CMS BALANCE Model GLP-1: Who Qualifies, What It Costs, and What Happens Next
The CMS BALANCE Model GLP-1 program is CMS's two-step effort to expand access to GLP-1 medications for obesity under Medicaid and Medicare Part D. Medicare has long been prohibited by law from covering drugs when used specifically for weight loss, while state Medicaid coverage of obesity drugs has remained optional. If you have been paying $1,000+ a month out of pocket for Wegovy or Zepbound, or if you gave up entirely because the price was out of reach — this program is what you have been waiting for.
The $50 copay does not count toward your Part D deductible or out-of-pocket cap. Low-income subsidies do not apply during the Bridge. The Bridge only lasts six months. And whether you keep access in 2027 depends entirely on whether your specific Part D plan volunteers to participate in BALANCE.
We built this page to be the only resource you need. Everything below — eligibility, cost, timelines, risks, and your options if you cannot wait or do not qualify — comes directly from official CMS guidance and verified policy analysis.
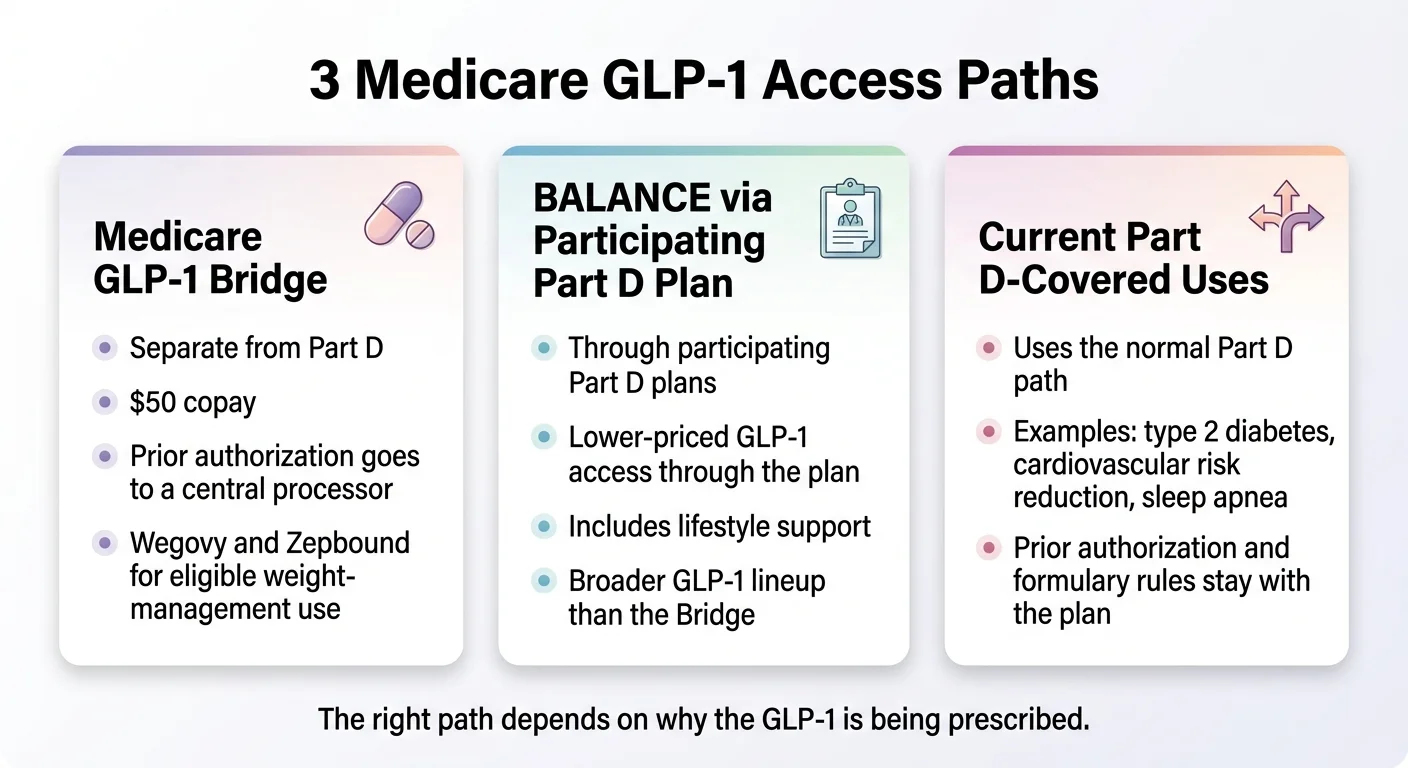
At a Glance: Your Three Paths to Medicare GLP-1 Coverage
There are actually three different pathways to GLP-1 coverage under Medicare right now, and most pages on the internet blur them together. That is why people are confused.
| GLP-1 Bridge (2026) | BALANCE — Part D (2027) | Current Part D (Now) | |
|---|---|---|---|
| When it starts | July 1, 2026 | January 1, 2027 | Already available |
| When it ends | December 31, 2026 | December 2031 | Ongoing |
| Which drugs | Wegovy (injection + tablets), Zepbound | Mounjaro, Ozempic, Rybelsus, Wegovy, Zepbound KwikPen, possibly orforglipron | Varies by plan formulary |
| Covers weight-loss GLP-1s? | ✅ Yes | ✅ Yes (broader drug list) | ❌ No (prohibited by law) |
| Your cost | $50/month flat | $50–$125/month (varies by plan type) | Varies (deductible + coinsurance) |
| Counts toward deductible? | ❌ No | ✅ Yes | ✅ Yes |
| Counts toward $2,100 OOP cap? | ❌ No | ✅ Yes | ✅ Yes |
| Plan must opt in? | ❌ No — CMS runs it directly | ✅ Yes (voluntary) | N/A |
| Prior auth goes to | CMS central processor | Your Part D plan | Your Part D plan |
| Low-Income Subsidy applies? | ❌ No | ✅ Yes | ✅ Yes |
What Is the CMS BALANCE Model GLP-1 Program?
