Last verified: · NovoCare, LillyDirect, Ro, and Sesame pricing confirmed · CMS GLP-1 Bridge FAQ reviewed · Medi-Cal Rx policy current
Insurance Guide · April 2026
What If My Insurance Doesn't Cover Weight-Loss Medication? Your 2026 Action Plan
By The RX Index Editorial Team — a pricing intelligence and comparison resource for GLP-1 telehealth providers
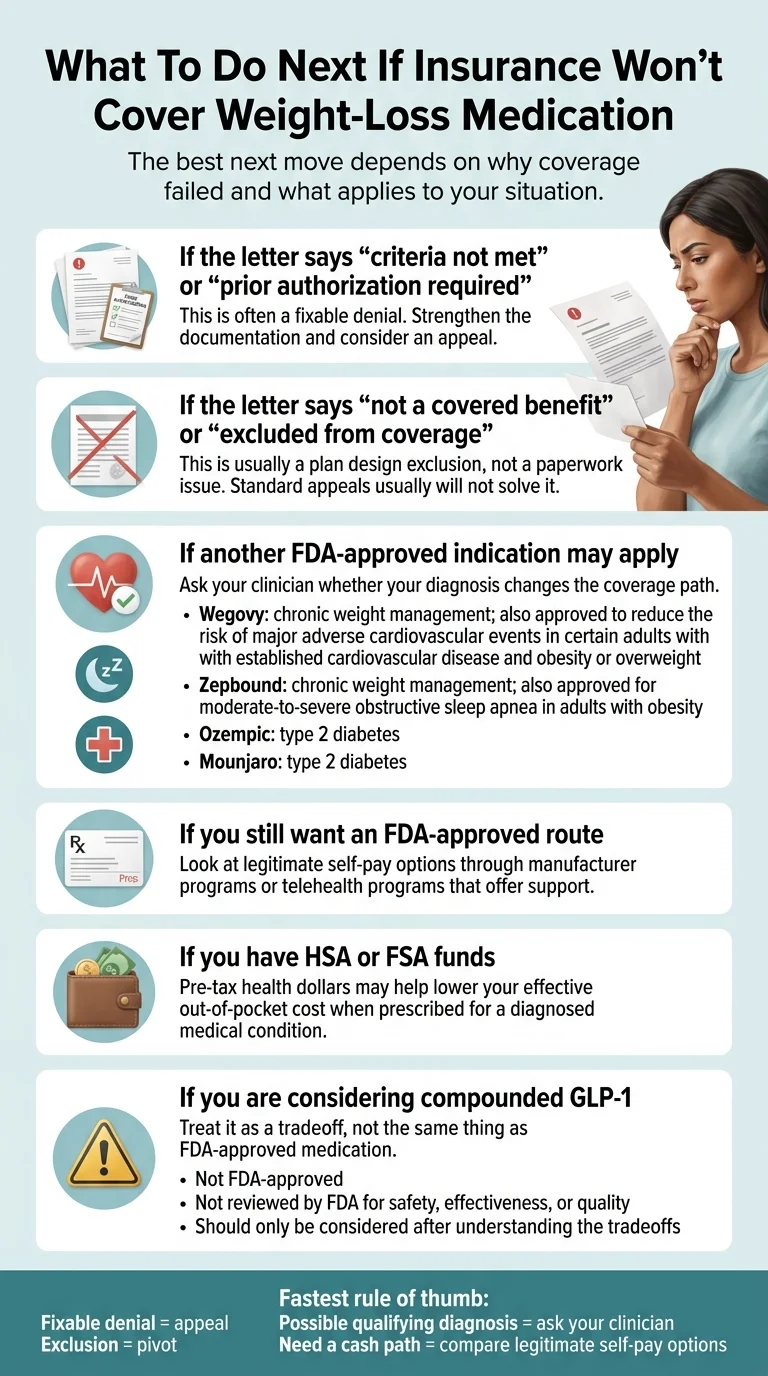
If your insurance doesn't cover weight-loss medication, the first move isn't to panic — it's to figure out which kind of “no” you got. A denial that says “criteria not met” or “prior authorization required” is usually fixable with better paperwork or a formal appeal. A denial that says “not a covered benefit” or “excluded from coverage” is a different problem — standard appeals won't move it, and you need to pivot fast. Verified FDA-approved self-pay now starts at $149/month for the Wegovy pill or the Foundayo starting dose, $199/month intro for the Wegovy pen, and $299/month for Zepbound. Below, we decode your denial letter, show you whether an appeal is worth filing, and lay out every legitimate path if coverage really is a dead end.
By The RX Index Editorial Team. The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. Last verified: .
