Sources checked against CMS.gov, FDA.gov, Medicare.gov, and Eli Lilly.
Does Medicare Cover Zepbound? Your Complete Coverage Guide
Published: · Last updated:
Medicare does not cover Zepbound (tirzepatide) for weight loss under ordinary Part D rules. That exclusion has been federal law since 2003. But the coverage picture changed dramatically in late 2025 and early 2026, and there are now 3 distinct Medicare coverage routes — each with different eligibility, different costs, and different timelines.
Your 3 Pathways to Zepbound on Medicare
| Pathway | Available When | Covers Weight Loss? | What You Pay | Who Qualifies |
|---|---|---|---|---|
| 1. OSA via Part D | Right now | No — covers sleep apnea only | Varies by plan; capped at $2,100/yr OOP | Adults with moderate-to-severe OSA + obesity, enrolled in Part D |
| 2. Medicare GLP-1 Bridge | Open now (through Dec 31, 2027) | Yes | $50/month | BMI ≥ 35; or BMI ≥ 30 with certain conditions; or BMI ≥ 27 with specific risk factors |
| 3. BALANCE Model | Postponed indefinitely (2028 at the earliest, if at all) | Yes | $50–$125/mo depending on plan type and phase | Must be enrolled in a participating Part D plan + meet clinical criteria |
| Self-pay fallback | Right now | N/A — no insurance used | $299–$449/month via LillyDirect | Anyone with a valid prescription |
Sources: CMS.gov (March 2026 Bridge FAQs), Eli Lilly, FDA.
Most pages covering this topic only explain one of these lanes — usually the sleep apnea pathway — and leave you guessing about the rest. We're going to walk through all three, explain exactly who qualifies, what you'll actually pay, and give you a clear next step no matter where you land.
Why Doesn't Medicare Cover Zepbound for Weight Loss?
Before we get into the pathways, it helps to understand why this is so confusing in the first place.
The Medicare Prescription Drug, Improvement, and Modernization Act of 2003 explicitly excludes “agents when used for anorexia, weight loss, or weight gain” from Part D coverage. That law was written years before GLP-1 medications like Zepbound existed as a treatment category. It has never been updated.
In 2024, CMS proposed reinterpreting this exclusion to allow Part D coverage for anti-obesity medications — a move that drew enormous interest, since roughly 20% of Medicare enrollees (about 14 million people) have an obesity diagnosis. But in April 2025, the administration decided not to move forward with that reinterpretation.
So the law hasn't changed. But the workarounds have arrived.
- December 2024: The FDA approved Zepbound for a non-weight-loss indication — moderate-to-severe obstructive sleep apnea in adults with obesity. That opened the first Medicare coverage lane.
- December 2025: CMS announced the Medicare GLP-1 Bridge and the BALANCE Model — covering Zepbound for weight loss through separate demonstration authorities that bypass the Part D exclusion entirely.
That's why you're finding contradictory information online. Some articles were written before December 2025. Some only cover the sleep apnea angle. Some still say the 2026 expansion was rejected — which is technically true for the Part D reinterpretation, but misses the Bridge and BALANCE programs entirely. We verified every claim on this page against the CMS GLP-1 Bridge FAQ (updated March 2026), the BALANCE Model documentation, and the current FDA label.
Pathway 1: Can Medicare Cover Zepbound for Sleep Apnea Right Now?
What the FDA Approved
In December 2024, the FDA approved Zepbound for the treatment of moderate-to-severe obstructive sleep apnea (OSA) in adults with obesity. It's the first and only prescription medication approved specifically for this use. Because this is a non-weight-loss indication, it sidesteps Medicare's weight loss drug exclusion entirely.
Who This Applies To
You may qualify if you meet all of the following:
- You have a confirmed diagnosis of moderate-to-severe OSA (typically from a sleep study/polysomnography)
- You have obesity (generally BMI ≥ 30)
- You're enrolled in Medicare Part D (standalone PDP or Medicare Advantage with drug coverage)
- Your specific plan lists Zepbound on its formulary for the OSA indication
- Your prescription is written specifically for OSA — not for weight loss

How to Get Covered Through This Pathway
- Confirm your OSA diagnosis. You'll need documentation of moderate-to-severe obstructive sleep apnea, usually from a sleep study. If you haven't had one, Medicare Part B covers diagnostic sleep tests when your doctor determines they're medically necessary.
- Check your plan's formulary. Not all Part D plans have added Zepbound for the OSA indication. Use the Medicare Plan Finder at Medicare.gov to search your specific plan's formulary. Look for Zepbound (tirzepatide) and check which indications are covered.
- Expect prior authorization. Nearly all plans require prior authorization for Zepbound. Your doctor will need to submit documentation including your sleep study results, BMI/obesity documentation, and a statement that Zepbound is being prescribed for OSA.
- Understand your costs. Your actual cost through Part D depends on your specific plan's formulary tier, pharmacy, and which coverage phase you're in. The 2026 Part D benchmarks: deductible of up to $615, and a covered-drug out-of-pocket cap of $2,100 — once you hit that, you pay $0 for the rest of the year. If you qualify for Extra Help (Low-Income Subsidy), copays for covered brand-name drugs are generally up to $12.65, and some beneficiaries pay less or $0.
What to Say When You Call Your Plan
What If Your Plan Doesn't Cover It for OSA?
- Request a formulary exception. Medicare allows you and your prescriber to ask for an exception when a needed drug isn't on the formulary. Your doctor will need to provide a supporting statement explaining why Zepbound is medically necessary for your OSA.
- Switch plans during enrollment. You can change plans during the Annual Enrollment Period (October 15 – December 7) or, for Medicare Advantage, during the Medicare Advantage Open Enrollment (January 1 – March 31).
- Check the Bridge program below. If you want Zepbound for weight management and also happen to have OSA, read Pathway 2 carefully — but know that CMS has made clear: if your use is coverable under ordinary Part D (like OSA), you go through your Part D plan, not the Bridge.
Free · 60 seconds · no signup
Pathway 2: The Medicare GLP-1 Bridge Program ($50/Month — Open Now Through 2027)
This is the biggest development in Medicare GLP-1 coverage. Every detail below is verified against the CMS GLP-1 Bridge FAQ page (updated March 2026).
What the Bridge Program Is
This is not a Part D benefit. It's a separate CMS-administered program that uses its own central claims processor. Your Part D plan doesn't have to opt in. CMS manages the whole thing directly. At $50/month, the Bridge eliminates more than 95% of Zepbound's $1,086 list price.