The BALANCE Model — it stands for Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth — is a voluntary CMS Innovation Center program designed to test whether expanding access to GLP-1 medications for weight management, paired with lifestyle support, can improve health outcomes for Medicare and Medicaid beneficiaries while controlling costs.
In plain English: CMS is using two legal authorities to create new coverage pathways. The 2026 Medicare GLP-1 Bridge is a separate Section 402 demonstration. BALANCE itself is an Innovation Center model under section 1115A of the Social Security Act. Together, they create a path for Medicare and Medicaid to cover GLP-1 medications for weight loss — a use that has been prohibited since 2003.
Why This Exists
For over two decades, Medicare has been prohibited by law from covering medications when prescribed solely for weight loss. That prohibition was written in 2003, long before GLP-1 medications demonstrated the kind of results that are now reshaping how physicians treat obesity — significant weight reduction, improved cardiovascular markers, better blood sugar control, and improvements across conditions like sleep apnea and kidney disease.
Meanwhile, the cost of GLP-1 medications has put them out of reach for most people without insurance coverage. Wegovy carries a list price around $1,350 per month. Zepbound runs approximately $1,086. For the millions of Medicare and Medicaid beneficiaries living with obesity, those prices made access essentially impossible without separate coverage for a non-weight-loss indication.
The BALANCE Model is CMS's effort to close that gap.
Medicare GLP-1 Bridge vs. BALANCE Model: The Difference That Matters Most
This is where most people get lost. They see a headline that says “Medicare covering GLP-1s at $50 per month” and assume it is one program. It is actually two different programs with different rules, different timelines, and different implications for your coverage.
The Medicare GLP-1 Bridge (July – December 2026)
The Bridge is a temporary, six-month demonstration that gives eligible Medicare Part D beneficiaries early access to Wegovy and Zepbound for weight loss at a $50 per month copay. It was designed as a stopgap — a way to get medications to beneficiaries before the full BALANCE Model is ready for Medicare Part D.
- Runs from July 1 through December 31, 2026
- Operates outside of the Part D benefit — completely separate from your normal drug coverage
- Your Part D plan does not need to opt in. CMS administers the Bridge directly through a central claims processor
- Only Wegovy (injection and tablets) and Zepbound are available through the Bridge
- Your doctor submits prior authorization to CMS's central processor, not to your insurance company
- You pay $50 per month at the pharmacy — CMS handles the rest
The BALANCE Model for Medicare Part D (Starting January 2027)
BALANCE is the longer-term program. Starting January 1, 2027, participating Medicare Part D plans can cover GLP-1 medications for weight management as part of the standard Part D benefit.
- Runs from January 1, 2027 through December 2031
- Your Part D plan must volunteer to participate. Not all plans will.
- Drug list is broader: Mounjaro, Ozempic, Rybelsus, Wegovy, Zepbound (KwikPen), and potentially orforglipron if it receives FDA approval
- Prior authorization goes through your Part D plan's normal process
- Cost-sharing varies by plan type (more on this below)
- Includes a mandatory lifestyle support program provided free by the drug manufacturer
Medicare GLP-1 Coverage 2026: What Actually Starts in July?
Starting July 1, 2026, the Medicare GLP-1 Bridge goes live nationwide. Every state. Every territory. If you are enrolled in a qualifying Part D plan and you meet the clinical criteria, you are eligible — regardless of whether your specific insurance company has done anything.
Here is how it works in practice:
You and your doctor decide a GLP-1 for weight management is appropriate
Your doctor submits a prior authorization request to the CMS central processor — not to your plan
If approved, you go to your pharmacy with the prescription
You pay $50. The pharmacy collects your copay and submits a claim to the central processor.
The central processor reimburses the pharmacy at the drug's wholesale acquisition cost, minus your $50 copay, plus a dispensing fee and any applicable sales tax
Do You Qualify? Medicare GLP-1 Bridge Eligibility Criteria
Based on the CMS Bridge FAQ released in March 2026, here are the eligibility requirements translated into plain language.
