CMS BALANCE Model Participating Plans: Status, Plan List, and What to Do Next (April 2026)
By The RX Index Editorial Team · Last verified: · Sources: CMS BALANCE, CMS Medicare GLP-1 Bridge, KFF, AHA News
Status snapshot — the three things you actually came to find
- Part D BALANCE participating plan list: Not available for 2027. CMS paused the Medicare Part D component on April 21, 2026.
- Medicare GLP-1 Bridge: Opens July 1, 2026 → runs through December 31, 2027. Your Part D plan does not need to opt in.
- Bridge copay: $50/month for eligible beneficiaries on Wegovy®, Zepbound® KwikPen®, or Foundayo®.
If you came here looking for a clean list of CMS BALANCE Model participating plans, here's what nobody is telling you straight: that list doesn't exist for Medicare Part D — and it's not going to for 2027. The Centers for Medicare & Medicaid Services (CMS) paused the Medicare Part D component of the BALANCE Model on April 21, 2026, seven days before this page was last verified. CMS's projected 80% participation threshold wasn't met. The Medicaid component is still moving forward.
Here's the part that actually changes your life. The Medicare GLP-1 Bridge — the $50-a-month program covering Wegovy, the Zepbound KwikPen, and Foundayo for weight loss — was just extended through December 31, 2027. And your Part D plan doesn't have to "join" anything for you to use it. CMS administers the Bridge directly, outside the regular Part D system, through a single central processor (Humana, working through the LI NET infrastructure that already exists). You don't need to switch plans during Open Enrollment to "qualify for BALANCE." You couldn't even if you wanted to.
So if you came expecting a plan list, you're getting something more useful: the actual answer, an honest tracker of what's live and what's paused, and a clear next step based on whether you're on Medicare, Medicaid, or neither.
| You searched for | Current answer (April 28, 2026) | Source | Your next step |
|---|---|---|---|
| CMS BALANCE Model participating plans | No actionable Part D list for 2027 | CMS BALANCE | Check Bridge eligibility — no BALANCE plan switching needed |
| Medicare GLP-1 Bridge participating plans | No plan opt-in required; works in most Part D plan types | CMS Bridge FAQ | Confirm you're in an eligible plan type |
| Which Part D plan covers $50 GLP-1s? | Bridge runs outside Part D — your plan isn't the gatekeeper | CMS Bridge FAQ | Ask your prescriber about the central-processor PA |
| Medicaid BALANCE participating states | State-by-state — applications open through July 31, 2026 | AHA News | Check your state Medicaid bulletins |
| What if I'm not on Medicare or Medicaid? | Bridge/BALANCE don't apply to you | — | Check FDA-approved self-pay paths instead |
Find your CMS GLP-1 path in 60 seconds.
Based on your insurance type, state, medication, and situation. No signup. No email.
Take the Free Path Checker →Are there CMS BALANCE Model participating plans right now?
No.
As of , there is no Medicare Part D plan list participating in the BALANCE Model for 2027 because CMS announced an indefinite delay of the Part D component on April 21, 2026 after the projected 80% participation threshold wasn't met. The Medicare GLP-1 Bridge — a separate, CMS-administered demonstration — is the access path through December 31, 2027, and it doesn't require plan opt-in.
We want to make this part really clear because there's a lot of misinformation floating around right now: pages telling you to switch Part D plans for “BALANCE access,” brokers selling 2027 plans on the promise of $50 GLP-1s, news articles dated December 2025 that make it sound like January 1, 2027 is going to be a bright line moment for Medicare obesity coverage. None of that is the current reality.
What the April 21, 2026 CMS memo actually said
CMS sent the announcement to plan sponsors via a Health Plan Management System (HPMS) email — the channel the agency uses for binding operational guidance to Medicare plan sponsors. As reported by AHA News and confirmed by Avalere Health, the substance was clear: the Part D leg of BALANCE will not launch in calendar year 2027 “pending further evaluation and data collection.” Plan sponsors were specifically instructed not to indicate BALANCE participation in HPMS or in their Bid Pricing Tool submissions for CY 2027.
In plain English: there is no plan list to publish because there are no participating plans to put on it.