What we actually verified for this page. We pulled current pricing directly from NovoCare, LillyDirect, Ro, and Sesame. We checked the FDA's approval language for Wegovy's cardiovascular indication and Zepbound's obstructive sleep apnea indication. We read CMS's March 3, 2026 FAQ on the Medicare GLP-1 Bridge and the April 2026 BALANCE update. We pulled the Medi-Cal Rx policy document that took effect January 1, 2026. We used HealthCare.gov for federal internal and external appeal rights, IRS Publication 502 for HSA/FSA rules, and the KFF 2025 Employer Health Benefits Survey for employer coverage stats.
Why You're Here, and Why It's Not Your Fault
You filled out the paperwork. Your doctor thought it made sense. You walked into the pharmacy expecting a normal copay. Somewhere between “congratulations, you qualify” and the register, someone said no.
That “no” could have come from your insurer, your pharmacy benefits manager, your employer's 2026 plan redesign, or your state Medicaid program quietly changing the rules on January 1. Your frustration isn't weakness — it's math. Without help, the list price for Wegovy runs about $1,349/month and Zepbound runs about $1,087/month in most pharmacies. That number is why the November 2025 KFF Health Tracking Poll found 56% of GLP-1 users said the drugs were difficult to afford, with 25% calling them “very difficult.”
We're not going to rehearse why weight is a medical issue. You already know. Let's go to the part where we figure out what to do next.
Step 1: Decode Your Denial Letter in 60 Seconds
Every weight-loss medication denial falls into one of five buckets, and the bucket determines whether you fight it, reframe it, or pivot. KFF's analysis of 2024 Medicare Advantage data found only 11.5% of denied prior authorization requests were ever appealed — but of those that were, 80.7% were overturned, fully or partially. The catch: those numbers only apply to the right kind of denial.
Pull out your denial letter. Look for the phrase the insurer used. Then find it here.
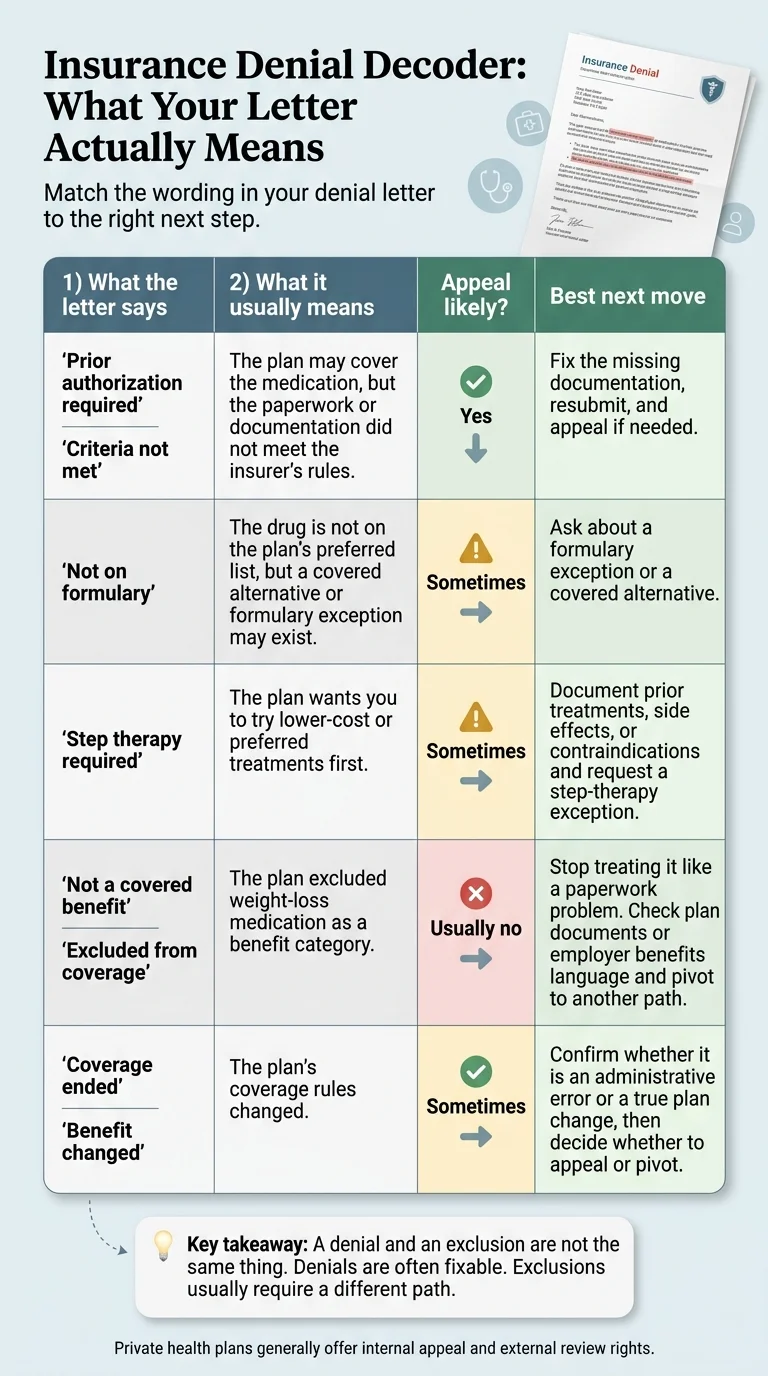
| What your letter says | What it usually means | Can you appeal? | Your best next move |
|---|---|---|---|
| "Prior authorization required" or "Criteria not met" | The plan may cover the drug, but the paperwork didn't meet their criteria — BMI threshold, comorbidity documentation, prior-therapy history. | Yes | Fix the missing documentation and resubmit. If resubmission fails, file a formal appeal with a letter of medical necessity. |
| "Not on formulary" | The drug isn't on your plan's preferred list. The class may still be covered — a different drug might be. | Sometimes | Ask about a formulary exception, or whether the preferred alternative is covered instead. |
| "Step therapy required" | The plan wants you to try cheaper options first — phentermine, Contrave, or sometimes Wegovy before Zepbound. | Sometimes | Document prior trials with dates, doses, side effects, or contraindications. Request a step-therapy exception. |
| "Not a covered benefit" or "Excluded from coverage" | The entire category has been carved out of your plan. Not a paperwork problem — a plan design problem. | Usually not | Stop appealing. Check your plan documents for any exception process, escalate to your employer benefits team if self-funded, or pivot straight to a self-pay path. |
| "Benefit changed" or "Coverage ended" | Your plan year rolled over and the employer or insurer changed what's covered. | Only sometimes | Confirm whether it's an administrative error (fixable) or a true benefit change (not fixable through appeal). |