The Quick Checklist
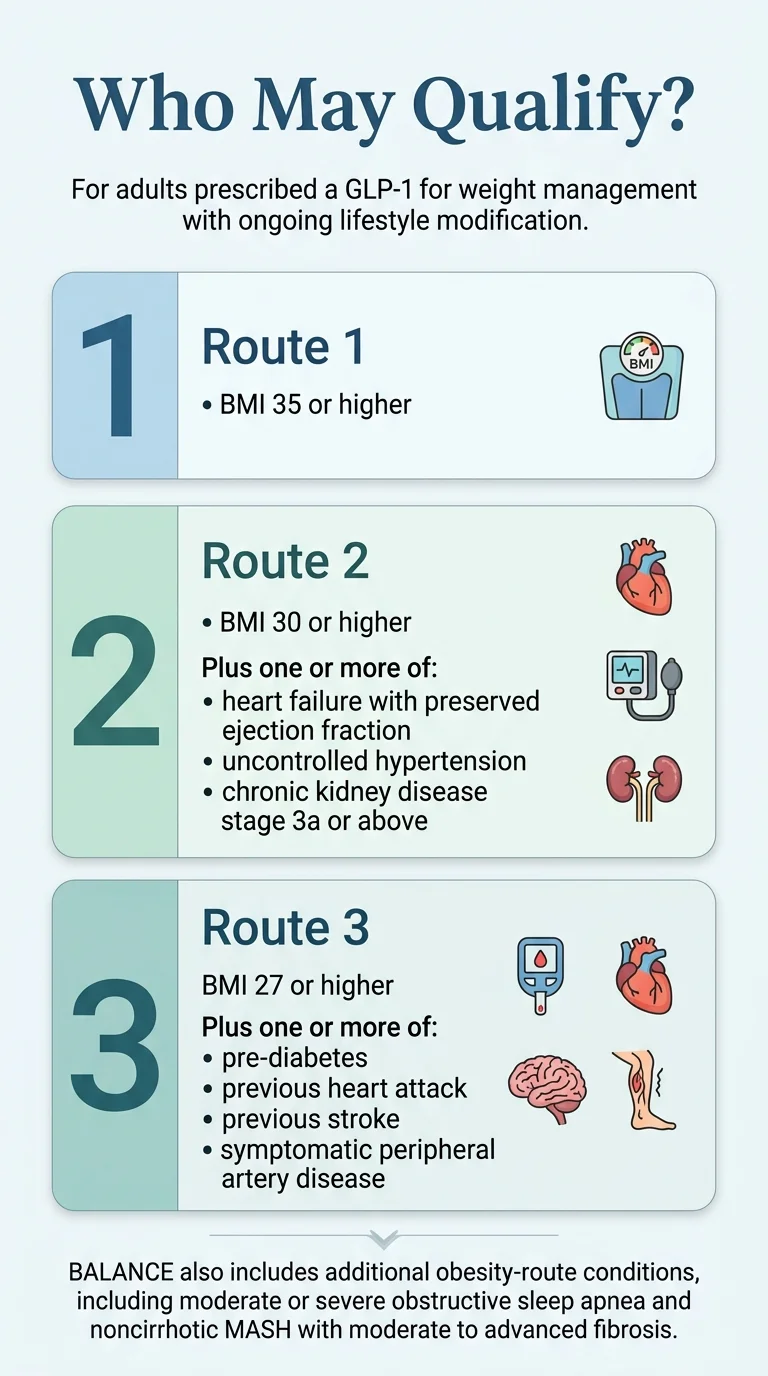
To qualify for the Medicare GLP-1 Bridge, you need all of the following:
You are 18 years or older
You are enrolled in a qualifying Medicare Part D plan for 2026
Your prescriber is prescribing the drug for weight reduction and ongoing maintenance of weight reduction, used alongside a reduced-calorie diet and increased physical activity
You meet one of the three BMI/diagnosis routes below
Route 1: BMI of 35 or Higher
If your BMI is 35 or above, you qualify based on BMI alone. No additional diagnosis is required. This is the most straightforward path. For reference: a 5'6“ person weighing 217 pounds has a BMI of approximately 35.
Route 2: BMI of 30 or Higher Plus Specific Conditions
If your BMI is between 30 and 34.9, you qualify if you also have one or more of these conditions:
- Heart failure with preserved ejection fraction (HFpEF)
- Uncontrolled hypertension (blood pressure not adequately managed with current treatment)
- Chronic kidney disease stage 3a or higher (CKD stage 3a+)
Route 3: BMI of 27 or Higher Plus Specific Conditions
If your BMI is between 27 and 29.9, you qualify if you also have one or more of these conditions:
- Prediabetes
- History of heart attack (prior myocardial infarction)
- History of stroke (prior cerebrovascular accident)
- Symptomatic peripheral artery disease (PAD)
Which Plan Types Are Eligible for the Bridge?
Standalone PDPs, MA-PD coordinated care plans (HMO, HMOPOS, Local PPO, Regional PPO)
Special Needs Plans (SNPs), Employer/union group waiver plans (EGWPs), LI NET
Private fee-for-service plans, PACE organizations, section 1876 cost contract plans, fallback plans, religious fraternal benefit plans — unless also enrolled in a standalone PDP
Dually eligible beneficiaries (those on both Medicare and Medicaid) can participate in the Bridge if they are enrolled in an eligible Part D plan type and meet the clinical criteria.
Who Qualifies Under the BALANCE Model in 2027?
The 2027 BALANCE criteria for Medicare Part D are similar to the Bridge criteria but slightly broader, because BALANCE covers both weight management and currently covered Part D uses.