Do You Qualify? The Specific Eligibility Criteria
To qualify for the Medicare GLP-1 Bridge, you must meet all of these baseline requirements:
- Enrolled in an eligible Part D plan type for 2026 — CMS includes standalone PDPs and MA coordinated care plans with drug coverage (HMO, HMO-POS, local/regional PPO), plus SNPs, EGWPs, and LI NET; some other plan types are excluded unless you're also in a standalone PDP
- At least 18 years old
- Prescribed Zepbound to reduce excess body weight and maintain weight reduction
- Combined with ongoing structured nutrition and physical activity
AND you must fall into one of these three BMI categories:
| BMI Threshold | Additional Conditions Required |
|---|---|
| BMI 35 or higher | None — BMI alone qualifies |
| BMI 30–34.99 | Plus at least one: heart failure with preserved ejection fraction (HFpEF), uncontrolled hypertension (blood pressure above 140/90 on two or more medications), chronic kidney disease stage 3a or higher, prediabetes, a previous heart attack or stroke, OR symptomatic peripheral artery disease |
| BMI 27–29.99 | Plus at least one: prediabetes (per ADA guidelines), a previous heart attack or stroke, OR symptomatic peripheral artery disease |
Criteria are measured as of when you start GLP-1 therapy — including therapy started before the July 1 launch.
Who's excluded, even if the BMI criteria fit: You aren't eligible for the Bridge if you already get a GLP-1 covered through your Medicare Part D plan, or if you have type 2 diabetes, moderate-to-severe sleep apnea, or fatty liver disease. In those cases, your Part D plan may cover a GLP-1 instead — and CMS routes you there.
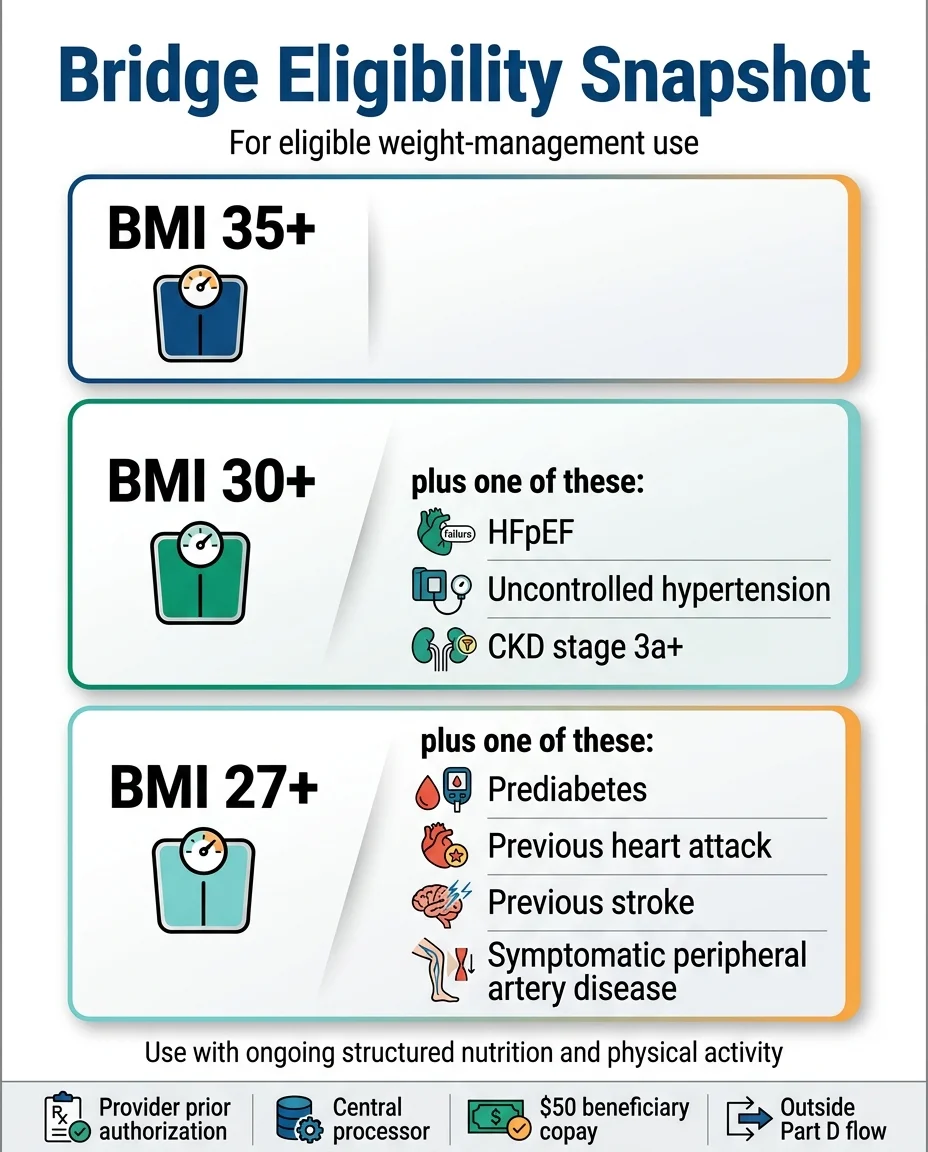
Your doctor submits a prior authorization request to CMS's central processor — not to your Part D plan — attesting that you meet these criteria.
5 Things Most People Don't Know About the Bridge
- The $50 does NOT count toward your Part D out-of-pocket cap. The Bridge operates entirely outside your Part D benefit. That means your $50/month payments don't reduce your $615 deductible and don't count toward your $2,100 annual cap. This is additional spending, separate from everything else. It won't appear on your Part D Explanation of Benefits, and you can't spread the $50 across months using the Medicare Prescription Payment Plan.
- Extra Help (Low-Income Subsidy) does NOT apply. Even if you qualify for Extra Help and pay little or nothing for other medications, you'll still owe the full $50/month under the Bridge. Over the full 18-month program, that's $900 — worth planning for.
- You can't transfer an existing Part D prescription to the Bridge to save money. If your doctor already prescribes Zepbound through your Part D plan for OSA, that prescription stays with your Part D plan. The clinical indication on your prescription determines which pathway applies. CMS goes further: having a Part D-coverable diagnosis — type 2 diabetes, moderate-to-severe OSA, or noncirrhotic MASH (fatty liver disease) — makes you ineligible for the Bridge outright, even if your BMI otherwise qualifies.