Why this decoder matters: most articles treat every denial as a paperwork fight. That framing burns readers weeks of time when they're actually dealing with a benefit exclusion. Blue Cross Blue Shield of Massachusetts says it plainly in their own provider bulletin: “No. This is a benefit exclusion that can't be appealed.” Don't spend your one good month of fight energy on the wrong battle.
Not sure which bucket you're in?
Ro runs a free benefits check with your insurer and returns a personalized coverage report. No membership required. Their own data found 43% of users have coverage of a GLP-1 for weight loss — and most didn't know it.
Check my GLP-1 coverage free on Ro → (sponsored affiliate link, opens in a new tab)Denial vs. Exclusion: The One Distinction That Saves Weeks
A denial means your insurer reviewed your specific request and said no. An exclusion means the entire medication category was removed from the plan for everyone. Denials are usually appealable under federal internal and external review rules. Exclusions are not — they're a plan design decision, and arguing medical necessity won't move them.
A prior authorization denial is about you. The plan covers Wegovy for weight loss in principle. But your PA didn't include your second BMI measurement, or your comorbidity code was wrong, or you hadn't documented a lifestyle attempt. Those are fixable.
A benefit exclusion is about the plan. Your employer, your insurer, or your PBM removed weight-loss drugs from the formulary. Nobody on this plan gets Wegovy for weight loss, no matter how perfect their paperwork is. BCBS Massachusetts spells this out in their own provider materials: “This is a benefit exclusion that can't be appealed.”
The reason this matters in 2026 specifically: the exclusion wave is real.
- CVS Caremark removed Zepbound from its standard formulary effective July 1, 2025, preferring Wegovy — CVS Caremark members whose employers didn't buy a rider are in an exclusion if they need Zepbound specifically.
- BCBS Massachusetts excluded Wegovy, Zepbound, and Saxenda for weight loss starting January 1, 2026, except where an employer with 100+ employees purchased a rider. No exceptions. No appeal.
- Health New England and Fallon Health dropped Wegovy, Zepbound, and Saxenda for individual and small-group members effective January 1, 2026 — no grandfathering.
- Medi-Cal eliminated GLP-1 coverage for weight loss for members age 21 and older on January 1, 2026. All previously approved prior authorizations expired December 31, 2025. No transition period.
- New Hampshire, Pennsylvania, and South Carolina Medicaid also eliminated weight-loss coverage on January 1, 2026.
If your denial letter uses the words “excluded,” “carved out,” “not a covered benefit,” or “not eligible” — that's an exclusion. Skip to the self-pay section and stop spending time on an appeal that can't win.
How to Tell If Your Appeal Is Worth Filing
You generally have 180 days to file an internal appeal on a commercial plan denial. External review by an independent reviewer is a federal right for most commercial plans under HealthCare.gov rules.
The five-step commercial appeal when it's worth doing
- Read the denial word for word. Underline the exact phrase. That phrase is your strategy.
- Request the clinical criteria the plan used. You have a right to this document. If they denied for BMI but you meet the threshold, their records may be wrong.
- Get a stronger Letter of Medical Necessity. The best LMNs address the specific denial reason, not generic “this drug is helpful.” See our GLP-1 letter of medical necessity guide for the 6-point checklist.