BALANCE Eligibility for Weight Management
- BMI 35+ — qualifies on BMI alone
- BMI 30+ with HFpEF, uncontrolled hypertension, CKD stage 3a+, moderate or severe obstructive sleep apnea, or noncirrhotic MASH with moderate-to-advanced fibrosis (F2–F3)
- BMI 27+ with prediabetes, prior MI, prior stroke, or symptomatic PAD
BALANCE Eligibility for Currently Covered Uses
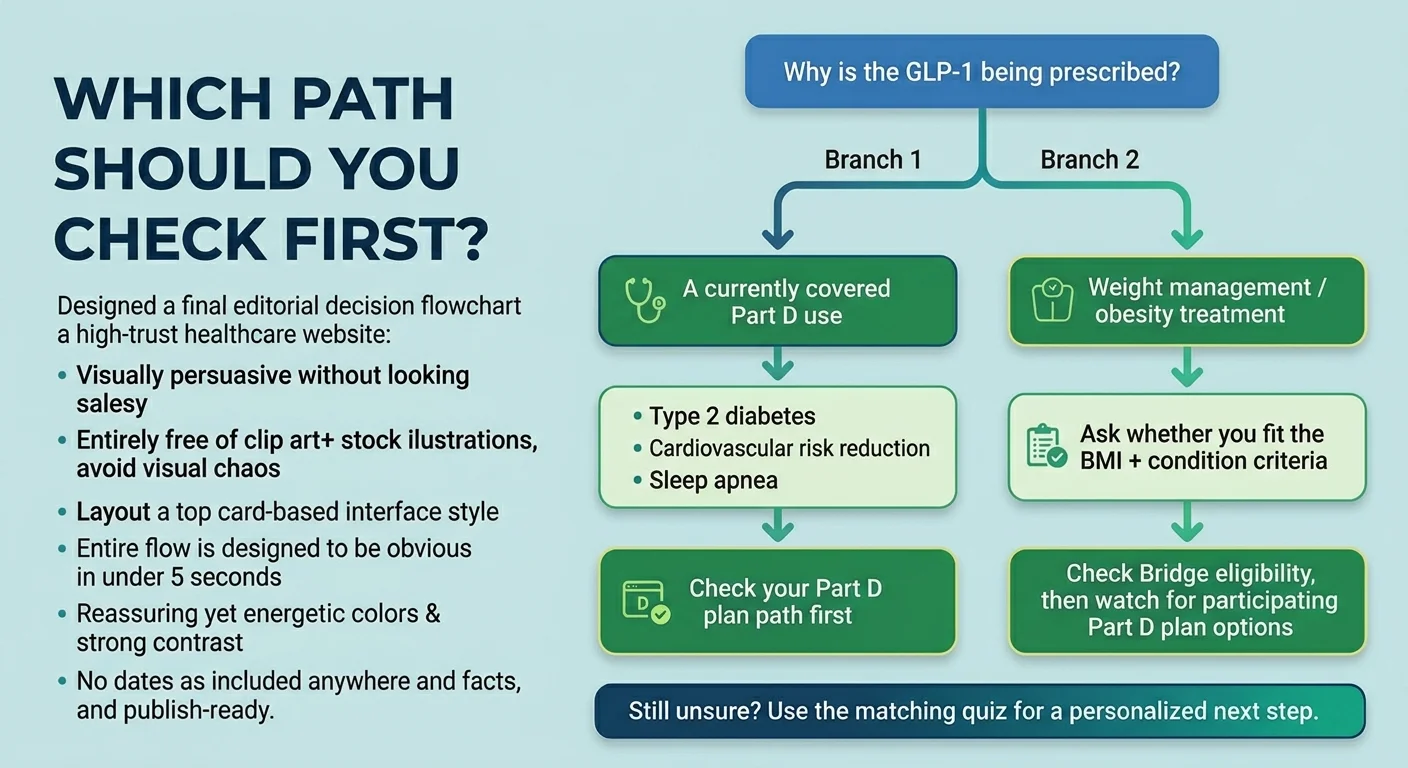
BALANCE also covers GLP-1 medications for uses that Medicare Part D already covers today — like type 2 diabetes, cardiovascular risk reduction, and obstructive sleep apnea. For these uses, the standard Part D coverage criteria apply. People who already qualify may be eligible to receive those products at a lower price in participating plans under BALANCE.
The Critical 2027 Difference
The biggest difference between Bridge and BALANCE is not the eligibility criteria — it is the plan participation requirement. CMS has set an 80% participation threshold: if Part D plans covering at least 80% of all Part D beneficiaries do not apply to participate, CMS will not move forward with BALANCE in Medicare for 2027. The target date for CMS to announce whether this threshold has been met is April 30, 2026.
During the 2026 Annual Enrollment Period (October 15 – December 7), pay close attention to which Part D plans are participating in BALANCE for 2027. If your current plan is not participating, you may need to switch to one that is — or accept that your GLP-1 coverage for weight management ends when the Bridge expires on December 31, 2026.
What GLP-1 Drugs Are Included?
Medicare GLP-1 Bridge (2026)
| Covered Under the Bridge | Manufacturer |
|---|---|
| ✓ Wegovy (semaglutide injection and oral tablets) | Novo Nordisk |
| ✓ Zepbound (tirzepatide injection) | Eli Lilly |
Ozempic, Mounjaro, and Rybelsus are not available through the Bridge. Those may be covered under your Part D plan for other indications (like diabetes), but the Bridge is specifically for weight management.
BALANCE Model (2027)
The full BALANCE drug list is significantly broader. Both Eli Lilly and Novo Nordisk have completed negotiations with CMS and agreed to participate.
| Covered Under BALANCE | Manufacturer |
|---|---|
| ✓ Mounjaro (tirzepatide) | Eli Lilly |
| ✓ Ozempic (semaglutide injection) | Novo Nordisk |
| ✓ Rybelsus (semaglutide oral tablets) | Novo Nordisk |
| ✓ Wegovy (semaglutide injection and tablets) | Novo Nordisk |
| ✓ Zepbound KwikPen (tirzepatide) | Eli Lilly |
| ✓ Orforglipron (oral, if FDA-approved by launch) | Eli Lilly |
How Much Will It Actually Cost?
This is where headlines have created the most confusion. “$50 GLP-1s for Medicare” is technically true but missing critical context.