- Prior authorization goes to CMS, not your Part D plan. This is a different process than what you're used to. Your doctor sends the prescription to the pharmacy and, when requested, completes the prior authorization through the CMS central processor — not your insurance company. If approved, you'll get a letter in the mail, and the authorization stays valid through December 31, 2027 (including refills and dose changes) unless you switch GLP-1s.
- The Bridge runs 18 months. It runs July 1, 2026 through December 31, 2027. BALANCE will not launch for Medicare Part D in 2027 — CMS extended the Bridge instead. After December 2027, coverage will depend on whether BALANCE launches for Medicare Part D in 2028.
How to Start Now (the Bridge Is Open)
The Bridge is open. Here's the process, straight from Medicare.gov:
- Confirm you're enrolled in an eligible plan type. Standalone PDPs and MA coordinated care plans with drug coverage qualify, along with SNPs, EGWPs, and LI NET. If you're in Original Medicare with no drug coverage, you're not eligible.
- Confirm you're Bridge-eligible, not Part D-routed. If you have type 2 diabetes, moderate-to-severe sleep apnea, or fatty liver disease — or you already get a GLP-1 through your Part D plan — you're not eligible for the Bridge. Your Part D plan is the lane to check instead.
- Document your qualifying criteria with your doctor. BMI and health conditions are assessed as of when GLP-1 therapy starts — if you began therapy before July 1, eligibility can be based on your status at initiation. Gather lab results, blood pressure readings, A1c levels, and records of cardiac events.
- Make sure the prescription is for Zepbound KwikPen. The Bridge doesn't cover single-dose Zepbound vials or pens.
- Have your doctor send the prescription and complete the prior authorization. The pharmacy may ask for your Medicare Number or the last 4 digits of your Social Security number. Your provider certifies the medication is part of a lifestyle program focused on diet and exercise. Watch the mail for your approval letter — it stays valid through December 31, 2027 (including refills and dose changes) unless you change GLP-1s.
Free · 60 seconds · no signup
Pathway 3: The BALANCE Model — What Happens After the Bridge Ends
The Bridge is an 18-month program (July 2026–December 2027). The longer-term plan is the BALANCE Model (Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth), designed to provide ongoing Medicare Part D coverage of GLP-1 medications for weight management.
What BALANCE Is
BALANCE is a CMS Innovation Center payment model that allows Medicare Part D plans to cover GLP-1s (including Zepbound and Wegovy) for weight management — something they're normally prohibited from doing. Beneficiaries receiving GLP-1s for weight management under BALANCE will also have access to a manufacturer-provided lifestyle support program at no cost.
Start dates:
- Medicare Part D: BALANCE will not launch in 2027 — CMS confirmed on April 30, 2026 that the participation threshold was not met, postponed the Part D portion indefinitely, and extended the Bridge through December 2027 instead. CMS will use Bridge utilization data to decide whether BALANCE proceeds; 2028 is the earliest realistic start, and it is not guaranteed.
- Medicaid: launched May 2026 (state by state, scheduled to run through 2031)
Why 2027 Is Not Guaranteed
The Kaiser Family Foundation has flagged this transition risk as one of the program's biggest concerns. It's a structural risk of how these programs are designed, not a scare tactic.
What You Should Do About This
- Nothing this fall — that's the good news. Because the Bridge was extended through 2027 and runs outside Part D, you don't need to switch plans for 2027 to keep $50/month access.
- Watch fall 2027 instead. If CMS revives BALANCE for 2028, plan participation will matter during the October 15 – December 7, 2027 enrollment window.
- If BALANCE does return, weigh a plan switch against the impact on your other medications.
Free · 60 seconds · no signup
Cost-sharing under BALANCE varies by plan type and benefit phase: during the deductible phase, up to $245 plus a dispensing fee per fill; initial coverage phase, Enhanced Alternative and EGWP plans cap cost-sharing at $50, while other plans cap at $125; catastrophic phase, $0.
Eligibility for BALANCE
The eligibility criteria are broader than the Bridge. Under BALANCE, you may qualify if you have:
- Type 2 diabetes
- Noncirrhotic MASH (metabolic dysfunction-associated steatohepatitis) with moderate-to-advanced liver fibrosis (stages F2–F3)
- Obstructive sleep apnea
- Obesity with lifestyle modification and meeting BMI criteria similar to the Bridge
How to Actually Get Medicare to Cover Zepbound (Step by Step)
Understanding the pathways is one thing. Actually navigating the system is another. Here's a practical walkthrough that applies no matter which pathway you're pursuing.
Step 1: Get the Indication Right
This is where most people stumble before they even start. For ordinary Part D coverage, the only current indication that works is moderate-to-severe obstructive sleep apnea in adults with obesity. If your doctor writes a prescription that says “for weight loss” or “for obesity,” your Part D plan will deny it — and that's not the plan being difficult, it's federal law.
For the Bridge program (starting July 2026), the indication is explicitly weight management — so the prescription should reference weight reduction. But if your doctor is already prescribing Zepbound for OSA through your Part D plan, you can't switch that same prescription to the Bridge for a lower copay.
Step 2: Confirm Your Coverage Route
There are now two completely separate prior authorization tracks:
- For OSA coverage: Prior authorization goes to your Part D plan
- For Bridge program weight loss coverage: Prior authorization goes to CMS's central processor (a completely different system)
Step 3: Check Formulary and Utilization Rules
For the OSA pathway, your plan may have specific utilization management requirements:
- Prior authorization: Nearly universal for Zepbound. Your doctor submits documentation before the pharmacy can fill the prescription.
- Step therapy: Plans may require you to try a lower-cost formulary drug first before approving Zepbound.
- Quantity limits: Plans may limit the quantity dispensed per fill.
- Tier placement: Brand-name specialty drugs like Zepbound are often placed on higher tiers, meaning coinsurance rather than a flat copay.