- File the internal appeal. Most plans give you 180 days. Send it certified. Include the denial letter, the clinical criteria, the new LMN, all supporting chart notes, and a one-page cover summary.
- Escalate. If the internal appeal fails, request a peer-to-peer review (your doctor talks to the insurer's medical director). If that fails, request external review by an independent reviewer.
When an appeal is probably the wrong fight
- Your letter says “not a covered benefit” or “excluded from coverage” — this is a plan design issue, not a medical necessity issue
- Your employer removed the obesity-drug rider for 2026 and HR has confirmed no exception process exists
- You've already appealed and gotten the same exclusion language back unchanged
- You're on Medicare Part D and the drug is prescribed purely for weight loss (federal law excludes this)
What a medical necessity letter should include
- Two separate BMI measurements documenting obesity (BMI ≥30) or overweight with comorbidity (BMI ≥27)
- Specific ICD-10 diagnosis codes for your weight-related conditions
- Documentation of prior lifestyle interventions and weight-management attempts, with dates and outcomes
- Documentation of prior pharmacologic attempts if step therapy is at issue
- A specific clinical rationale for why this drug, at this dose, for this patient
Want someone to handle the paperwork?
Ro's insurance concierge handles the PA and the appeal as part of their Body membership. Their own workflow page says the full insurance process takes about 2–3 weeks. If coverage comes through, your medication can drop as low as $25/month with a commercial savings card. If it doesn't, you transition to Ro's cash-pay pricing at manufacturer parity.
Note: Ro does not currently coordinate coverage for Medicare, Medicaid, or TRICARE, except for FEHB. If that's your situation, skip to the Medicare section below.
Start with Ro's insurance concierge → (sponsored affiliate link, opens in a new tab)The Two FDA-Approved Indications Most People Miss
The FDA approved Wegovy for cardiovascular risk reduction in adults with established heart disease and obesity/overweight, and Zepbound in December 2024 for moderate-to-severe obstructive sleep apnea in adults with obesity. When a genuine diagnosis fits these on-label uses, many plans — and Medicare Part D — will cover the drug, because the indication is not weight loss.
The Wegovy cardiovascular-risk-reduction pathway
The FDA approved Wegovy in March 2024 for reducing major adverse cardiovascular events (heart attack, stroke, cardiovascular death) in adults with established cardiovascular disease who have obesity or overweight. That's a separate coverage lane.
You may qualify if you have:
- Documented cardiovascular disease (prior heart attack, prior stroke, established coronary artery disease, or peripheral artery disease), AND
- BMI ≥27
Why this matters: Medicare Part D can cover Wegovy for CV risk reduction even though weight-loss-only coverage remains prohibited by statute. Commercial plans that exclude weight-loss GLP-1s sometimes still cover this indication because it's a different therapeutic category.
The Zepbound obstructive sleep apnea pathway
The FDA approved Zepbound in December 2024 for moderate-to-severe OSA in adults with obesity — the first and only GLP-1 with an FDA-approved sleep apnea indication.
You may qualify if you have:
- Moderate-to-severe OSA confirmed by sleep study (AHI ≥15), AND
- BMI ≥30
| Drug | Approved indication that may change coverage | What your plan will want to see |
|---|---|---|
| Wegovy | Cardiovascular risk reduction in adults with established CV disease + BMI ≥27 | Documented CV event or diagnosis, BMI measurement |
| Wegovy | Moderate-to-advanced liver scarring in adults with MASH (approved August 2025) | Liver biopsy or imaging with fibrosis staging |
| Zepbound | Moderate-to-severe OSA in adults with obesity | Sleep study with AHI ≥15, BMI ≥30 |
| Ozempic / Mounjaro | Type 2 diabetes (not weight loss) | A1C, diabetes diagnosis codes |
The Real Self-Pay Landscape (with Verified 2026 Prices)
FDA-approved self-pay starts at $149/month for the Wegovy pill and the Foundayo 0.8 mg starter dose, $199/month intro for the Wegovy pen, and $299/month for Zepbound at the starter vial or KwikPen dose. Every price below was verified on .