The Medicare GLP-1 Bridge, originally scheduled to end December 31, 2026, was simultaneously extended through December 31, 2027 — giving Medicare beneficiaries continuous access to FDA-approved weight-loss GLP-1s at $50 per month for an additional 12 months while CMS rethinks Part D-based coverage.
The 80% threshold — and why most insurers walked away
CMS conditioned the Part D launch on a “critical mass” of plan participation. The 80% threshold was an enrollment-weighted calculation: projected beneficiary enrollment in applying Part D plans, divided by total Part D enrollment (the RFA excluded SNPs and EGWPs from the threshold math even though those plans were eligible to participate). Applications closed April 20, 2026. The threshold was missed.
Industry analysis from Avalere Health and Optum / Advisory Board points to several drivers:
- Bid timing pressure. Part D bids for 2027 were due June 1, 2026 — leaving plans roughly six weeks after the application deadline to model the financial impact of expanded GLP-1 coverage. With no historical claims data on weight-loss GLP-1 use in Part D (because Medicare has been statutorily prohibited from covering weight-loss drugs since 2003), plans had no reliable way to project utilization or premium impact.
- Adverse selection risk. A plan that opted in might attract a disproportionate share of beneficiaries seeking GLP-1 coverage, concentrating cost without offsetting revenue.
- Maximum Fair Price (MFP) overlap. Semaglutide products (Ozempic, Rybelsus, Wegovy) are on the Medicare Drug Price Negotiation Program list with MFPs taking effect in 2027. The interaction between BALANCE pricing and MFP pricing required statutory waivers that didn't fully resolve plans' accounting concerns.
The result: enough plans declined that CMS couldn't launch the model.
Don't waste time hunting for a list — here's the path that actually exists
If you've been calling Part D plans asking whether they “joined the Bridge” or whether they're a “BALANCE plan,” save the phone time. The Bridge is administered directly by CMS through Humana as the central processor; plans don't opt in. Your Part D enrollment matters for one reason: you have to be in an eligible plan type to qualify for Bridge access (we cover this exactly below). Beyond that, your individual plan has no role in approving, denying, or processing your Bridge prescription.
See if the Bridge fits your situation in 60 seconds.
Use the Free Path Checker →Covers your insurance type, state, medication, and what to do this week.
Does my Part D plan have to opt in to the Medicare GLP-1 Bridge?
No.
CMS says Part D sponsors do not have to opt in for eligible beneficiaries to access Bridge-covered drugs. The Bridge operates outside the Medicare Part D benefit's normal coverage and payment flow, administered directly by CMS through a single central processor (Humana, working through the LI NET infrastructure).
This is the single most misunderstood thing about how the Bridge works, and it's where you can stop searching the second you internalize it. There is nothing your Part D plan needs to do for you to access $50/month Wegovy, Zepbound KwikPen, or Foundayo if you qualify. The plan is not the gatekeeper. CMS is.
What still matters is your plan type:
✓ Eligible plan types
- ✓Standalone Prescription Drug Plan (PDP)
- ✓Medicare Advantage with Part D (MA-PD) — HMO, HMOPOS, Local PPO, Regional PPO
- ✓Special Needs Plans (SNPs)
- ✓Employer/Union Group Waiver Plans (EGWPs)
- ✓LI NET program
- ✓Dual-eligible (if also in an eligible Part D plan type)
✗ Not eligible plan types
- ✗Private fee-for-service plans (unless also in a standalone PDP)
- ✗Section 1876 cost contract plans (unless also in standalone PDP)
- ✗Section 1833 health care prepayment plans (unless also in standalone PDP)
- ✗PACE organizations (unless also in standalone PDP)
- ✗Fallback plans
- ✗Religious fraternal benefit plans (unless also in standalone PDP)
Beyond plan type, what matters is your eligibility under one of the three BMI/diagnosis tiers (covered below), the specific drug and formulation prescribed, and the prior authorization route. None of that runs through your Part D plan.