Step 4: Help Your Doctor Build the Strongest Prior Authorization
Prior authorization requests get approved far more often when the documentation is thorough. Make sure your doctor includes:
- Your complete diagnosis with supporting evidence (sleep study results for OSA, recent lab work for Bridge-qualifying conditions)
- Your BMI with a recent date of measurement
- A clear statement of medical necessity explaining why you need Zepbound specifically
- What alternatives have been tried and why they were insufficient, ineffective, or contraindicated
- The exact FDA-approved indication being targeted
- Relevant clinical guidelines supporting the use of Zepbound for your condition
Step 5: Know What to Do When the First Answer Is No
A denial is a decision, not a dead end. Medicare gives you formal appeal rights, and many initial denials get overturned when proper documentation is submitted on the second try. Common fixable issues include incomplete paperwork and using the wrong indication on the prescription — both can be corrected and resubmitted. See the full denial section below.
Why Do Different Websites Say Different Things?
If you've been researching this topic for more than ten minutes, you've probably noticed that answers contradict each other. There are three reasons:
- Timing. Many articles were published before December 23, 2025 — the date CMS announced the Bridge and BALANCE programs. At least one major pharmacy information site still says CMS “decided against” expanding coverage in 2026, which was true for the Part D reinterpretation but completely misses the Bridge program.
- Confusing sleep apnea coverage with weight loss coverage. Some pages explain that Medicare covers Zepbound for OSA and then leave the impression that weight loss coverage is available too. It's not — not through ordinary Part D. The Bridge is a separate program with separate rules.
- Confusing the Bridge with Part D. The Bridge operates outside Part D. The $50 copay, the eligibility criteria, the prior authorization process, and the financial accounting are all separate. Pages that lump everything together create the wrong expectations.
How Much Does Zepbound Actually Cost on Medicare?
Here's every scenario in one place:
| Your Situation | Monthly Cost | Annual Cost | Counts Toward Part D Cap? | Key Detail |
|---|---|---|---|---|
| OSA via Part D (before OOP cap) | Varies — coinsurance on specialty tiers can be significant | Up to $2,100 (cap) | Yes | Deductible up to $615; plan covers 100% after $2,100 cap |
| OSA via Part D (after OOP cap) | $0 | Already capped at $2,100 | Yes | Plan covers 100% rest of year |
| OSA via Part D + Extra Help | Up to $12.65 for brand drugs | Varies by LIS category | Yes | If you qualify for Low-Income Subsidy |
| GLP-1 Bridge (July 2026–Dec 2027) | $50 | $900 (18 months) | No | Outside Part D — additional cost; LIS subsidies do NOT apply |
| BALANCE Model (2028 at the earliest, if it proceeds) | $50–$125 (varies by plan/phase) | Varies | Yes (within Part D) | Must be in a participating plan; $0 in catastrophic phase |
| LillyDirect self-pay | $299–$449 | $3,588–$5,388 | N/A | 2.5mg = $299; 5mg = $399; 7.5–15mg = $449 |
| Full retail (no discount) | ~$1,086 | ~$13,032 | N/A | Sticker price — almost nobody should pay this |
Prices verified July 3, 2026. Sources: CMS.gov, LillyDirect, Eli Lilly press releases, Medicare.gov.
Can Medicare Beneficiaries Use the Zepbound Savings Card?
There are two different Lilly programs, and the distinction matters:
- The commercial insurance savings card (which reduces cost to as low as $25/month for commercially insured patients) excludes government insurance beneficiaries — including Medicare, Medicaid, TRICARE, and VA. If you have Medicare, this card won't work at the pharmacy.
- The self-pay program through LillyDirect is a separate pathway — a cash-pay option available to anyone with a prescription, including Medicare beneficiaries who are paying out of pocket. This is how you access the $299–$449/month pricing described above.
The Honest Admission: What This Page Can't Do
We can tell you the rules. We can map out every pathway. We can show you the eligibility criteria and cost numbers. But we cannot tell you that getting Zepbound on Medicare is simple, because it isn't.
The system is genuinely confusing. Prior authorizations get denied. Formularies change. The Bridge just launched and some operational kinks are still being worked out. The BALANCE Model didn't hit its participation threshold and is postponed indefinitely. The people who successfully get Zepbound through Medicare are the ones who know which lane they're in, have their documentation ready, use the right language with their plan, and have a backup if the first attempt doesn't work. That's what the rest of this page is designed to help you do.
What If Medicare Denies Coverage for Zepbound?
Denials happen — and they're not the end of the road. A denial is a decision that can be appealed, and many initial denials result from incomplete documentation rather than a fundamental eligibility problem. The difference between approval and denial often comes down to how thoroughly the paperwork was prepared.
Understanding Why You Were Denied
Before you do anything else, find out the specific reason for the denial. Common denial reasons include:
- Wrong indication on the prescription. If it says “weight loss” instead of “obstructive sleep apnea,” Part D coverage won't happen under current rules. This is the single most common fixable error.
- Incomplete documentation. Missing sleep study results, no recent BMI on file, or a vague medical necessity letter.
- Plan formulary exclusion. Zepbound isn't on your specific plan's formulary for the indication being requested. This doesn't mean it can't be covered — it means you need a formulary exception.
- Step therapy requirement not met. Your plan may require you to try a lower-cost covered drug first. If you've already tried required medications, make sure that's documented.
- Prior authorization not submitted properly. Wrong form, missing signature, sent to the wrong fax number.