Direct-from-manufacturer self-pay
| Option | Starting price | Full price ladder | Refill-timing catch |
|---|---|---|---|
| Wegovy pill (NovoCare) | $149/mo | $149 for 1.5 mg and 4 mg (4 mg through Aug 31, 2026); $299 for 9 mg; $299 for 25 mg | 4 mg intro ends Aug 31, 2026 → then $199 |
| Wegovy pen (NovoCare) | $199/mo intro | First two new-patient fills at $199; most doses $349/mo after December 31, 2026; HD doses $399/mo | Intro pricing ends December 31, 2026 |
| Foundayo (LillyDirect) | $149/mo | $149 (0.8 mg) · $199 (2.5 mg) · $299 (5.5 mg) · $299 (9 mg) · $349 (14.5 mg) · $349 (17.2 mg) | 14.5 mg and 17.2 mg drop to $299 if refilled within 45 days |
| Zepbound vials (LillyDirect) | $299/mo | $299 (2.5 mg) · $399 (5 mg) · $499 (7.5 mg) · $699 (10 mg) · $699 (12.5 mg) · $699 (15 mg) | 7.5–15 mg drop to $449 with Self Pay Journey Program if refilled within 45 days |
| Zepbound KwikPen (LillyDirect) | $299/mo | Same as vials: $299–$699; 7.5 mg+ drop to $449 with Self Pay Journey Program | Launched Feb 23, 2026; same 45-day refill rule |
| TrumpRx | $149/mo (Wegovy pill) | Wegovy pill $149 · Wegovy/Ozempic pens $199 · Zepbound $299+ · Foundayo $149 starter | Routes through manufacturer programs and retail pharmacy coupons |
⚠ Zepbound price cliff: If you're at 10 mg or above and miss the 45-day refill window, regular price is $699/month — not the $449 Self Pay Journey rate. Set a calendar reminder around day 30–35. Same concept for Foundayo's top two doses — the $299 you planned for becomes $349 if you miss the window.
Through a telehealth partner with insurance help included
| Option | Program cost | Medication cost | What you get beyond direct |
|---|---|---|---|
| Ro Body Program | $39 first month, then $149/mo; as low as $74/mo with annual prepay | Matches LillyDirect and NovoCare pricing. With insurance + savings card: as low as $25/mo | Free Insurance Coverage Checker (no signup), insurance concierge for PA and appeals, unified care team, access to Foundayo/Wegovy pill/pen/Zepbound pen/KwikPen |
| Success by Sesame | $59–$99 per 28-day cycle ($59 with annual subscription) | Wegovy and Ozempic injection at $349/mo for Costco members; Wegovy pill from $149/mo; Zepbound KwikPen from $299/mo; Foundayo from $149/mo | Broad FDA-approved formulary, choose-your-own-provider model, Costco Pharmacy partnership for members |
Choosing between them
- Already have a prescription and just want the cheapest FDA-approved fill? Go direct to LillyDirect or NovoCare.
- Don't have a prescription yet and your insurance might still cover something? Start with Ro's free Coverage Checker before you commit to anything.
- Costco member? Sesame + Costco Pharmacy is the cheapest brand-name injection path — $349/month for Wegovy or Ozempic.
- Want the lowest-friction “handle it for me” experience with FDA-approved meds? Ro's insurance concierge and unified care team are built for exactly this.
One honest admission about Ro
Ro does NOT make sense if you already have a prescription and only want the absolute cheapest brand-name fill. In that case, LillyDirect or NovoCare direct is cheaper because Ro adds a membership fee you don't need. But if your real question is still “can insurance cover this, or can someone help with the paperwork?” — that's where Ro wins. Ro isn't trying to be the cheapest raw price. It's the lowest-friction way from “I was denied” to “I'm on treatment.”
One Thing Most Readers Don't Realize: Self-Pay Doesn't Count Toward Your Deductible
If you fill a Wegovy prescription using NovoCare self-pay (or Zepbound through LillyDirect, or Foundayo through the Lilly Savings Card), that payment is made outside your insurance — it does not count toward your annual deductible or out-of-pocket maximum. NovoCare states this on their own pricing page. It means a year of $349/month Wegovy self-pay is a full $4,188 out of pocket that doesn't count toward anything else in your plan.
That's usually still the right math when insurance is a dead end, but it's the math. One workaround: if you have commercial insurance that does cover the drug (even with a high copay), using your plan to pay may cost more per month but puts you closer to your out-of-pocket max — which can matter if you have other medical expenses coming.
Path-by-Path Segmentation: Which Route Fits You
Most readers don't need “the best provider.” They need the best route. Match your situation to the right next step.