What changed on April 21, 2026 — the pause and the Bridge extension
On April 21, 2026, CMS paused the Medicare Part D component of the BALANCE Model for 2027 and extended the Medicare GLP-1 Bridge through December 31, 2027. The Medicaid component of BALANCE continues on its original schedule, with state applications open through July 31, 2026 and start dates between May 1, 2026 and January 1, 2027. Manufacturer agreements with Eli Lilly and Novo Nordisk remain in place.
| Item | Original CMS plan (Dec 2025 – early 2026) | Current status (April 28, 2026) | Practical effect for you | Source |
|---|---|---|---|---|
| Medicare Part D BALANCE | Launch January 1, 2027 | Paused indefinitely for CY 2027 | No 2027 BALANCE plan to switch into | CMS BALANCE |
| Medicare GLP-1 Bridge | July 1, 2026 → December 31, 2026 (6 months) | July 1, 2026 → December 31, 2027 (18 months total) | 12 extra months of $50/month access | CMS Bridge FAQ |
| Bridge → BALANCE transition | Switch Part D plans during 2026 Open Enrollment | No plan switching required for weight-loss GLP-1 access | Choose your 2027 Part D plan based on your other meds | CMS Bridge FAQ |
| Medicaid BALANCE | Rolling state launch May 2026 → January 2027 | On schedule | State decisions still pending; check your state | AHA News |
| Manufacturer agreements (Lilly, Novo) | $245 net price/month for 2027 model drugs | Still executed | Pricing locked for participating channels | KFF brief |
| Bridge $50 copay | Set in March 2026 FAQ | No change | $50/month if you qualify | CMS Bridge FAQ |
| Drug Price Negotiation MFP for Ozempic/Rybelsus/Wegovy | Effective January 1, 2027 | Independent — still effective | Affects diabetes/CV pricing separately | AAF analysis |
The pause is significant but it isn't a cancellation. CMS's language — “pending further evaluation and data collection” — leaves the door open. The CY2028 Advance Notice, which CMS typically releases in January or February of the prior year, is the document to watch. If BALANCE language reappears there in substantive form, expect a relaunch attempt for plan year 2028.
Why this is actually better news for most beneficiaries than it sounds
This is the part that gets buried in the technical coverage. Under the original BALANCE plan:
- •The Bridge was supposed to end December 31, 2026.
- •To keep weight-loss GLP-1 coverage in 2027, you would have needed to be enrolled in a Part D plan that opted into BALANCE — meaning many people would have had to switch plans during Open Enrollment, with all the disruption that brings for non-GLP-1 medications, network pharmacies, and premiums.
- •If your plan didn't join, you'd have lost coverage on January 1.
Under the post-April-21 reality:
- ✓The Bridge runs through December 31, 2027 — 12 extra months of $50/month access.
- ✓You don't have to switch plans for 2027 to keep weight-loss GLP-1 coverage.
- ✓Your 2027 Part D plan choice can be based on what actually matters: how it covers your other medications.
There's a real downside — the Bridge is narrower than BALANCE would have been (Wegovy, Zepbound KwikPen, and Foundayo only), and the $50 copay doesn't count toward your Part D out-of-pocket cap. Both of those things would have been better under BALANCE. But on the question of whether your existing access continues, the extension is a quiet win.
Bridge vs. BALANCE vs. regular Part D — the only comparison you need
The Medicare GLP-1 Bridge is the active access path. Medicare Part D BALANCE is paused. Regular Part D continues to apply for GLP-1s prescribed for currently coverable indications like type 2 diabetes, cardiovascular risk reduction, or obstructive sleep apnea. These are three separate access paths with different rules, different drug lists, and different paperwork.
| Feature | Medicare GLP-1 Bridge | Medicare Part D BALANCE | Regular Medicare Part D |
|---|---|---|---|
| Status (April 28, 2026) | Opens July 1, 2026 → Dec 31, 2027 | Paused for CY 2027 | Active (year-round) |
| Who runs it | CMS, via Humana central processor | Would have been your Part D plan | Your Part D plan |
| Plan opt-in required? | No — works regardless of which Part D plan | Was voluntary; threshold not met | N/A — your plan is already in |
| Drug list | Wegovy (injection + tablets), Zepbound KwikPen, Foundayo | Was Mounjaro, Ozempic, Rybelsus, Wegovy, Zepbound KwikPen, Foundayo | Plan-specific formulary |
| Use case | Weight loss only | Was weight loss + lifestyle support | Type 2 diabetes, CV risk, OSA, other coverable indications |
| Patient cost | Flat $50/month | Was tiered: $50 enhanced/EGWP, $125 basic, $245 deductible | Plan-specific; tiered, deductible-dependent |
| Counts toward Part D out-of-pocket cap (TrOOP)? | No — outside Part D | Would have counted | Yes |
| LIS / Extra Help applies? | No — Bridge is outside the benefit | Would have applied | Yes |
| Manufacturer coupons / discount cards? | Cannot be applied to Bridge claims | Would have followed Part D rules | Plan-specific |
| Prior authorization route | CMS central processor (BIN 028918 / PCN MEDDGLP1BR) | Would have been your plan | Your plan |
| Authority | Section 402(a)(1)(A) demonstration | Section 1115A CMMI model | Standard Part D statute |
Sources: CMS Medicare GLP-1 Bridge FAQ; CMS BALANCE Part D RFA; KFF brief.