2026 Bridge Cost: $50 Per Month (With Caveats)
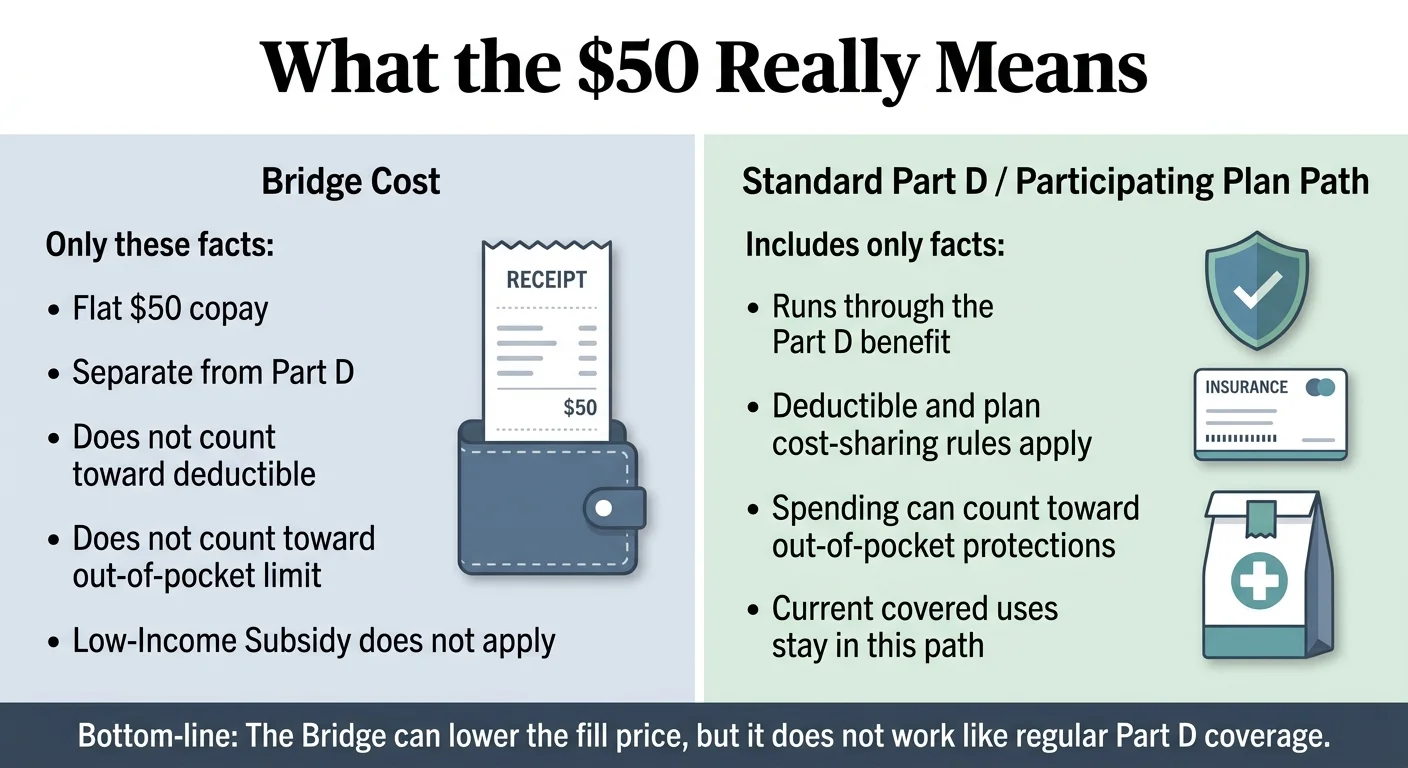
What it is
A flat $50 copay per monthly supply, every month, regardless of which phase of the Part D benefit you are in. You pay the same whether you have met your deductible or not.
What it is NOT
- Does not count toward your Part D deductible (up to $615 in 2026)
- Does not count toward your $2,100 annual out-of-pocket cap (TrOOP)
- Not covered by the Part D Low-Income Subsidy (Extra Help)
- Does not interact with your Part D benefit in any way
Over six months (July through December 2026), you will pay $300 total for Bridge medications. For context: $300 for six months of Wegovy or Zepbound compares to approximately $6,500–$8,100 at full retail pricing for the same period — a reduction of more than 95%.
2027 BALANCE Cost: It Depends on Your Plan Type
- Enhanced alternative plans and EGWPs: Up to $50 per 28–30 day supply during the initial coverage phase
- Basic alternative plans: Up to $125 per 28–30 day supply during the initial coverage phase
- Defined standard plans: Not eligible to participate in BALANCE
The important difference from the Bridge: under BALANCE, your GLP-1 costs do count toward your Part D deductible and $2,100 out-of-pocket cap. And Low-Income Subsidy benefits do apply.
Cost Comparison Table
| Cost Element | Bridge (2026) | BALANCE Enhanced/EGWP (2027) | BALANCE Basic (2027) | Retail (No Coverage) |
|---|---|---|---|---|
| Monthly copay | $50 | Up to $50 | Up to $125 | $1,086–$1,350 |
| Counts toward deductible | ❌ No | ✅ Yes | ✅ Yes | N/A |
| Counts toward OOP cap | ❌ No | ✅ Yes | ✅ Yes | N/A |
| LIS/Extra Help applies | ❌ No | ✅ Yes | ✅ Yes | N/A |
| Negotiated net drug price | $245 | $245 | $245 | Full WAC |
What Is the Lifestyle Support Program Requirement?
You will see this mentioned in almost every official document about BALANCE, and it raises questions: do I have to join a diet program to get my medication?
Here is what it actually means. Under both the Bridge and the full BALANCE Model, all beneficiaries receiving GLP-1 medications for weight management must be provided access to a lifestyle support program. These programs are provided by the drug manufacturer — not by CMS, not by your insurance company, and not by your doctor. They are provided at no cost to you.