| Your situation | Best first move |
|---|---|
| Denial letter says "criteria not met" or "prior authorization required" | File the appeal with a stronger LMN. Let Ro's insurance concierge handle the paperwork if you want help. |
| Denial letter says "not a covered benefit" or "excluded" | Skip the appeal. Ask HR about a rider if your plan is self-funded; pivot to a self-pay path. |
| You have documented cardiovascular disease history | Ask your cardiologist about Wegovy's CV risk reduction indication. |
| You have moderate-to-severe sleep apnea | Get the sleep study and ask about Zepbound's OSA indication. |
| You have confirmed MASH with moderate-to-advanced fibrosis | Ask about Wegovy's MASH indication (approved August 2025). |
| You already have a current GLP-1 prescription and want the cheapest fill | LillyDirect or NovoCare direct — skip the membership fees. |
| You don't have a prescription yet and want someone to check insurance | Ro's free Insurance Coverage Checker (no signup required). |
| You're a Costco member | Sesame + Costco Pharmacy for $349/month Wegovy or Ozempic. |
| You're on Medicare Part D and have qualifying diagnoses | The Medicare GLP-1 Bridge opens July 1, 2026. Talk to your prescriber now. |
| You're in California, New Hampshire, Pennsylvania, or South Carolina on Medicaid | Obesity coverage ended January 1, 2026. Check non-weight-loss indications or pivot to self-pay. |
| You lost coverage mid-treatment and you're already on the drug | Get your latest fill dispensed if possible; file a continuation appeal citing chronic disease management; set up a self-pay bridge at the same dose. |
| You have an HSA or FSA balance | Stack HSA/FSA dollars on whichever path you pick. |
| You've exhausted FDA-approved paths and want lower-cost alternatives | Read our separate compounded GLP-1 guide first — it's a different regulatory conversation. |
If You're Already on the Medication and Coverage Just Stopped
Coverage ending mid-treatment is its own category of problem. You have three jobs: protect the fill you have, file a continuation appeal if the denial is appealable, and set up a self-pay bridge at your current dose so you don't interrupt therapy.
- Don't skip the step you already took. If you still have refills on your existing prescription, call the pharmacy before coverage cuts off and ask whether you can fill one more month.
- Ask for the exact document triggering the change. If it's a benefit exclusion, your employer or plan administrator should have notification. If it's a utilization management change, it may be appealable.
- File a continuation appeal if the denial is a PA denial, not an exclusion. Studies show most people regain weight after discontinuing GLP-1s; that fact supports a continuation appeal framed around chronic disease management.
- Bridge with self-pay at your current dose. Line up LillyDirect or NovoCare ahead of time so you don't miss a dose. Note: you can't use a manufacturer commercial savings card if you're on Medicare, Medicaid, or TRICARE.
- If you're on Medicare and just lost coverage, see whether the CV risk reduction (Wegovy) or OSA (Zepbound) indications fit — those go through normal Part D coverage, not the Bridge.
Medicare, Medicaid, and Employer Plans
Medicare currently cannot cover GLP-1s for weight loss alone under federal statute, but the CMS Medicare GLP-1 Bridge will cover Wegovy, Foundayo, and the Zepbound KwikPen at $50/month for eligible Part D beneficiaries from July 1, 2026 through December 31, 2027. Medicaid coverage depends entirely on your state. Employer plans are the wildcard.
Medicare Part D
Medicare is statutorily prohibited from covering drugs used purely for weight loss. Three pathways exist in 2026:
Pathway 1: On-label non-weight-loss uses, available now. Your Part D plan may cover Wegovy for cardiovascular risk reduction, Wegovy for MASH, or Zepbound for OSA if you have the qualifying diagnosis.
Pathway 2: The Medicare GLP-1 Bridge, starting July 1, 2026. The Bridge provides $50/month copay access to Wegovy, Foundayo, and the Zepbound KwikPen. Eligibility requires one of three tiers:
- Tier 1: BMI ≥35 alone
- Tier 2: BMI ≥30 with heart failure with preserved ejection fraction, uncontrolled hypertension, or chronic kidney disease stage 3a or higher
- Tier 3: BMI ≥27 with prediabetes, prior myocardial infarction, prior stroke, or symptomatic peripheral artery disease
Timeline: The Bridge runs July 1, 2026 through December 31, 2027 (extended April 21, 2026 when CMS announced the permanent BALANCE Model would not launch in 2027 as originally planned). Verify current dates at cms.gov/medicare before relying on a specific date.
What to do now: Talk to your prescriber before July 1 so the prior authorization is ready to submit on day one. The Bridge runs through December 2027 — no plan opt-in required. BALANCE will not launch for Medicare Part D in 2027. Watch for BALANCE 2028 announcements during fall 2027 open enrollment (October 15 – December 7, 2027).
Medicaid (state-by-state)
Roughly 13 states covered GLP-1s for obesity as of early 2026 — down from 16 in 2025. Four states eliminated obesity coverage effective January 1, 2026:
- California (Medi-Cal): Wegovy, Zepbound, and Saxenda removed for weight-loss indications as of January 1, 2026. Important carve-outs still exist: Wegovy can still be covered for noncirrhotic MASH and may be submitted for cardiovascular disease; Zepbound PA requests may be considered for OSA; members under age 21 can still seek coverage under EPSDT.
- New Hampshire — eliminated obesity coverage January 1, 2026
- Pennsylvania — eliminated obesity coverage January 1, 2026 while continuing diabetes coverage
- South Carolina — eliminated obesity coverage January 1, 2026
Employer-sponsored plans
Per the KFF 2025 Employer Health Benefits Survey: 16% of firms with 200–999 workers, 30% of firms with 1,000–4,999 workers, and 43% of firms with 5,000+ workers covered GLP-1 agonists for weight loss in 2025. About 19% of large firms (200+) covered them overall.