Your Formal Appeal Rights
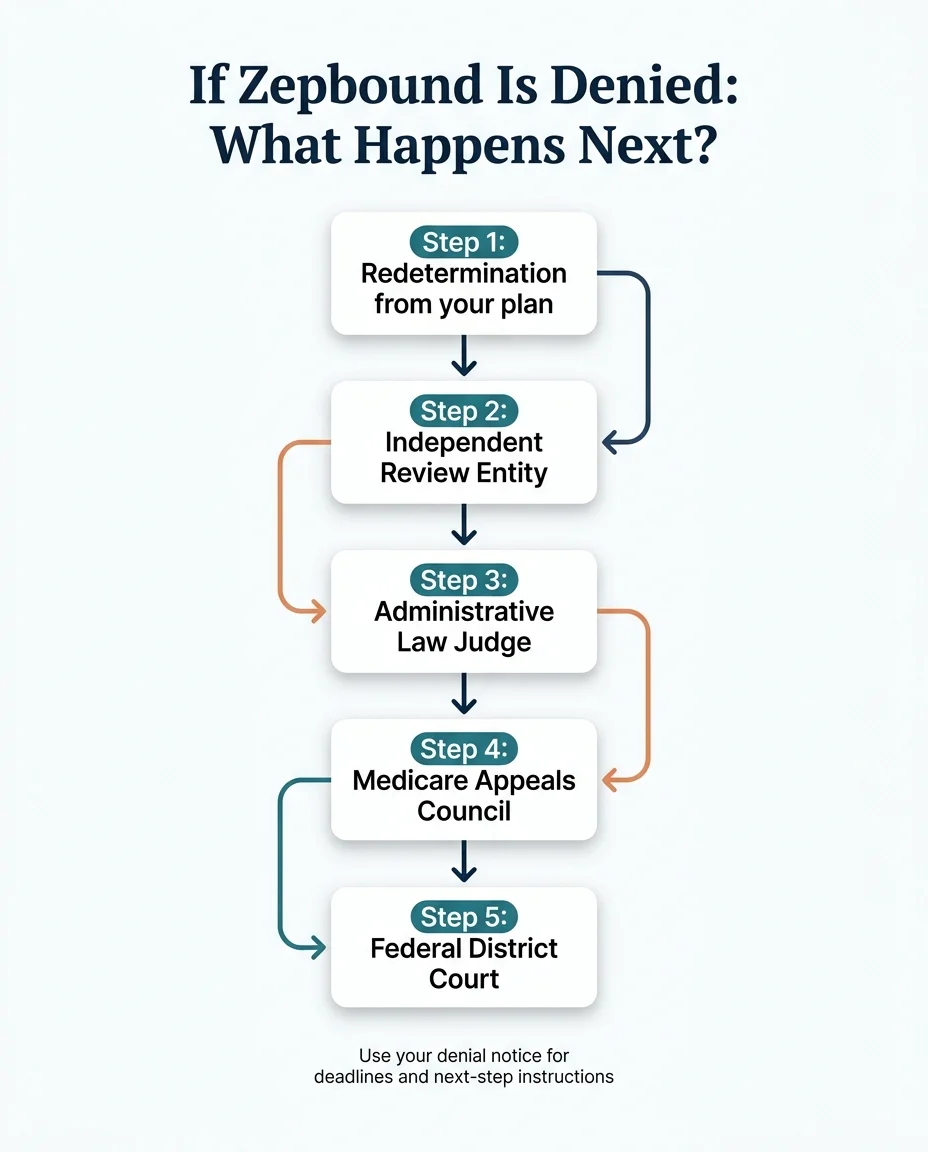
Level 1 — Redetermination by Your Plan
Your plan re-reviews the decision, ideally with additional documentation from your doctor. Timeline: up to 7 calendar days for a standard benefit request, or 72 hours for an expedited request (available if waiting could seriously harm your health).
Level 2 — Independent Review Entity (IRE)
If your plan upholds the denial, it automatically goes to an independent reviewer outside your insurance company. A fresh set of eyes that doesn't work for your plan.
Level 3 — Administrative Law Judge (ALJ) Hearing
If the amount in controversy meets the 2026 threshold ($200), you can request a formal hearing before an administrative law judge.
Level 4 — Medicare Appeals Council
A further level of review if you disagree with the ALJ's decision.
Level 5 — Federal District Court
Final formal appeal route available if the amount meets the threshold.
What Makes a Strong Appeal Package
- A detailed letter from your prescribing physician explaining exactly why Zepbound is medically necessary for your specific situation
- Complete diagnosis documentation — sleep study results, lab work, imaging
- Your BMI with a recent date of measurement
- A clear explanation of what alternatives have been tried and why they didn't work
- The specific FDA-approved indication for which Zepbound is being prescribed
- Any relevant clinical guidelines or medical literature supporting the use
- A direct response to the reason given for the denial
You Can Also Request a Formulary Exception
This is different from an appeal. A formulary exception asks the plan to cover a drug that isn't normally on their formulary. Your doctor must provide a written medical justification explaining why the formulary alternatives won't work for you specifically. Plans are required by Medicare to have an exception process. The worst they can say is no — and even then, you have the appeal rights described above.
Free · 60 seconds · no signup
Key Dates: Your Medicare Zepbound Timeline
There's a lot happening in a short window. Here are the dates that matter:
| Date | What Happens | What You Should Do |
|---|---|---|
| Now | OSA pathway available through Part D | Check your plan's formulary; submit prior authorization if you have OSA |
| March 2026 | CMS released the Bridge FAQs and prior authorization details | Done — see the CMS Bridge FAQ |
| April 30, 2026 | BALANCE Part D launch postponed indefinitely; Bridge extended through December 31, 2027 | No plan switch needed for 2027 |
| July 1, 2026 ★ | Medicare GLP-1 Bridge opened — live now | Have your doctor submit the prescription and prior authorization |
| Throughout 2027 | Bridge continues at $50/month for Zepbound KwikPen, Wegovy, and Foundayo | Monitor CMS announcements on whether BALANCE will proceed |
| Oct 15 – Dec 7, 2027 | Annual Enrollment Period | If CMS revives BALANCE for 2028, plan participation will matter here |
| December 31, 2027 | Medicare GLP-1 Bridge ends (unless further extended) | Have a 2028 plan — BALANCE (if it proceeds), self-pay, or another pathway |
| January 1, 2028 (potential) | BALANCE may launch for Part D — not guaranteed; CMS will decide using Bridge data | Watch fall-2027 announcements |
The enrollment window in October–December 2027 will be particularly important — that's when you'll need to make sure your 2028 plan participates in BALANCE (if CMS runs a new participation round).
Does Medicare Cover Zepbound for These Specific Conditions?
These are the most common condition-specific searches we see. Here's a direct answer for each one.
Does Medicare Cover Zepbound for Sleep Apnea?
Yes — this is the one condition where ordinary Medicare Part D may cover Zepbound right now, when prescribed for moderate-to-severe OSA in adults with obesity. See Pathway 1 above for full details.
Does Medicare Cover Zepbound for Weight Loss?
Not under regular Part D. The federal weight loss drug exclusion still applies. However, the Medicare GLP-1 Bridge ($50/month, open now through December 2027, Zepbound KwikPen only) covers Zepbound for weight management. BALANCE has been postponed indefinitely for Part D — the Bridge is the path through the end of 2027. See Pathways 2 and 3 above.
Does Medicare Cover Zepbound for Obesity?
Same answer as weight loss. Under ordinary Part D, obesity alone doesn't create a coverage pathway for Zepbound. But under the Bridge program, obesity is a qualifying condition — with specific BMI thresholds (≥ 35, or ≥ 30 with comorbidities, or ≥ 27 with specific risk factors).