The distinction that matters most: the Bridge is the only path to Medicare coverage of GLP-1s prescribed solely for weight loss. If your prescription is for a currently coverable indication — Ozempic for type 2 diabetes, Wegovy for cardiovascular risk reduction in adults with established cardiovascular disease, Zepbound for obstructive sleep apnea in adults with obesity — that prescription goes through your regular Part D plan, with your regular plan's prior authorization and copay. The Bridge isn't relevant to those prescriptions.
For the deeper how-it-works mechanics of the Bridge:
Eligibility tiers, doctor visit checklist, pharmacy details, and timing — all in one guide.
Read our full Medicare GLP-1 Bridge guide →Which GLP-1 medications are covered (and which are NOT)
The Medicare GLP-1 Bridge covers Wegovy® injection, Wegovy® tablets, Zepbound® KwikPen®, and Foundayo® for eligible weight-management use. It does NOT cover Zepbound single-dose vials or pens, Ozempic, Mounjaro, Rybelsus, Saxenda, or any compounded GLP-1. Brand and formulation matter — getting this wrong is the most common reason beneficiaries get blindsided at the pharmacy counter.
Source: CMS Medicare GLP-1 Bridge FAQ, last updated April 6, 2026 (Foundayo was added after FDA approval; the FAQ also clarified that only the KwikPen formulation of Zepbound is included).
Bridge formulation eligibility matrix
| Brand | Active ingredient | Formulation | Bridge status |
|---|---|---|---|
| Wegovy® | Semaglutide | Injection (all approved doses) | ✅ Covered |
| Wegovy® tablets | Semaglutide | Oral tablet | ✅ Covered |
| Zepbound® KwikPen® | Tirzepatide | KwikPen device | ✅ Covered |
| Foundayo® | Orforglipron | Oral tablet (all approved doses) | ✅ Covered (added April 6, 2026) |
| Zepbound® single-dose vial | Tirzepatide | Vial | ❌ NOT covered |
| Zepbound® single-dose pen | Tirzepatide | Pen (non-KwikPen) | ❌ NOT covered |
| Ozempic® | Semaglutide | Injection | ❌ Not Bridge-eligible (coverable through regular Part D for type 2 diabetes / CV / CKD) |
| Mounjaro® | Tirzepatide | Injection | ❌ Not Bridge-eligible. Only Zepbound KwikPen (the weight-management tirzepatide brand) is covered. |
| Rybelsus® | Oral semaglutide | Oral tablet | ❌ Not Bridge-eligible (coverable through regular Part D for type 2 diabetes) |
| Saxenda® | Liraglutide | Injection | ❌ Not on Bridge list |
| Compounded semaglutide / tirzepatide | — | — | ❌ Not eligible. Only listed FDA-approved branded medications covered. |
The Ozempic question we have to answer every week
We get asked this constantly: “Ozempic and Wegovy contain the same active ingredient — can I get Ozempic through the Bridge if my doctor prescribes it?” No. Despite the same active molecule (semaglutide), Ozempic and Wegovy are different FDA-approved products with different approved indications, different dosing structures, and different NDC numbers. The Bridge drug list is by NDC. Ozempic for weight loss isn't Bridge-eligible because Ozempic isn't FDA-approved for weight loss.
If you have type 2 diabetes and your prescription for Ozempic is for that indication, you don't need the Bridge — your regular Part D plan covers it (subject to its formulary and prior authorization rules). That's actually a more flexible path because it counts toward your Part D out-of-pocket cap.