Ask HR for these specific documents:
- The Summary Plan Description (SPD), with the weight-management benefit language highlighted
- Whether the plan is self-funded or fully insured (changes your appeal options)
- Whether an exception process exists for specific diagnoses
- When the plan year renews and what's changing at renewal
ACA Marketplace and Individual Plans
Marketplace and individual plans rarely cover GLP-1s for weight loss. When they do, it's usually for type 2 diabetes or for the on-label CV or OSA indications described above. Your realistic moves if your plan dropped coverage at renewal: (1) see whether a different Marketplace plan in your state covers GLP-1s at Open Enrollment, (2) use the CV/OSA/MASH pathways if any apply to you, or (3) go self-pay.
Using HSA or FSA Funds to Stack Savings
FDA-approved GLP-1 medications are HSA- and FSA-eligible when prescribed for a diagnosed medical condition. Under IRS Publication 502, prescription medicines for diagnosis, treatment, or prevention of disease qualify. 2026 HSA limits: $4,400 (individual) and $8,750 (family), with a $1,000 catch-up for 55+; FSA contributions are capped at $3,400.
Paying cash with HSA or FSA dollars gives you an effective 22–37% discount depending on your tax bracket. A $349 Wegovy fill costs roughly $245 in after-tax-equivalent dollars if you're in a 30% combined marginal bracket.
- HSAs are lenient at point-of-sale but you keep the Letter of Medical Necessity in case of audit (3-year IRS window).
- FSAs usually require the LMN at claim submission — check with your plan administrator.
Compounded GLP-1 Is a Different Regulatory Conversation
Compounded semaglutide and tirzepatide are not FDA-approved and have not been reviewed by the FDA for safety, efficacy, or manufacturing quality. If an FDA-approved path is financially accessible to you through any of the sections above, FDA-approved is the safer default.
If you're considering a compounded path anyway, you should know:
- Compounded GLP-1s are not FDA-reviewed for safety, efficacy, or quality
- Quality varies between compounding pharmacies (503A state-licensed and 503B outsourcing facilities operate under different regulatory conditions)
- The FDA has issued safety communications about fraudulent compounded GLP-1 products
- Cancellation and billing friction is more common in this lane — read terms carefully
Because the compounded lane has its own providers, regulatory nuances, and pricing dynamics, we keep it in a separate guide rather than mixing it with FDA-approved options here.
Read The Compounded GLP-1 Decision Guide →What Real Patients Say
Three attributed service reviews included to illustrate user experience, not typical medical results. Material affiliate relationship is disclosed below.
"did the paperwork for the pre authorization for my insurance"
— Lauren Kearns, Trustpilot review of Ro, March 25, 2026
"accessible care for people without insurance"
— Annalyese Zepeda, Trustpilot review of Sesame, March 12, 2026
"You aren't paying $145 for the medication"
— Matthew Vermeern, Trustpilot review of Ro, March 25, 2026. We included this one because it captures the most common complaint about Ro: the membership fee is separate from the medication cost. Go in knowing that and you won't be surprised at checkout.
Disclosure: The RX Index earns affiliate compensation when readers start programs through Ro, Sesame, Embody, or MEDVi links on this page. Compensation does not affect the order of recommendations or the facts presented. Testimonials reflect individual user experiences and are not representative of typical medical results.
Frequently Asked Questions
What if my insurance doesn't cover weight-loss medication at all?
Your first move is to decode whether it's a denial (appealable — the plan reviewed your specific request and said no) or an exclusion (not appealable — the plan removed the whole category). Denials are worth appealing, especially if the reason is paperwork or step therapy. Exclusions require pivoting — either to an on-label non-weight-loss indication, to your employer's exception process, or to a self-pay path.
Is 'not a covered benefit' the same as a prior authorization denial?
No. A prior authorization denial means the plan reviewed your specific request and said no based on criteria — which you can usually appeal. 'Not a covered benefit' means the entire medication category has been excluded from the plan by design, and standard appeals generally will not move it.
Can I appeal if my insurance denies Wegovy, Zepbound, or Foundayo?
For most commercial plans, yes — you have internal appeal rights (typically 180 days to file) followed by external review rights if the internal appeal fails, per HealthCare.gov federal guidelines. Whether the appeal is worth filing depends on the denial reason. KFF's 2024 Medicare Advantage data found that when denied prior authorization requests were appealed, 80.7% were overturned fully or partially — but only 11.5% were ever appealed.
How much does Wegovy cost without insurance in 2026?
Verified April 23, 2026: the Wegovy pill starts at $149/month for the 1.5 mg and 4 mg doses through NovoCare (4 mg offer available through August 31, 2026), then $199/month; 9 mg and 25 mg doses are $299/month. Wegovy injection is $199/month for the first two new-patient fills through December 31, 2026, then $349/month for most doses and $399/month for HD.