Does Medicare Cover Zepbound for Diabetes?
No — and here's a common point of confusion. Zepbound is not FDA-approved for type 2 diabetes. The diabetes version of tirzepatide is called Mounjaro. Mounjaro is approved for type 2 diabetes and is covered by most Part D plans for that use. If you have type 2 diabetes and want the benefits of tirzepatide, ask your doctor about Mounjaro. It uses the same molecule at the same doses. Your Part D plan is far more likely to cover it.
Does Medicare Cover Zepbound for Heart Disease?
Not directly. Zepbound doesn't have an FDA-approved cardiovascular indication. (Wegovy does — it's approved to reduce major adverse cardiovascular events in adults with established cardiovascular disease who are obese or overweight, and Part D may cover Wegovy for that use.) However, for the Bridge program, a prior heart attack or prior stroke qualifies you for the lowest BMI threshold (≥ 27).
Does Medicare Cover Zepbound for High Blood Pressure?
Not directly under Part D. But uncontrolled hypertension — systolic blood pressure above 140 mmHg or diastolic above 90 mmHg while on two or more blood pressure medications — is a qualifying comorbidity for the Bridge program at BMI ≥ 30.
Does Medicare Cover Zepbound for Prediabetes?
Not under ordinary Part D. But pre-diabetes (per American Diabetes Association guidelines) qualifies you for the Bridge program at the lowest BMI threshold (≥ 27).
Does Medicare Cover Zepbound for Fatty Liver Disease?
Not through the Bridge — and there's a wrinkle. Per Medicare.gov, people with fatty liver disease aren't eligible for the Bridge at all, because a GLP-1 for that diagnosis may be coverable under ordinary Part D. The catch: Zepbound doesn't have an FDA-approved MASH indication — Wegovy does. So if noncirrhotic MASH is your diagnosis, the practical next step is a Part D formulary and indication check with your prescriber, likely for Wegovy rather than Zepbound. If BALANCE eventually launches for Part D (2028 at the earliest), MASH with moderate-to-advanced fibrosis (F2–F3) is on its eligibility list.
Does Medicare Cover Zepbound for Seniors?
"Seniors" isn't a clinical indication — but we understand the question. Most Medicare beneficiaries are 65+, and the answer doesn't change based on age. What matters is your diagnosis, BMI, and which pathway you're pursuing.
Medicare Part D vs. Medicare Advantage: Which Covers Zepbound?
- Original Medicare + Standalone Part D (PDP): This is the standard route. Part D covers outpatient prescription drugs including Zepbound (when the indication qualifies). Check your plan's formulary at Medicare.gov.
- Medicare Advantage with Drug Coverage (MA-PD): MA plans that include Part D drug coverage follow the same federal exclusion for weight loss drugs. They can cover Zepbound for OSA if it's on their formulary. MA-PD enrollees are also eligible for the GLP-1 Bridge program.
- Medicare Advantage Without Drug Coverage: If your MA plan doesn't include prescription drug benefits, it won't cover Zepbound at all.
- Part B: Generally no. Part B typically covers drugs that aren't self-administered — think infusions at a doctor's office. Zepbound is a self-administered injection (you give it to yourself at home), so the practical Medicare route is Part D, not Part B.
- The Bridge is administered by CMS, not your Part D plan. You need to be enrolled in an eligible Part D plan type — CMS includes standalone PDPs and MA coordinated care plans with drug coverage, plus SNPs, EGWPs, and LI NET — and meet the clinical criteria.
What If You Don't Qualify for the Bridge? Options Available Right Now
Pathway 1 requires a sleep apnea diagnosis. Pathway 2 is open now — but not everyone qualifies, approval isn't instant, and it only covers the KwikPen. Pathway 3 is postponed indefinitely. And here's the group almost nobody writes for: if your BMI is between 27 and 34.9 without one of the qualifying conditions — or under 27 — there is currently no Medicare pathway for you at all. If that's you, or you're waiting on a prior authorization decision, or your plan type is excluded, here's what's actually available today.
Self-Pay Through LillyDirect
Eli Lilly sells Zepbound directly to patients through its LillyDirect platform. No insurance required. Pricing as of March 2026:
- 2.5 mg (starter dose): $299/month
- 5 mg: $399/month
- 7.5 mg through 15 mg (maintenance doses): $449/month
These are for single-dose vials and the newer multi-dose KwikPen (launched February 2026). Both require a prescription from a licensed provider. To maintain the $449 maintenance dose pricing, you need to refill within 45 days of your previous delivery.
The Self-Pay Bridge Math
Here's what this looked like in real dollars for someone who started self-pay in April and moved to the Bridge when it opened in July:
| Month | Source | Cost |
|---|---|---|
| April | LillyDirect (starter dose) | $299 |
| May | LillyDirect | $399 |
| June | LillyDirect | $449 |
| July | Bridge program | $50 |
| August | Bridge program | $50 |
| September | Bridge program | $50 |
| October | Bridge program | $50 |
| November | Bridge program | $50 |
| December | Bridge program | $50 |
| Total (9 months) | $1,447 | |
Compare that to $1,086/month at full retail ($9,774 over the same period). The math often makes more sense than people expect — especially when weighed against the downstream health costs of untreated obesity: higher blood pressure medications, sleep apnea equipment, joint replacements, diabetes management.
Starting today, the math is simpler: self-pay only has to cover the gap between your first fill and your Bridge approval — then you're at $50/month through December 2027. And an underrated detail: Medicare assesses the clinical criteria as of when you start GLP-1 therapy, including therapy started before July 1. Beginning on self-pay now doesn't disqualify you from the Bridge later.
Telehealth Providers Who Prescribe Zepbound
If your primary care doctor doesn't prescribe GLP-1 medications, or if you want a streamlined process, telehealth platforms can help. Ro is one option that prescribes FDA-approved Zepbound with medical oversight, licensed providers, and pharmacy fulfillment.