Bridge NDC reference (for your pharmacy if they're new to this)
If your pharmacist hasn't seen the Bridge yet, hand them this.
| Brand | NDC numbers |
|---|---|
| Wegovy | 0169-4525-14, 0169-4505-14, 0169-4501-14, 0169-4517-14, 0169-4524-14, 0169-4415-31, 0169-4404-31, 0169-4409-31, 0169-4425-31, 0169-4572-14 |
| Zepbound KwikPen | 0002-3566-11, 0002-3555-11, 0002-3544-11, 0002-3533-11, 0002-3522-11, 0002-3511-11 |
| Foundayo | 0002-4178-31, 0002-4503-31, 0002-4794-31, 0002-4803-31, 0002-4839-31, 0002-4953-31 |
Source: CMS Medicare GLP-1 Bridge FAQ, last updated April 6, 2026.
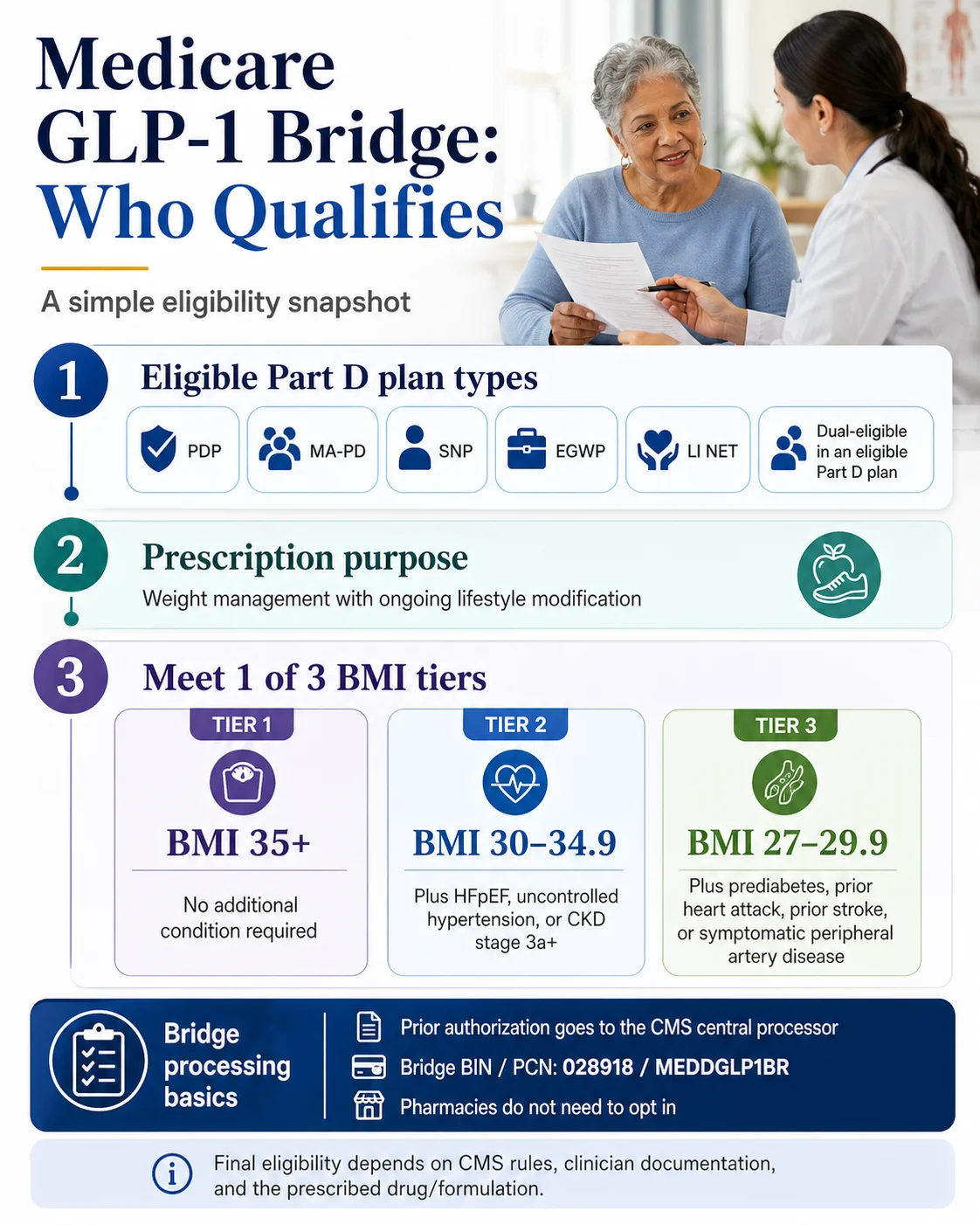
Who qualifies for the Medicare GLP-1 Bridge — the three BMI pathways
To qualify for the Medicare GLP-1 Bridge, you must (1) be enrolled in an eligible Medicare Part D plan type, (2) be prescribed an eligible GLP-1 specifically for weight loss with ongoing lifestyle modification, and (3) meet one of three BMI/diagnosis tiers published in the CMS Bridge FAQ. You only need to meet one tier.