The programs include education on reduced-calorie eating, increasing physical activity, and medication adherence. Think of it as structured support — not a gym membership requirement or a mandatory diet class.
Key Dates: Your CMS BALANCE Model Timeline
Here is every date that matters, in order.
Already happened
December 23, 2025
CMS announces the BALANCE Model and Medicare GLP-1 Bridge
January 8, 2026
Manufacturer RFA and state/plan Notices of Intent were due
February 2026
CMS completes manufacturer negotiations (Eli Lilly and Novo Nordisk confirmed)
March 2026
CMS releases detailed Medicare GLP-1 Bridge FAQ with eligibility criteria and operational design
Coming up
April 20, 2026
Part D plan sponsor applications due for BALANCE Model participation
April 30, 2026 (target)
CMS announces whether the 80% Part D participation threshold has been met for 2027 BALANCE launch
May 1, 2026
BALANCE Model launches for participating state Medicaid programs (rolling enrollment through December)
July 1, 2026
Medicare GLP-1 Bridge goes live nationwide — $50/month Wegovy and Zepbound for eligible Part D beneficiaries
July 31, 2026
State Medicaid Agency RFA deadline for BALANCE
October 15 – December 7, 2026
Medicare Annual Enrollment Period — critical for choosing a 2027 Part D plan that participates in BALANCE
December 31, 2026
Medicare GLP-1 Bridge ends
January 1, 2027
BALANCE Model launches for participating Medicare Part D plans
December 2031
BALANCE Model testing period concludes
Does Medicare Cover GLP-1 for Prediabetes, Sleep Apnea, Heart Disease, or Diabetes?
Each condition has a different coverage pathway, and getting this wrong could cost you months of delays or unnecessary out-of-pocket spending.
Prediabetes
Short answer: Prediabetes can qualify you for Bridge and BALANCE GLP-1 coverage for weight management — but only if your BMI is 27 or higher.
Prediabetes is listed as a qualifying condition under Route 3 of the Bridge eligibility criteria (BMI 27+ with specified comorbidities). It is not a blanket Part D benefit. If you have prediabetes but a BMI below 27, the Bridge and BALANCE weight-management pathways do not currently apply to you. If your doctor has diagnosed prediabetes and your BMI is 27 or above, the Bridge could be your path starting July 2026.
Obstructive Sleep Apnea (OSA)
Short answer: It depends on which program and which drug.
There are two different coverage pathways. First: Zepbound for moderate to severe OSA in adults with obesity received FDA approval in December 2024. Because this is a Medicare-coverable Part D indication (not weight loss), your Part D plan may already cover Zepbound for this use under its standard formulary — that coverage goes through your plan's normal process, not through the Bridge. Second: Under BALANCE (2027), moderate or severe OSA is listed as a qualifying comorbidity for the BMI 30+ weight-management pathway. If you have OSA, talk to your doctor about which coverage pathway makes the most sense.
Cardiovascular Disease
Short answer: Wegovy for cardiovascular risk reduction is already a coverable Part D use. The Bridge may not be your best path.
In March 2024, the FDA approved Wegovy to reduce the risk of major adverse cardiovascular events in adults with established cardiovascular disease who are either obese or overweight. Medicare Part D plans can cover Wegovy for this use now, though coverage varies by formulary. If you have established cardiovascular disease, the coverage pathway for that use runs through your Part D plan rather than the Bridge — and Part D payments count toward your deductible and OOP cap. Additionally, if your cardiovascular history includes a prior heart attack, prior stroke, or symptomatic PAD, those qualify you for the Bridge and BALANCE weight-management criteria under Route 3 (BMI 27+).
Type 2 Diabetes
Short answer: GLP-1 medications for type 2 diabetes are generally covered under Medicare Part D already.
Part D plans generally cover GLP-1s for FDA-approved indications such as type 2 diabetes, but whether a specific product is on your formulary — and what prior authorization or step therapy rules apply — varies by plan. Under the 2026 Part D benefit structure, your annual out-of-pocket costs for covered drugs are capped at $2,100. Where BALANCE adds value for diabetes patients: if you have both type 2 diabetes and obesity, a participating BALANCE plan in 2027 may offer additional GLP-1 formulations or more favorable pricing for weight-management uses.
What Could Still Stop You From Getting Coverage
We have been giving you the good news. Here is the honest risk picture — because you deserve to make decisions based on the full truth, not headlines.
The 80% Participation Threshold
CMS requires that Part D plans covering at least 80% of all Part D beneficiaries apply to participate in BALANCE for the model to launch in Medicare in 2027. If that threshold is not met, CMS will not move forward with BALANCE for Part D plans. The target date for CMS to announce whether the threshold is met is April 30, 2026. This is the single biggest 'what if' in the entire BALANCE Model.
The Plan-Switching Risk
If you start on the Bridge in July 2026, you need your Part D plan to participate in BALANCE for 2027. If your plan does not opt in, you face a choice: switch to a participating plan during open enrollment (potentially disrupting coverage for your other medications) or lose GLP-1 weight-management coverage on January 1, 2027. KFF has highlighted this risk prominently.
BALANCE Is Voluntary — And That Means Uncertain
Every link in the chain is voluntary. Manufacturers chose to participate (Lilly and Novo Nordisk are in). State Medicaid agencies choose whether to participate (only 13 states covered GLP-1s for obesity in Medicaid as of January 2026 — down from 16 in 2025). Part D plans choose whether to participate. CMS itself states: 'This model will not guarantee coverage for any individual.'