What makes Ro particularly relevant for Medicare beneficiaries: they prescribe the actual FDA-approved product — not a compounded version — which means if you start through Ro and later qualify for the Bridge or a BALANCE-participating plan, you're already established on the same medication. That can make the transition smoother when coverage kicks in.
| If this is you | Best self-pay route |
|---|---|
| You already have a prescriber and want the lowest total monthly cost | LillyDirect |
| You need a prescriber, or want clinical support managing doses and side effects | Ro (sponsored affiliate link, opens in a new tab)(sponsored) |
FDA-Approved Zepbound — Start Today
Check current Ro pricing and eligibility
FDA-approved Zepbound with licensed physician oversight and home delivery. Medicare members can pay cash, separate from their Medicare benefit. Ro walks you through your options before you commit to anything. Medicare assesses Bridge eligibility as of when you started therapy — starting now doesn't cost you the $50 pathway later.
Check eligibility on Ro → (sponsored affiliate link, opens in a new tab)Cash-pay path only. Ro cannot coordinate GLP-1 coverage for government insurance plans. Costs do not count toward your Medicare Part D benefit.
A Note on Compounded Tirzepatide
Some online providers offer compounded tirzepatide at lower prices. We want to be direct about this:
- Compounded medications are not FDA-approved
- They are not the same product as brand-name Zepbound
- They will not be covered under any Medicare pathway — not Part D, not the Bridge, not BALANCE
- The FDA has issued warnings about certain compounded GLP-1 marketing practices
For Medicare beneficiaries specifically, brand-name Zepbound positions you to take advantage of the Bridge and BALANCE programs when they become available. Compounded tirzepatide does not.
What Other Medicare-Covered Options Exist?
If Zepbound isn't an option right now, Medicare does cover several weight-management related services available today:

- Sleep studies: Medicare Part B covers diagnostic sleep tests when your doctor determines they're clinically indicated. If you suspect you have sleep apnea, this is the first step toward the OSA coverage pathway for Zepbound.
- CPAP therapy: Medicare may cover a 12-week CPAP trial if you're diagnosed with obstructive sleep apnea and meet the coverage conditions.
- Obesity behavioral counseling: Medicare Part B covers intensive behavioral therapy for obesity (BMI ≥ 30) when provided in a primary care setting. This is counseling — not medication — but it's covered and can complement your weight management plan.
- Bariatric surgery: For qualifying patients, Medicare covers certain bariatric procedures including gastric bypass and sleeve gastrectomy.
None of these replace the effectiveness of GLP-1 medications for many patients. But they're covered, available now, and can be part of a comprehensive approach — especially while you work through a prior authorization, or if you don't qualify for the Bridge. See also our complete guide on Medicare coverage for Wegovy.
Your Action Plan: What to Do Based on Your Situation
Pathway 1 — Available Now
If You Have Sleep Apnea and Obesity
Your next step is Pathway 1. Call your Part D plan today and ask if Zepbound is on the formulary for the OSA indication. If yes, have your doctor submit a prior authorization. If no, request a formulary exception. This coverage is available right now.
Pathway 2 — Open Now
If You Want Zepbound for Weight Loss and Meet Bridge Criteria
Your next step is to apply. Confirm your Part D enrollment, document your BMI and qualifying conditions with your doctor, and have them submit the prescription and prior authorization now — the program runs through December 31, 2027. If you want to start before your approval arrives, self-pay through LillyDirect or Ro (sponsored affiliate link, opens in a new tab) (sponsored) ($299–$449/month for the medication) keeps you on the same FDA-approved product in the meantime.
Self-Pay — Fastest Path
If You Want Zepbound Now and Can Manage $299–$449/Month
Your fastest path is LillyDirect or a telehealth provider like Ro (sponsored affiliate link, opens in a new tab) (sponsored). Get a prescription, start treatment, and transition to the Bridge at $50/month if you qualify — it's open now, and Medicare assesses eligibility based on when you started therapy.
Financial Assistance
If Budget Is a Major Concern
Check Lilly's current assistance programs first — call 1-800-545-6962 and ask what financial assistance is available for Zepbound. If you can manage $50/month, the Bridge program — open now at $50/month — may be your best bet. Also talk to your doctor about whether Mounjaro (same ingredient, diabetes indication) might be covered under your Part D plan if you have type 2 diabetes.
Appeal — Don't Give Up
If You Were Denied and Don't Know What to Do
File an appeal or formulary exception. Find out the specific reason for the denial and address it directly. Many denials can be overturned with proper documentation. See the denial section above for the step-by-step process.
Not Sure Where You Fall?
Take our free 60-second quiz. We'll match you to the right pathway — OSA coverage, Bridge eligibility, self-pay, or appeal strategy — based on your specific Medicare situation, health conditions, and budget. No email required to see your results.
Find My Zepbound Coverage Path →How We Verified This Page
Trust matters on a topic like this, so here's exactly how we built and maintain this page:
- CMS GLP-1 Bridge FAQ page (cms.gov) — Bridge dates, eligibility criteria, $50 copay, plan-type eligibility, TrOOP exclusion, central processor details, and the rule that Bridge cannot be used for indications coverable under basic Part D
- Medicare.gov GLP-1 Bridge enrollee page (medicare.gov/glp1bridge) — beneficiary eligibility checklist, plan type eligibility, step-by-step prior authorization process, and the six qualifying conditions verified July 3, 2026
- CMS BALANCE Model (cms.gov) — 2027 timeline, cost-sharing by plan type and benefit phase, participation threshold, KwikPen formulation detail, lifestyle support program requirements, and eligibility criteria
- Medicare.gov Part D costs — 2026 Part D deductible cap ($615) and covered-drug out-of-pocket cap ($2,100)
- Medicare.gov Extra Help — 2026 LIS cost-sharing amounts by category
- Zepbound savings and pricing (zepbound.lilly.com) — commercial savings card exclusions, self-pay program terms, and LillyDirect pricing
- Medicare appeals (medicare.gov) — appeal levels, timelines, expedited review criteria
- FDA Zepbound label (accessdata.fda.gov) — approved indications (chronic weight management and moderate-to-severe OSA in adults with obesity)
We review this page against CMS sources at least monthly, and immediately when CMS, FDA, or Eli Lilly announce policy or pricing changes. The “Last Verified” date at the top reflects our most recent full review.
What we do NOT claim: We don't maintain a database of every Part D plan's Zepbound formulary status by ZIP code. Plans change their formularies, and the only authoritative source for your specific plan's coverage is the plan itself or the Medicare Plan Finder tool.
Frequently Asked Questions
Does Medicare Part B cover Zepbound?
Generally no. Part B typically covers drugs administered by a healthcare provider (like infusions). Zepbound is self-administered at home, so the standard Medicare route is Part D or Medicare Advantage with drug coverage, not Part B.
Does Medicare Advantage cover Zepbound?
It can — if your MA plan includes Part D drug coverage and Zepbound is on the formulary for a covered indication (currently OSA). MA-PD enrollees in coordinated care plans are also eligible for the GLP-1 Bridge, which is open now. The federal weight loss drug exclusion applies to MA plans the same way it applies to standalone Part D.
Does Wellcare, Humana, UnitedHealthcare, or Aetna cover Zepbound?
Coverage depends on your specific plan and the indication, not just the insurer. Two plans from the same carrier in different states can have different formularies. Check your plan directly at Medicare.gov or call the number on your Medicare card.
Can I use the Zepbound Savings Card with Medicare?
The commercial insurance savings card does not work with Medicare or other government insurance. However, Lilly's separate self-pay program through LillyDirect is available to Medicare beneficiaries paying cash — that's a different program with pricing of $299–$449/month depending on dose. See current self-pay options and pricing above →
Does the $50 Bridge copay count toward my Part D out-of-pocket cap?
No. The Bridge operates outside the Part D benefit. Your $50 monthly copay doesn't count toward the $615 deductible or the $2,100 annual cap. This is additional spending, separate from everything else.
What if my plan says Zepbound isn't on the formulary?
You can request a formulary exception. Your doctor must provide a supporting statement explaining why Zepbound is medically necessary and why formulary alternatives won't work. You can also switch plans during enrollment periods.
What if I have OSA but my doctor wrote the prescription for weight loss?
The indication on the prescription matters for coverage purposes. If your goal is to use the OSA pathway through Part D, make sure the prescription specifies the OSA indication. If you'd prefer the weight loss pathway, the Bridge program opens July 1 — but if your use is coverable under Part D (like OSA), CMS says you go through your Part D plan, not the Bridge.
Is Zepbound 'approved by Medicare'?
This is an important distinction. The FDA approves drugs. Medicare plans decide coverage within Medicare rules. Zepbound has FDA approval for weight management and OSA. Whether Medicare covers it depends on which pathway applies to you. 'Approved by Medicare' isn't really the right framing.
Will Medicare cover Zepbound in 2027?
Not through BALANCE. CMS confirmed the 80% participation threshold for Medicare Part D was not met, so BALANCE will not launch for Medicare Part D in 2027. However, the Medicare GLP-1 Bridge has been extended through December 31, 2027, giving eligible beneficiaries continued access to Zepbound KwikPen (and Wegovy and Foundayo) at $50/month through the Bridge.
What's the difference between Zepbound and Mounjaro?
Same active ingredient (tirzepatide), same doses, different FDA approvals. Mounjaro is for type 2 diabetes. Zepbound is for weight management and sleep apnea. If you have diabetes, Mounjaro is often the easier Medicare path because it doesn't face the weight loss drug exclusion.
Does Medicaid cover Zepbound?
Coverage varies by state and is changing. The BALANCE Model opens to state Medicaid agencies as early as May 2026. Check with your state Medicaid office for the most current status.
Is compounded tirzepatide covered by Medicare?
No. Medicare does not cover compounded medications for weight loss. Compounded tirzepatide is not FDA-approved, not substitutable for Zepbound, and not eligible for any Medicare coverage pathway. Tirzepatide is no longer on the FDA shortage list, which further narrows the legal basis for 503A patient-specific compounding.
How do I apply for the Medicare GLP-1 Bridge?
There's no application form for you to fill out. Your doctor sends a prescription for a covered GLP-1 (Zepbound KwikPen, Wegovy, or Foundayo) to the pharmacy and, when requested, completes a prior authorization through the CMS central processor — not your Part D plan. Your provider certifies that you meet the clinical criteria and that the medication is part of a lifestyle program focused on diet and exercise. The pharmacy may ask for your Medicare Number or the last 4 digits of your Social Security number, and you'll pay the $50 copay for a one-month supply (28 or 30 days, depending on the drug). If approved, you'll get a letter in the mail, and your prior authorization stays valid through December 31, 2027 — including refills and dose changes — unless you switch to a different GLP-1. Check eligibility at Medicare.gov/glp1bridge or call 1-800-MEDICARE.
I have sleep apnea AND meet the BMI criteria — can I pick the $50 Bridge instead of Part D?
No. CMS is explicit about this: beneficiaries whose diagnosis is coverable under Part D — type 2 diabetes, moderate-to-severe OSA, or noncirrhotic MASH (fatty liver disease) — are ineligible for the Bridge even if they otherwise meet the BMI criteria. If you have one of those diagnoses, your route is your Part D plan (see Pathway 1). The same goes if you already get a GLP-1 covered through your Part D plan.
The Bottom Line
Medicare's relationship with Zepbound is complicated — but it's no longer a dead end.
If you have sleep apnea, coverage may be available right now through your Part D plan. If you want it for weight management, the $50/month Bridge program is open right now and runs through December 31, 2027. What happens in 2028 depends on whether CMS moves forward with the BALANCE Model — it's postponed indefinitely, and CMS will use Bridge data to decide.
None of these pathways are automatic. They all require documentation, the right indication, and often a prior authorization. But the paths exist — and knowing which one applies to your situation is more than half the battle.
Still not sure which GLP-1 program is right for you?
Or if you're ready to start on self-pay today:
Start Now — FDA-Approved Zepbound
Check eligibility on Ro for FDA-approved Zepbound
Licensed physicians, home delivery, no Medicare coordination required. The Bridge is open — but if you don't qualify, your plan type is excluded, or you're waiting on a prior authorization decision, this is the fastest way to start on brand-name Zepbound. If Bridge coverage comes through later, you're already established on the same medication.
Check eligibility on Ro → (sponsored affiliate link, opens in a new tab)Self-pay path only. Ro does not coordinate GLP-1 coverage for government insurance plans.
Related Guides
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice. Zepbound (tirzepatide) is a prescription medication. Consult your healthcare provider before starting any medication. Coverage information is based on current federal rules and may change as CMS releases additional guidance.
About The RX Index: We're an independent research team covering GLP-1 medication access, pricing, and insurance coverage. We believe everyone deserves clear, accurate information about their treatment options — especially when the system makes it hard to find.
Sources verified against CMS.gov, FDA.gov, Medicare.gov, Eli Lilly, and Kaiser Family Foundation. Last updated: July 3, 2026. Next scheduled review: October 2026.