The three eligibility tiers
BMI 35+
None — BMI alone qualifies
BMI 30–34.9
Plus HFpEF, uncontrolled hypertension (systolic >140 or diastolic >90 while on ≥2 antihypertensives), or CKD stage 3a+
BMI 27–29.9
Plus prediabetes (ADA criteria), prior MI, prior stroke, or symptomatic peripheral artery disease
Source: CMS Medicare GLP-1 Bridge FAQ.
A few details competing pages routinely get wrong:
⚠ BMI is measured at GLP-1 initiation, not at the time of the prior authorization. If you've already started losing weight, your starting BMI is what counts.
⚠ Controlled hypertension does not qualify under Tier 2. It must specifically be uncontrolled blood pressure despite already being on at least two antihypertensive medications.
⚠ Tier 3 conditions are specific. “Prediabetes” follows ADA diagnostic criteria. “Heart attack” and “stroke” must be documented. “Symptomatic peripheral artery disease” is a clinical diagnosis — not just claudication mentioned in passing.
Quick BMI reference
| Height | BMI 27 (Tier 3) | BMI 30 (Tier 2) | BMI 35 (Tier 1) |
|---|---|---|---|
| 5'2" | ~148 lbs | ~164 lbs | ~191 lbs |
| 5'4" | ~157 lbs | ~174 lbs | ~204 lbs |
| 5'6" | ~167 lbs | ~186 lbs | ~217 lbs |
| 5'8" | ~177 lbs | ~197 lbs | ~230 lbs |
| 5'10" | ~188 lbs | ~209 lbs | ~244 lbs |
| 6'0" | ~199 lbs | ~221 lbs | ~258 lbs |
The doctor visit cheat sheet
Bring this to your appointment so the prior authorization gets submitted correctly the first time. Common denials trace back to incomplete documentation in the chart at the time of the PA request.
- ✓Your current Medicare drug coverage type (PDP, MA-PD, SNP, EGWP, dual-eligible, LI NET).
- ✓Your medication preference (Wegovy injection, Wegovy tablets, Zepbound KwikPen, or Foundayo).
- ✓Your BMI at the time you intend to start the medication.
- ✓Documentation of your qualifying condition (Tier 2 or Tier 3 only).
- ✓Confirmation that the prescription is for weight loss with ongoing lifestyle modification (CMS-required attestation).
- ✓A note for your prescriber: the prior authorization goes to the CMS central processor, not to your Part D plan.
See if you'd qualify in 60 seconds.
Covers Bridge eligibility, plan-type fit, drug coverage, and what to ask your prescriber.
Use Our Medicare GLP-1 Path Checker →How prior authorization actually works (and why your Part D plan isn't involved)
For weight-loss prescriptions covered by the Bridge, your prescriber submits the prior authorization to the CMS central processor — Humana, working through the LI NET infrastructure — not to your Part D plan. Your pharmacy bills the central processor using BIN 028918 and PCN MEDDGLP1BR. Your $50 copay is what you owe. For a properly routed Bridge claim, your Part D plan does not approve, deny, or adjudicate the claim.
This is the part that breaks the most pharmacist and provider workflows in the early days — the muscle memory is to send everything to a Part D plan. The Bridge changes the address.
The Bridge claim workflow, step by step
- 1
You confirm eligible plan type: PDP, MA-PD, SNP, EGWP, LI NET, or dual-eligible enrolled in one of the above.