How much does Zepbound cost without insurance in 2026?
Verified April 23, 2026: Zepbound single-dose vials and the Zepbound KwikPen through LillyDirect follow the same regular price ladder: $299 for 2.5 mg, $399 for 5 mg, $499 for 7.5 mg, $699 for 10 mg, $699 for 12.5 mg, and $699 for 15 mg. The 7.5 mg through 15 mg doses drop to $449/month when refilled within 45 days under the Zepbound Self Pay Journey Program.
How much does Foundayo cost without insurance in 2026?
Verified April 23, 2026: Foundayo through LillyDirect is $149 for 0.8 mg, $199 for 2.5 mg, $299 for 5.5 mg, $299 for 9 mg, $349 for 14.5 mg, and $349 for 17.2 mg per 30-day supply. The 14.5 mg and 17.2 mg doses drop to $299/month if refilled within 45 days under the Foundayo Self Pay Journey Program.
Can I get Wegovy covered through a cardiovascular indication if it's denied for weight loss?
Yes, if you have a documented diagnosis of cardiovascular disease and BMI ≥27. Wegovy's FDA-approved cardiovascular risk reduction indication is a separate coverage lane. On Medicare, this goes through your Part D plan's normal PA process — not the GLP-1 Bridge.
Can I get Zepbound covered through a sleep apnea indication if it's denied for weight loss?
Yes, if you have a documented sleep study showing moderate-to-severe OSA (AHI ≥15) and BMI ≥30. Zepbound's FDA-approved OSA indication is a separate coverage lane.
Does Medicare cover weight-loss medication?
Not for weight loss alone — federal law excludes this. Medicare Part D can cover Wegovy for CV risk reduction or MASH, and Zepbound for OSA, when those separate FDA-approved indications are met. The Medicare GLP-1 Bridge (July 1, 2026 through December 31, 2027) will cover Wegovy, Foundayo, and Zepbound KwikPen at $50/month for eligible Part D beneficiaries who meet the three-tier BMI and diagnosis criteria.
Does Medicaid cover Wegovy or Zepbound for weight loss?
It depends on your state. Roughly 13 states covered GLP-1s for obesity as of early 2026. California, New Hampshire, Pennsylvania, and South Carolina eliminated weight-loss coverage on January 1, 2026. Medicaid coverage for type 2 diabetes, and sometimes for on-label CV risk or OSA indications, generally continues.
Is Ro worth it if I already have a prescription?
Usually not, if cheapest cash price is your only criterion. Going direct to LillyDirect or NovoCare without a membership fee is cheaper when you already have a prescriber. Ro is worth it when you want someone to check and fight for insurance coverage, when you need ongoing clinician support, or when you don't yet have a prescriber for a GLP-1.
Can I use HSA or FSA when insurance won't cover my medication?
Yes. FDA-approved GLP-1 medications are HSA- and FSA-eligible when prescribed for a diagnosed medical condition, per IRS Publication 502. A Letter of Medical Necessity is typically required for FSA claims. 2026 HSA limits are $4,400 individual / $8,750 family (plus $1,000 catch-up for 55+); FSA is capped at $3,400.
What documents do I ask HR or my insurer for?
Three documents close most of the uncertainty: (1) the Summary Plan Description (SPD) with the weight-management benefit language, from HR or your benefits portal; (2) the exact denial letter with the cited denial code and clinical criteria, from your insurer; (3) the plan's medical necessity criteria for the specific medication, also from your insurer. If you're on a self-funded plan, also ask HR whether the plan includes a GLP-1 rider or exception process.
Should I switch to compounded semaglutide or tirzepatide?
Only after weighing the regulatory trade-off. Compounded GLP-1s are not FDA-approved and have not been reviewed by the FDA for safety, efficacy, or manufacturing quality. The FDA has issued safety communications about compounded GLP-1 products as national supply has stabilized. If you're considering this path, read our dedicated compounded GLP-1 decision guide before choosing a provider.
Still Not Sure Which Path Fits You?
You've read the decoder. You've seen every realistic option. If you're still not sure which one is right for you, take our free 60-second matching quiz. We ask about your insurance, your denial letter wording, your budget, and your medical history, and we match you to the path that actually fits. No email required to see your result.
Take the Free GLP-1 Matching Quiz →Related guides
- How to Appeal a GLP-1 Insurance Denial (2026)
- GLP-1 Cost Without Insurance: 17 Real Prices (2026)
- How to Get GLP-1 Without Insurance from $149/mo
- Cheapest Zepbound Without Insurance: Real Prices by Dose
- GLP-1 Letter of Medical Necessity: 6-Point Checklist
- Compounded GLP-1 Decision Guide: What to Know Before Choosing
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We don't sell medications, issue prescriptions, or provide medical advice. Information on this page is editorial, was verified on , and will be re-verified monthly. For urgent medical questions, call your prescriber or 911.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup