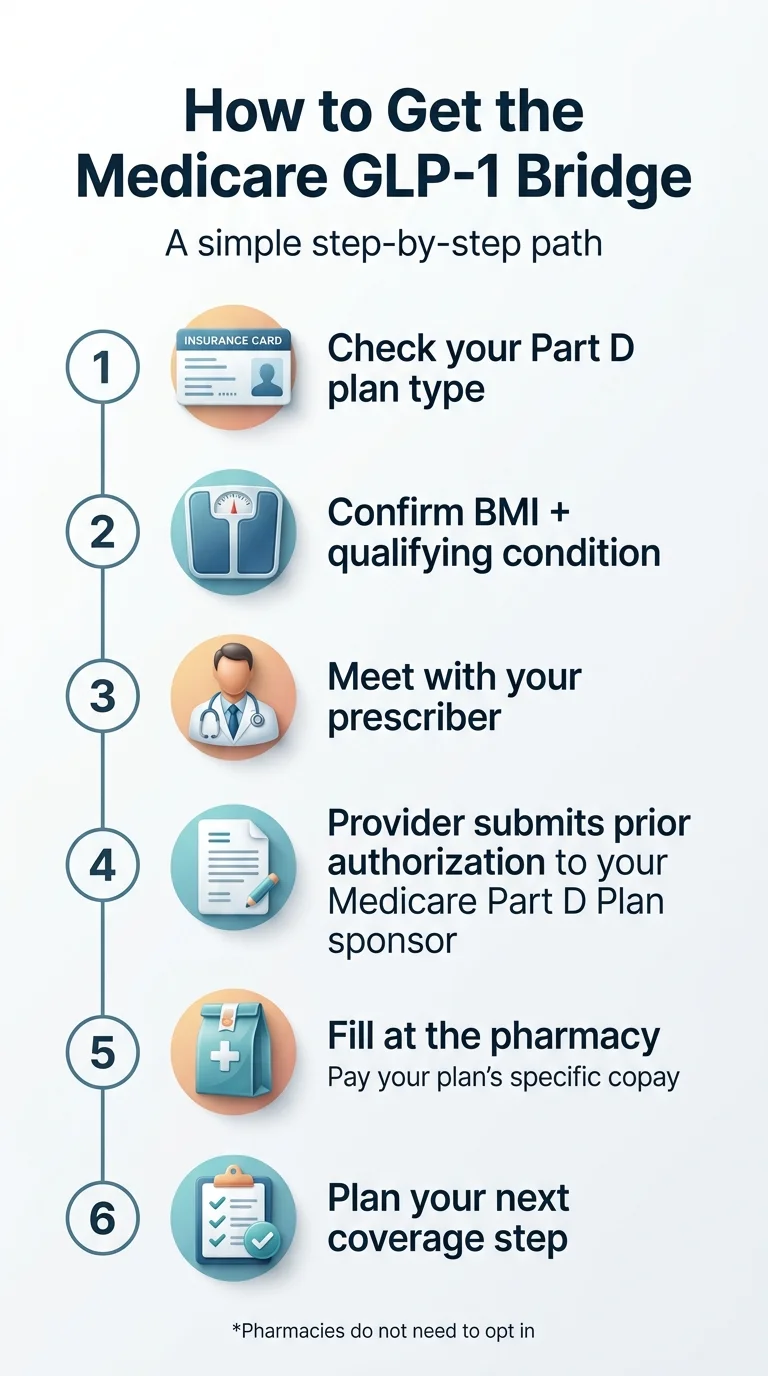
Confirm Your Part D Coverage Type
Check whether your 2026 plan qualifies. Eligible: Standalone PDP, MA-PD (Medicare Advantage with drug coverage), SNPs, EGWPs, LI NET. Not eligible: PACE, private fee-for-service (unless also in a PDP), cost contracts, fallback plans, religious fraternal benefit plans. If you're not sure what type of plan you have, call 1-800-MEDICARE (1-800-633-4227) or check your plan documents at Medicare.gov.
Gather Your Medical Documentation
- Your current BMI — or enough information for your doctor to calculate it. If borderline, get it measured at the office.