What Happens After 2031?
BALANCE is a demonstration model, not permanent legislation. The model testing period runs through December 2031. The underlying statutory Medicare exclusion on weight-loss drug coverage still exists. Whether that changes depends on Congress.
What About Medicaid Under BALANCE?
The BALANCE Model covers both Medicare and Medicaid, but the Medicaid pathway has its own rules and timeline.
Medicaid Timeline
State Medicaid programs can begin participating in BALANCE on a rolling basis starting May 1, 2026, with the enrollment window remaining open through at least January 2027. The State Medicaid Agency RFA deadline is July 31, 2026.
How Medicaid BALANCE Works
CMS has negotiated supplemental rebate agreements with participating manufacturers that go on top of existing statutory Medicaid drug rebates. States that join must adopt standardized coverage criteria (similar to the Medicare criteria). The BALANCE key terms apply equally in fee-for-service and managed care.
The State Participation Problem
Medicaid coverage of GLP-1s for obesity is optional for states, and many states have been pulling back. As of January 2026, only 13 state Medicaid programs covered GLP-1s for obesity — down from 16 in 2025. States like California, New Hampshire, Pennsylvania, and South Carolina eliminated coverage, largely due to budget pressures. BALANCE could reverse this trend by offering states better pricing, but participation is voluntary.
What Medicaid Enrollees Pay
Medicaid prescription cost-sharing is generally limited to nominal amounts that vary by state and eligibility group. If your state participates in BALANCE and you meet the eligibility criteria, this is potentially the most affordable path to GLP-1 access anywhere in the healthcare system.
What If You Cannot Wait — or Do Not Qualify?
The Medicare GLP-1 Bridge does not start until July 2026. BALANCE does not start until 2027. Some people do not meet the BMI criteria. Some people's states will not participate. Some people are not on Medicare or Medicaid at all. If any of that describes you, you still have options worth exploring.
FDA-Approved GLP-1s Through a Telehealth Provider
If you have employer insurance, VA coverage, or another plan that covers GLP-1s, telehealth platforms like Ro can help you navigate coverage for medications like Wegovy or Zepbound. Ro offers physician-supervised care, dose management, and insurance navigation tools — though Ro does not coordinate coverage for government insurance programs like Medicare or Medicaid. For cash-pay patients, Ro connects eligible users with manufacturer discount programs.
FDA-Approved GLP-1 — Available Now
Check your eligibility for FDA-approved GLP-1 treatment through Ro
Licensed physicians, FDA-approved Wegovy and Zepbound, ongoing clinical support. If you have private insurance, Ro can help navigate coverage. Cash-pay options also available with manufacturer pricing programs.
Check eligibility on Ro →Cash-pay path. Ro cannot coordinate GLP-1 coverage for government insurance programs.
Compounded GLP-1 Medications for Cash-Pay Patients
For people paying entirely out of pocket — including Medicare beneficiaries who cannot use manufacturer copay cards under federal law — compounded GLP-1 medications through a telehealth provider can be significantly more affordable than brand-name retail pricing. MEDVi is a straightforward option starting at $179 for the first month, with no contracts or membership fees, and includes physician oversight and care team access.
An important distinction: compounded GLP-1 medications are not FDA-approved as finished drug products. They are prepared by licensed, regulated compounding pharmacies and prescribed by licensed physicians — but they have not gone through the same approval process as brand-name medications like Wegovy. If having an FDA-approved product matters most to you, the Bridge (starting July 2026) or a brand-name pathway through insurance is a better fit.
Most Affordable Option — Available Now
See current MEDVi pricing and availability
Compounded semaglutide and tirzepatide from $179/month. Licensed physicians, U.S. compounding pharmacies, no contracts. Note: compounded GLP-1s are not FDA-approved finished drugs — understand the distinction before deciding.
See MEDVi pricing →Not Sure Which Path Fits?
Our free matching quiz takes 60 seconds and asks about your insurance, BMI, timeline, and budget — then tells you which path (Bridge, BALANCE, private insurance, or cash-pay) makes the most sense for your specific situation.
Take the 60-second GLP-1 matching quiz →Step by Step: How to Prepare for the Medicare GLP-1 Bridge
If you think you qualify for the Bridge, here is your action plan between now and July 2026. Each step builds on the one before it.
Confirm your Medicare Part D enrollment
You must be enrolled in a qualifying Part D plan for 2026. If you are not currently enrolled in Part D, you may be able to join during a Special Enrollment Period — act quickly, as there are time limits and potential late enrollment penalties.
Know your BMI and health history
Review the three eligibility routes above. Calculate or confirm your current BMI. Gather documentation of any qualifying comorbidities (prediabetes, prior MI, prior stroke, symptomatic PAD, HFpEF, uncontrolled hypertension, CKD stage 3a+).
Talk to your doctor before July
Do not wait until July 1 and hope it works out. Schedule an appointment with your prescriber now and discuss whether a GLP-1 for weight management is appropriate for you. If it is, your doctor can prepare the prior authorization paperwork in advance.
Understand the prior authorization process
Your doctor submits the prior authorization to CMS's central processor — not to your insurance company. This is different from how most prescriptions work. Make sure your doctor's office knows this.
Budget for $50 per month starting July
The Bridge copay is separate from your regular Part D costs. Over six months, plan for $300 in additional out-of-pocket spending.
Plan for the 2027 transition
During the Annual Enrollment Period (October 15 – December 7, 2026), research which Part D plans in your area are participating in BALANCE for 2027. If your current plan is not participating, seriously consider switching. Your continued GLP-1 access depends on it.
Save this page
Bookmark it. We update it as CMS releases new guidance, and we will add BALANCE plan participation data as soon as it becomes available.
How We Verified This Page
Every factual claim on this page is sourced from official CMS guidance or verified policy analysis. We do not speculate, and we do not fill in blanks with assumptions.
Primary sources used:
- CMS BALANCE Model official page — program overview, eligibility, timeline, FAQ
- CMS Medicare GLP-1 Bridge FAQ — Bridge-specific eligibility criteria, cost mechanics, operational details, plan type eligibility (updated March 9, 2026)
- CMS BALANCE Model RFA (manufacturer) — model design elements, negotiation framework
- KFF: What to Know About the BALANCE Model for GLP-1s in Medicare and Medicaid — independent policy analysis, 80% threshold, LIS implications, transition risks
- KFF Quick Take: What Medicare's Temporary Program Covering GLP-1s for Obesity Means for Beneficiaries
- CMS Press Release: CMS Launches Voluntary Model — official announcement, December 23, 2025
Last verified: March 25, 2026
Update log: March 25, 2026 — Updated with latest CMS Bridge FAQ guidance (March 9, 2026 revision), KFF BALANCE explainer (March 24, 2026), and CY2027 Part D cost-sharing details.
Frequently Asked Questions
Is the CMS BALANCE Model the same as the Medicare GLP-1 Bridge?
No. The Bridge is a temporary, six-month Section 402 demonstration (July–December 2026) that CMS runs directly. BALANCE is a longer-term Innovation Center model (2027–2031) that operates through participating Part D plans. The Bridge acts as a stopgap while BALANCE gets set up for Medicare.
Will all Medicare beneficiaries pay $50 for Wegovy or Zepbound?
Under the Bridge (2026), eligible beneficiaries pay $50 per month flat. Under BALANCE (2027), it depends on your plan type. Enhanced alternative plans and EGWPs are capped at $50. Basic alternative plans are capped at $125. Defined standard plans cannot participate in BALANCE.
Does the $50 Bridge copay count toward my Part D deductible or out-of-pocket cap?
No. The Bridge operates outside the Part D benefit. Your $50 monthly copay does not reduce your deductible (up to $615 in 2026) and does not count toward the $2,100 annual out-of-pocket cap. Under BALANCE in 2027, cost-sharing does count toward your Part D deductible and OOP cap.
Does Medicare cover GLP-1 for prediabetes?
Prediabetes qualifies you for the Bridge and BALANCE weight-management criteria if your BMI is 27 or higher (Route 3). It is not a standalone Part D coverage indication outside these programs. If you have prediabetes and a BMI of 27+, talk to your doctor about the Bridge starting in July 2026.
Does Medicare cover GLP-1 for sleep apnea?
Zepbound for moderate to severe obstructive sleep apnea in adults with obesity may be coverable under your Part D plan right now — that is a current Medicare-covered indication, not a Bridge or BALANCE pathway. Coverage depends on your plan's formulary. Under BALANCE (2027), moderate or severe OSA is also listed as a qualifying comorbidity for the BMI 30+ weight-management route.
What if I already get Wegovy or Zepbound through my Part D plan?
If your GLP-1 is covered under Part D for a currently approved indication (like cardiovascular risk reduction or sleep apnea), that coverage continues. The Bridge is specifically for weight-management use. CMS has said it will monitor plans to prevent shifting existing Part D prescriptions to the Bridge.
Which Part D plan types can participate in the Bridge?
Eligible plan types include standalone PDPs, MA-PD coordinated care plans, SNPs, EGWPs, and LI NET. CMS excludes private fee-for-service plans, section 1876 cost contract plans, section 1833 health care prepayment plans, PACE organizations, fallback plans, and religious fraternal benefit plans — unless also enrolled in a standalone PDP.
Will I have to switch Part D plans in 2027?
Possibly. If your current plan does not participate in BALANCE, you would need to switch to a participating plan during the 2026 Annual Enrollment Period (October 15 – December 7) to maintain weight-management GLP-1 coverage in 2027. Switching plans can affect cost-sharing, formulary coverage, and pharmacy networks for your other medications.
What happens if BALANCE participation is too low?
CMS set an 80% threshold: if Part D plans covering at least 80% of beneficiaries do not apply to participate, CMS will not launch BALANCE in Medicare for 2027. The target date for CMS to announce the result is April 30, 2026. If the threshold is not met, CMS may pursue alternative approaches.
Still Not Sure Which GLP-1 Program Is Right for You?
We built this page to be the most complete, plainest-English guide to the CMS BALANCE Model anywhere on the internet. But we also know that everyone's situation is different. Your BMI, your diagnoses, your insurance plan, your state, your budget, your timeline — all of those variables affect which path makes sense for you.
Whether you are preparing for the Medicare GLP-1 Bridge in July, exploring BALANCE for 2027, or looking for affordable access right now — the right program depends on where you stand today.
Take the free 60-second GLP-1 matching quiz
We'll ask you four quick questions and match you with the coverage pathway — or provider — that fits your exact situation. No commitment, no email required, and you'll have a clear next step in under a minute.
Take the free 60-second GLP-1 matching quiz →Related Guides
This guide is for informational purposes only and does not constitute medical advice. Always consult with your healthcare provider before starting any medication. The RX Index may receive compensation from providers mentioned on this page. This does not influence our coverage of government programs or the accuracy of anything on this page. See our full editorial policy and advertising disclosure.
Last updated: March 25, 2026 · Verified against CMS.gov: March 25, 2026