- Documentation of qualifying conditions — prediabetes lab results (ADA guidelines), cardiology records for prior heart attack or stroke, blood pressure readings for uncontrolled hypertension, or kidney function tests for CKD.
- Your current medication list — particularly important if you're already on a GLP-1 for another condition.
- Confirmation of lifestyle modification commitment — the prior authorization requires your doctor to attest you're combining medication with structured nutrition and physical activity.
Schedule a Visit With Your Prescriber — Now, Not in July
This is the step most people will delay, and it's the one that costs them the most time. Prior authorizations take time. CMS hasn't specified exact turnaround times yet, and the central processor's workflow is still being finalized. If you wait until July 1 to start the conversation, you'll be competing with every other Medicare beneficiary who saw the same headlines. Schedule a visit in May or June to discuss Bridge eligibility, gather documentation, and prepare the prior authorization so it can be submitted as soon as the program opens.
Your Doctor Submits the Prior Authorization to CMS
This is different from a normal Part D prior authorization. Your doctor sends the request to CMS's central processor — not to your Part D plan. CMS will release detailed submission instructions in Spring 2026. For pharmacies, the Bridge uses BIN: 028918 and PCN: MEDDGLP1BR, effective July 1, 2026.
Fill Your Prescription at the Pharmacy
Once the prior authorization is approved, take your prescription to the pharmacy. Pharmacies don't need to separately opt in. You pay $50 at the counter. The central processor reimburses the pharmacy at wholesale acquisition cost plus a dispensing fee.
Plan for What Comes After December 2026
This step is optional in theory and critical in practice. We cover it in the next section — including the “December Cliff” checklist that ensures you don't lose coverage when the Bridge ends.
What Happens After December 2026? The Transition You Need to Plan For
The Bridge ends December 31, 2026. There is no extension, no grace period, and no automatic continuation.
If you start Wegovy or Zepbound through the Bridge in July and want to continue past December, you'll need to be enrolled in a Part D plan that participates in the BALANCE Model — CMS's longer-term program that launches for Medicare Part D plans on January 1, 2027.
The BALANCE Model Is Voluntary
What the BALANCE Model Changes in 2027
- How it works: Unlike the Bridge (where CMS handles everything directly), BALANCE operates through your Part D plan. Your plan processes claims, manages prior authorization, and handles your prescription like any other Part D drug.
- What it covers: A significantly broader drug list than the Bridge — including Wegovy, Zepbound, Ozempic, Mounjaro, Rybelsus, and others pending FDA approval.
- The cost structure: Not a simple flat-$50 program. Beneficiary cost sharing varies by plan type and benefit phase — some plans cap initial-coverage cost sharing at $50, others at $125; catastrophic phase is $0. Crucially: whatever you pay under BALANCE does count toward your Part D deductible and out-of-pocket cap.
- The lifestyle component: All beneficiaries receiving GLP-1s through BALANCE will have access to a manufacturer-provided lifestyle support program at no additional cost.
Why Stopping a GLP-1 Matters Medically
This isn't just a paperwork issue. In the STEP 1 extension study, participants who stopped semaglutide regained about two-thirds of prior weight loss within one year. GLP-1 medications work while you're taking them. The benefits don't persist once you stop. Starting a GLP-1 in July with no plan for January isn't necessarily the wrong move — six months of treatment can deliver meaningful health improvements — but go in with eyes open and a transition plan in place.
Your December Cliff Checklist
July–August 2026
Start the Bridge program. Begin treatment, manage side effects, and settle into your dose.
September 2026
Check whether your current Part D plan has announced BALANCE participation for 2027. Call your plan or check Medicare.gov.
Oct 15 – Dec 7, 2026 (Open Enrollment)
If your plan is NOT joining BALANCE, research plans that are. Use Medicare's Plan Finder to compare drug coverage for all your medications — not just GLP-1s.
Before December 31, 2026
Have a conversation with your doctor about your 2027 coverage pathway. If BALANCE isn't an option, discuss alternatives.
January 2027 and beyond
Transition seamlessly to BALANCE, or activate your backup plan.
The beneficiaries who maintain their progress will be the ones who plan ahead — not the ones who scramble in December.
Medicare GLP-1 Bridge vs. Standard Part D vs. BALANCE Model
One of the biggest sources of confusion right now is the relationship between three overlapping Medicare GLP-1 pathways. They are not the same thing, and confusing them could cost you time, money, or both.
| Feature | Standard Part D (Today) | GLP-1 Bridge (2026) | BALANCE Model (2027) |
|---|---|---|---|
| When | Available now | July 1 – Dec. 31, 2026 | January 1, 2027+ |
| Covers weight-loss GLP-1s? | ❌ No (prohibited by law) | ✅ Yes (Wegovy, Zepbound) | ✅ Yes (broader drug list) |
| Covers diabetes/CV/OSA GLP-1s? | ✅ Yes (if on formulary) | ❌ No (use Part D instead) | ✅ Yes |
| Who approves claims? | Your Part D plan | CMS central processor | Your Part D plan |
| Plan must opt in? | N/A | ❌ No | ✅ Yes (voluntary) |
| Monthly cost | Varies by plan/tier | $50 flat | Varies by plan/phase ($0–$125) |
| Counts toward Part D OOP cap? | ✅ Yes | ❌ No | ✅ Yes |
| Extra Help/LIS applies? | ✅ Yes | ❌ No | Included under model terms |
| Duration | Ongoing | 6 months only | Through Dec. 2031 |
Which Lane Are You In?
- Weight loss only: The Bridge (July–Dec. 2026), then BALANCE (2027+), is your path. Neither regular Part D nor current law can cover this.
- Type 2 diabetes: Your regular Part D plan may already cover Ozempic, Mounjaro, or Rybelsus. Check your plan's formulary. You do NOT need the Bridge.
- Cardiovascular disease and overweight or obese: Wegovy is FDA-approved for cardiovascular risk reduction. Your Part D plan may cover it for this indication, which is a better deal than the Bridge because Part D payments count toward your out-of-pocket cap and Extra Help applies.
- Obstructive sleep apnea and obesity: Zepbound is FDA-approved for moderate to severe OSA. Same logic — Part D coverage for the sleep apnea indication may be a better financial deal.
Biggest Misunderstandings About the $50 Medicare GLP-1 Program
We've read every major article, official FAQ, and forum thread about this program. These are the most common misunderstandings — each one can lead to wasted time or wrong decisions.
"My Part D plan has to opt in for me to use the Bridge."
Wrong. The Bridge operates entirely outside of Part D. CMS runs the whole thing through a central processor. Your Part D plan doesn't need to opt in, doesn't process Bridge claims, and doesn't bear any financial risk. You just need to be enrolled in an eligible Part D plan type.
"The Bridge is the same thing as the BALANCE Model."
Wrong. The Bridge is a temporary six-month demonstration (July–December 2026). BALANCE is a longer-term model launching in January 2027 that runs through December 2031 and does require Part D plans to voluntarily participate. They have different legal authorities, different timelines, and different rules.
"The Bridge covers all GLP-1 medications."
Wrong. Only Wegovy (injection and oral tablet) and Zepbound are covered. Ozempic, Mounjaro, Rybelsus, Saxenda, and compounded formulations are not.
"The $50 copay will count toward my Part D spending cap."
Wrong. Because the Bridge runs outside of Part D, the $50 does not count toward your Part D deductible, gross covered prescription drug costs, or true out-of-pocket costs (TrOOP). It's financially separate.
"Extra Help will reduce my Bridge copay."
Wrong. The Low-Income Subsidy (Extra Help) does not apply to Bridge prescriptions. Even if you pay $0 for most medications, you'll pay the full $50 under the Bridge.
"If my doctor already prescribes me Zepbound for sleep apnea, I can switch it to the Bridge and save money."
Not how it works. CMS has explicitly stated that if a GLP-1 is prescribed for a use that's coverable under the Part D benefit — regardless of whether your plan actually covers it — you cannot use the Bridge for that drug. CMS says they will monitor plans to prevent coverage shifting.
"This is permanent Medicare GLP-1 coverage."
Wrong. The Bridge ends December 31, 2026. Period. Continuation depends on the BALANCE Model launching successfully in 2027, your Part D plan participating in BALANCE, and you being enrolled in a participating plan.
What Medicare Already Covers Without the Bridge
Before you pursue the Bridge, it's worth checking whether you already have a GLP-1 coverage pathway you might not know about. Many Medicare beneficiaries do — and the regular Part D pathway can actually be better than the Bridge because it counts toward your out-of-pocket cap and Extra Help applies.
GLP-1s for Type 2 Diabetes
If you have type 2 diabetes, your Part D plan may cover Ozempic (semaglutide injection), Mounjaro (tirzepatide injection), or Rybelsus (oral semaglutide). Coverage depends on your plan's formulary and may require prior authorization or step therapy — but the coverage exists and has existed for years.
Wegovy for Cardiovascular Risk Reduction
Wegovy is FDA-approved to reduce the risk of major adverse cardiovascular events in adults with established cardiovascular disease who are also overweight or obese. If you meet that description, your Part D plan may cover Wegovy for the cardiovascular indication. This has nothing to do with the Bridge.
Zepbound for Obstructive Sleep Apnea
Zepbound has FDA approval for treating moderate to severe obstructive sleep apnea in adults with obesity. If you have OSA, your Part D plan may cover Zepbound for that indication. See our full guide on Medicare coverage for Zepbound.
What Beneficiaries Are Actually Asking Right Now
We monitor forums, Medicare communities, and reader questions to understand what real beneficiaries are confused about. Here are the themes that keep coming up.
"I'm confused about what 'meet the criteria' and 'eligible beneficiaries' actually means."
This comes up in nearly every Medicare forum thread about the Bridge. It means the three BMI/diagnosis tiers we outlined above. If you meet any one of them and are in an eligible Part D plan, you're a candidate. Your doctor attests to the criteria in the prior authorization.
"Can I get a GLP-1 covered for prediabetes?"
Under the Bridge (starting July 2026), prediabetes is a qualifying condition — but only in combination with BMI of 27 or higher (Tier 3). Before the Bridge launches, Medicare does not cover GLP-1s for prediabetes through standard Part D.
"I'm already paying over $1,000/month out of pocket. Can I switch to $50?"
If you're currently self-paying for Wegovy or Zepbound specifically for weight loss and you meet the Bridge criteria, yes — starting July 1, 2026, you should be able to transition to Bridge coverage and pay $50/month. Talk to your prescriber about submitting the prior authorization to the CMS central processor before July. That alone could save you over $6,000 in the second half of this year.
"My doctor prescribed Zepbound for sleep apnea. Can I use the Bridge instead since it's cheaper?"
Probably not. If Zepbound is prescribed for sleep apnea — which is a Part D-coverable indication — CMS says you cannot use the Bridge for that drug. You'd need to continue through your Part D plan. The Bridge is only for weight-loss-only prescriptions.
What If You Don't Qualify for the Medicare GLP-1 Bridge?
Not everyone will qualify — and that's the reality we need to address honestly. Maybe your BMI doesn't meet the thresholds. Maybe you're in a plan type that's excluded. Maybe you don't have one of the specific qualifying conditions. Or maybe you just don't want to wait until July. Whatever the reason, you are not out of options.
Option 1: Check Whether Regular Part D Already Covers Your GLP-1
If you have type 2 diabetes, cardiovascular disease, or obstructive sleep apnea, your Part D plan may already cover a GLP-1 for that condition. This is the first thing to check because it costs you nothing to investigate and uses the coverage you're already paying for. Call the number on the back of your Part D card and ask: “Does my plan cover [Ozempic / Wegovy / Zepbound] for [your condition]? What's the prior authorization process?”
Option 2: FDA-Approved GLP-1 Through a Telehealth Provider
If regular Part D doesn't apply and the Bridge doesn't either, you can still access FDA-approved Wegovy and Zepbound through telehealth medical programs — without waiting for any government program to launch.
Ro is the most comprehensive option we've evaluated for this. Their Body program pairs you with a licensed physician who evaluates your health, prescribes FDA-approved GLP-1 medication if appropriate, and provides ongoing clinical support including dose management and side-effect guidance. The membership starts at $45 for the first month and $145/month after that, with medication billed separately. Cash-pay medication options start at $149/month for lower doses.
What makes Ro worth highlighting here: it's month-to-month with no long-term contract, so you can start now and transition to Bridge or BALANCE coverage later without penalty. It also serves as a smart insurance policy — if BALANCE doesn't materialize in 2027 or your plan doesn't participate, you already have a clinical relationship and treatment plan in place.
FDA-Approved Wegovy & Zepbound — Available Now
See if you qualify for FDA-approved GLP-1 treatment through Ro
Licensed physicians, FDA-approved medication, no long-term commitment. Month-to-month — start now, transition to Bridge in July if you qualify. Cash-pay path only; cannot coordinate Medicare coverage.
Check eligibility on Ro →Self-pay path. Ro cannot coordinate GLP-1 coverage for government insurance plans.
Option 3: Compounded GLP-1 Programs
For beneficiaries on tighter budgets where brand-name medication pricing isn't feasible, compounded GLP-1 programs offer a lower entry point.
We want to be clear about what this means: compounded GLP-1 products are not FDA-approved finished drugs. The FDA does not review them for safety, effectiveness, or quality before they are marketed, and the agency has raised concerns about dosing inconsistencies and misleading promotional claims in this category. This is not the same as saying they are dangerous — but you should understand the distinction before deciding.
MEDVi is the strongest option we've evaluated in this category. They offer compounded semaglutide and tirzepatide starting at $179 per month with no membership fees, no contracts, and month-to-month billing. Treatment is overseen by licensed physicians, and medications ship from licensed U.S. compounding pharmacies.
Most Affordable GLP-1 Option
See current MEDVi pricing — compounded GLP-1 from $179/mo
Licensed physicians, U.S. compounding pharmacies, no membership fees, no contracts. Compounded semaglutide and tirzepatide. Not FDA-approved finished drugs — understand the distinction before deciding.
See MEDVi pricing →Option 4: TrumpRx Self-Pay Pricing
TrumpRx.gov is a government-backed platform offering reduced self-pay prices on brand-name GLP-1 medications. Check TrumpRx.gov directly for current figures, as they update periodically. Note that patients covered by government insurance programs like Medicare and Medicaid may face eligibility restrictions on certain discount programs offered through the platform.
Choosing Your Path
| Your Situation | Best Next Step |
|---|---|
| You have a Part D-coverable condition (diabetes, CV disease, OSA) | Call your Part D plan — regular coverage may be your best deal |
| You want FDA-approved medication and can invest in clinical support | Check eligibility on Ro |
| You need the most affordable starting point possible | See pricing on MEDVi |
| You want to start now and transition to Bridge in July | Start with Ro or MEDVi, then switch |
Can't Wait Until July? How to Start GLP-1 Treatment Now
The Bridge doesn't open until July 1, 2026. If you've been thinking about GLP-1 treatment — if you've watched the news coverage, talked to friends who've had success, or discussed it with your doctor — you don't have to wait three more months to begin.
Many people use the months before July to start their GLP-1 journey, build the habit, manage initial side effects (which are often most noticeable in the first few weeks), and get to a stable dose. By the time Bridge coverage kicks in, they're already seeing results and can transition their coverage to $50/month.
Why Starting Early Is Medically Smart
GLP-1 medications use a dose titration schedule. You don't start at the full dose. Wegovy begins at 0.25 mg weekly and gradually increases over about 16–20 weeks to reach the maintenance dose of 2.4 mg. Zepbound starts at 2.5 mg and titrates up to 15 mg over a similar period. During those early weeks, side effects like nausea, constipation, or decreased appetite are most common. Most patients find they diminish significantly as the body adjusts. If you start in April or May, you'll be through the toughest adjustment period before the Bridge even launches.
Here's What the Timeline Looks Like
Today or this week
Complete a telehealth evaluation through a provider like Ro (FDA-approved) or MEDVi (compounded)
Weeks 1–4
Begin at the starting dose. Manage any initial side effects with your provider's guidance.
Weeks 5–12
Gradually increase to a higher dose. You'll typically start seeing meaningful weight loss in this period.
Late June
Talk to your prescriber about submitting the Bridge prior authorization to CMS's central processor.
July 1
Transition to $50/month coverage through the Bridge if you qualify. Your treatment continues seamlessly — same medication, different payment pathway.
The Financial Math of Starting Early
Yes, you'll pay more per month before July. But consider: three months of waiting is three months of not losing weight, not improving your health markers, and then scrambling to start from scratch while everyone else floods the prior authorization system at once. For many people, the health improvements in those first three months — lower blood pressure, better blood sugar, reduced inflammation, improved mobility — are worth the investment even before Bridge pricing kicks in.
Start Now — Don't Wait Until July
Start a free GLP-1 medical evaluation on Ro
FDA-approved Wegovy and Zepbound with licensed physicians, ongoing clinical support, and home delivery. Month-to-month — transition to Bridge coverage in July if you qualify. Cash-pay path only.
Start free GLP-1 evaluation on Ro →Self-pay path. Ro cannot coordinate GLP-1 coverage for government insurance plans.
What These Medications Actually Do
The Bridge hasn't launched yet, so there are no Bridge-specific patient outcomes to report. But the medications it covers — Wegovy and Zepbound — have been studied extensively, and the clinical evidence is strong.
- In the pivotal STEP trials, patients taking semaglutide (the active ingredient in Wegovy) lost an average of approximately 15% of their body weight over 68 weeks when combined with diet and exercise, compared to about 2.4% with diet and exercise alone.
- In trials of tirzepatide (the active ingredient in Zepbound), patients lost an average of approximately 18–21% of body weight depending on the dose, compared to about 3% with placebo.
- For someone weighing 250 pounds, that translates to roughly 37 to 52 pounds of weight loss.
- The SELECT cardiovascular outcomes trial demonstrated that semaglutide reduced the risk of major adverse cardiovascular events by 20% in adults with established heart disease and overweight or obesity.
These aren't miracle drugs. They work best alongside real changes in nutrition and physical activity. Side effects — particularly gastrointestinal symptoms — are common, especially during dose titration, and not everyone responds the same way. But for people who have struggled with weight for years despite genuine effort, GLP-1 medications represent the most effective pharmacological tool available. The Bridge makes them accessible to Medicare beneficiaries at a price point that was unthinkable even a year ago.
Frequently Asked Questions
Is the Medicare GLP-1 Bridge Program real?
Yes. It was announced by CMS on December 23, 2025, with detailed FAQs published March 3, 2026. It runs from July 1 through December 31, 2026.
When does the Medicare GLP-1 Bridge start?
July 1, 2026. It ends December 31, 2026. There is no extension or grace period.
Does Medicare cover Ozempic through the Bridge?
No. Ozempic is FDA-approved for type 2 diabetes, not weight loss. Only Wegovy and Zepbound are covered under the Bridge. If you have diabetes, Ozempic may be covered through your regular Part D plan.
Does Medicare cover Mounjaro through the Bridge?
No. Mounjaro is approved for type 2 diabetes. Zepbound, which contains the same active ingredient (tirzepatide) but is approved for weight loss, is covered.
Does Medicare cover GLP-1 for prediabetes through the Bridge?
Yes — if you also have a BMI of 27 or higher. Prediabetes (per ADA guidelines) is a qualifying condition under Tier 3 of the Bridge eligibility criteria.
Does my Part D plan need to opt in for the Bridge?
No. The Bridge is administered by CMS through a central processor, entirely outside of Part D. Your plan does not need to opt in, and your plan is not directly involved in Bridge claims.
Does the $50 copay count toward my Part D out-of-pocket cap?
No. The Bridge operates outside Part D, so the $50 does not count toward your Part D deductible or your $2,100 annual out-of-pocket spending cap (TrOOP).
Can Extra Help reduce the $50 copay?
No. Low-Income Subsidy (Extra Help) cost-sharing does not apply to Bridge prescriptions. You'll pay the full $50 regardless of your LIS status.
Is the Wegovy pill (oral tablet) covered under the Bridge?
Yes. CMS has confirmed that Wegovy tablets are covered along with Wegovy injection and Zepbound injection.
I already use Wegovy for heart disease risk reduction through Part D. Can I switch to the Bridge?
No. If your GLP-1 is prescribed for a use that's coverable under Part D — even if your specific plan doesn't cover it — you cannot use the Bridge for that drug. You must use the Part D pathway.
What if my doctor already prescribes me Zepbound for sleep apnea?
You'll continue through your Part D plan. The Bridge only covers prescriptions written specifically for weight loss. CMS has stated they will monitor to ensure plans don't shift coverage from Part D to the Bridge.
Can my doctor appeal a Bridge prior authorization denial?
CMS has not yet released details on the appeal process. Additional guidance is expected in Spring 2026.
What happens if fewer than 80% of Part D plans join the BALANCE Model?
CMS has stated they will not launch BALANCE in Medicare for 2027 if participation falls below 80%. That could mean Bridge coverage in 2026 followed by no weight-loss GLP-1 coverage in 2027.
Can a telehealth provider help with the Medicare Bridge?
The Bridge requires a prescriber to submit prior authorization to CMS's central processor. Any licensed medical provider who can prescribe Wegovy or Zepbound can participate. Whether specific telehealth platforms will integrate with the central processor remains to be seen — CMS will release more details in Spring 2026.
I'm on Medicaid, not Medicare. Does this apply to me?
The Bridge is Medicare-only. Medicaid coverage for GLP-1 weight loss medications is expanding separately through the BALANCE Model, with participating states joining as early as May 2026. Contact your state Medicaid office for details.
Is this the same as Medicare drug price negotiation?
No. Medicare drug price negotiation (under the Inflation Reduction Act) is a separate program. Semaglutide was selected for negotiation in 2025, with negotiated prices taking effect in 2027. The Bridge is a CMS demonstration using different legal authority.
Our Sources and How We Keep This Updated
Every eligibility criterion, every cost figure, every program date on this page was verified against official CMS documentation. We don't rely on secondary reporting for core facts.
What we verified ourselves:
- The three distinct BMI/diagnosis eligibility tiers — and the fact that many other sites compress or misstate them
- That SNP, EGWP, and LI NET beneficiaries ARE eligible (contrary to at least one major competing article)
- That Part D plans do NOT need to opt in for the Bridge (contrary to at least two competing articles)
- The exact covered products: Wegovy injection, Wegovy oral tablet, and Zepbound only
- The $50 copay structure and its exclusion from Part D TrOOP and deductible calculations
- The BIN (028918) and PCN (MEDDGLP1BR) for pharmacy claims processing
- The net manufacturer price of $245 per monthly supply
- The July 1 – December 31, 2026 program dates
Primary sources:
- CMS Medicare GLP-1 Bridge FAQ page — last verified March 25, 2026
- CMS BALANCE Model overview
- CMS press release, December 23, 2025
- KFF analysis of the Bridge and BALANCE Model
- FDA compounding enforcement guidance
- STEP 1 extension study (semaglutide weight regain)
This page is updated whenever CMS releases new guidance about the Bridge or BALANCE Model. Key dates to watch: Spring 2026 (additional CMS details on prior authorization process), July 1, 2026 (Bridge launch), and October–December 2026 (BALANCE participation announcements and open enrollment decisions).
Still Not Sure Which GLP-1 Program Is Right for You?
The Medicare GLP-1 Bridge is a big deal — the first time in over 20 years that Medicare beneficiaries can access weight-loss medications at an affordable price. But it's not the only path, and it's not the right fit for everyone.
Whether you qualify for the Bridge, need to use regular Part D for a covered indication, want to plan for BALANCE in 2027, or need a telehealth option that starts today — the right program depends on your BMI, your health conditions, your budget, and your timeline.
Take our free 60-second matching quiz to find your personalized GLP-1 path
We'll ask you four quick questions and match you with the coverage pathway — or provider — that fits your exact situation. No commitment, no email required, and you'll have a clear next step in under a minute.
Take the free GLP-1 matching quiz →Related Guides
This guide is for informational purposes only and does not constitute medical advice. Always consult with your healthcare provider before starting any medication. The RX Index may receive compensation from providers mentioned on this page. This does not influence our coverage — we recommend based on program quality, pricing, and patient fit.
Last updated: March 25, 2026 · Verified against CMS.gov: March 25, 2026. Next scheduled review: when CMS releases Spring 2026 prior authorization guidance.