- 2
Your provider confirms BMI/diagnosis criteria — one of the three tiers from the previous section.
- 3
Your provider writes the prescription for an eligible drug (Wegovy injection or tablets, Zepbound KwikPen, or Foundayo) for weight management.
- 4
Your provider submits the prior authorization to the CMS central processor — not to your Part D plan. CMS will release the specific submission portal details in spring 2026; your provider should monitor CMS guidance leading up to July 1, 2026.
- 5
Your pharmacy bills the Bridge using BIN 028918 and PCN MEDDGLP1BR. The pharmacy collects your $50 copay and is reimbursed through the Bridge claims process; participating manufacturers provide eligible Bridge drugs at a $245 net price per monthly supply under CMS terms.
- 6
You pick up your medication and continue with lifestyle modification as part of the program's core requirement.
When PA goes to your Part D plan instead of the central processor
The Bridge is specifically for weight-loss-only prescriptions. If your prescriber writes the GLP-1 for an indication that's already coverable under regular Part D — Zepbound for obstructive sleep apnea in adults with obesity, or Wegovy for cardiovascular risk reduction — the prior authorization follows your plan's normal process. Same drug, different paperwork, depending on what your prescription says.
The Bridge troubleshooting table
| If this happens | Likely cause | Who to call | What to say |
|---|---|---|---|
| Pharmacy says “drug is not on formulary” | They billed your Part D plan instead of the Bridge | Pharmacist | “This is a Medicare GLP-1 Bridge claim. Please bill BIN 028918, PCN MEDDGLP1BR, not my Part D plan.” |
| Part D plan denies the weight-loss prescription | Plan was sent the PA in error | Your prescriber's office | “Please resubmit the prior authorization to the CMS Bridge central processor, not to my Part D plan.” |
| Pharmacy doesn't recognize BIN 028918 | Bridge is new; operational guidance still rolling out | Pharmacy manager | “CMS established BIN 028918 / PCN MEDDGLP1BR for the Medicare GLP-1 Bridge. CMS guidance is on the Medicare GLP-1 Bridge page.” |
| Plan rep says “we don’t participate in the Bridge” | Common misunderstanding | Plan rep | “Plans don't have to participate. CMS administers the Bridge through a central processor. My access doesn't run through your plan.” |
| You're told you must be a Humana plan member | Confusion between Humana's processor role and plan enrollment | Pharmacy or plan rep | “Humana administers the Bridge for all eligible beneficiaries. I don't need to be a Humana plan member to use it.” |
| Pharmacy tries to apply a manufacturer coupon | Standard reflex; not allowed on Bridge claims | Pharmacist | “CMS doesn't permit coupons or discount programs on Bridge claims. Please process at the $50 copay only.” |
What it costs — and the LIS gotcha that affects low-income enrollees
Bridge cost in plain numbers
Beneficiary copay
$50 per 30-day supply
Same for everyone, regardless of income.
Manufacturer net price
$245 per 30-day supply
Under CMS-negotiated Bridge terms.
TrOOP impact
None
Bridge spend doesn't count toward your Part D out-of-pocket cap ($2,100 in 2026, $2,400 in 2027).
LIS / Extra Help
Not applicable to Bridge
Even full LIS pays the full $50 on Bridge claims.
Manufacturer savings cards
Not applicable
Coupons and discount programs cannot be applied to Bridge claims.
HSA/FSA reimbursement
Check with your administrator
Eligibility can depend on plan rules and documentation.
The damaging admission about the Bridge — and the upside
We're going to be straight with you: the Bridge is narrower than a fully launched BALANCE Model would have been. Under BALANCE, if it had launched in Part D for 2027 as planned:
- ✗The drug list would have been broader (Mounjaro, Ozempic, Rybelsus added to Wegovy / Zepbound KwikPen / Foundayo).
- ✗Cost-sharing would have integrated with the Part D out-of-pocket cap, meaning your spend would have helped you reach the $2,400 catastrophic threshold.
- ✗Low-income beneficiaries with LIS would have received their normal cost-sharing reductions.
The Bridge doesn't do any of those three things. But here's what the Bridge does do that BALANCE-2027 wouldn't have: it works regardless of which Part D plan you're in. It runs through December 31, 2027. It doesn't require you to switch plans during Open Enrollment. For most beneficiaries, that trade — narrower drug list and no TrOOP credit, in exchange for not having to switch plans and 12 extra months of access — works out fine.
What about the $1,600 figure people quote
A common pattern in public Medicare-focused forum threads: a beneficiary's doctor prescribes the Wegovy pill, the Part D plan denies it, and the cash-pay quote is around $1,600/month. That denial happens because regular Part D still excludes weight-loss-only prescriptions under the 2003 statute. The Bridge is the answer for a weight-loss-only Wegovy prescription starting July 1, 2026. If that beneficiary qualifies under one of the three BMI tiers, they go from a $1,600/month list price to a $50 copay — a $1,550 monthly difference. That's the size of the access change the Bridge is making for the people it covers.
What individual insurers actually said — the public statement tracker
| Insurer | Bridge role | BALANCE stance (pre-pause) | What this does NOT prove | Source / date |
|---|---|---|---|---|
| UnitedHealthcare | Confirmed: will participate in the Bridge | Was actively working toward BALANCE participation; flagged "notable challenges" | Bridge access for any beneficiary; the Bridge doesn't require plan opt-in | ReutersApril 21, 2026 |
| CVS Health (Aetna) | Status not publicly confirmed | Did not opt in to BALANCE before the April 20 deadline | Anything about Aetna's regular Part D coverage decisions | ReutersApril 21, 2026 |
| Humana | Serves as Bridge central processor (administrative) | Stance not publicly confirmed | Plan exclusivity — you don't need to be a Humana enrollee to use the Bridge | CMS Bridge FAQ |
| Cigna / Express Scripts | Status not publicly confirmed | Status not publicly confirmed | — | Last searched April 28, 2026 |
| Elevance Health (Anthem) | Status not publicly confirmed | Status not publicly confirmed | — | Last searched April 28, 2026 |
| Kaiser Permanente | Status not publicly confirmed | Status not publicly confirmed | — | Last searched April 28, 2026 |
| Centene | Status not publicly confirmed | Status not publicly confirmed | — | Last searched April 28, 2026 |
Why the labels matter — and the editorial rule we follow on this page
- •A Bridge “participant” is meaningless in the sense most beneficiaries are looking for. The Bridge covers eligible beneficiaries regardless of which plan they’re in (provided the plan type is eligible). UnitedHealthcare saying they’ll participate in the Bridge is essentially a statement that they’re prepared operationally — but it doesn’t gate access for anyone else.
- •A “BALANCE participating plan” doesn’t currently exist because the Part D component isn’t launching. CVS/Aetna declining and UnitedHealthcare working toward “yes” both happened in a context where the model was still being negotiated; both became moot when CMS paused.
- •Humana’s central processor role is an administrative function, not a plan-coverage statement. You don’t have to be in a Humana plan to use the Bridge. Any pharmacist or insurance broker telling you otherwise is mistaken.
Which state Medicaid programs are participating in BALANCE
The Medicaid GLP-1 obesity coverage starting point (January 2026)
As of January 2026, 13 state Medicaid programs covered GLP-1s for obesity treatment under fee-for-service, down from 16 in October 2025, per KFF's analysis of 50-state Medicaid budget data. Four states removed coverage in early 2026: California, New Hampshire, Pennsylvania, and South Carolina. States that already cover obesity GLP-1s in Medicaid have a strong reason to apply to BALANCE because the negotiated supplemental rebates would lower their per-member cost.
How Medicaid BALANCE participation works (different from Medicare)
- •State agreements — Each participating state signs a State Agreement with CMS adopting standardized Medicaid Key Terms.
- •Supplemental rebate agreements — Participating states sign supplemental rebate agreements with each participating manufacturer, on top of statutory Medicaid Drug Rebate Program rebates.
- •Equal application — The Medicaid Key Terms apply equally in fee-for-service Medicaid and Medicaid managed care.
- •Floor, not ceiling — States cannot make eligibility more restrictive than the Key Terms but can offer broader coverage.
- •Member cost — Medicaid enrollees generally pay little or no copay for prescription drugs; the benefit is whether the drug is covered at all, not the copay amount.
- •Net pricing — The discounted Medicaid net price is confidential, not publicly disclosed.
State BALANCE participation tracker
| Region | Existing GLP-1 obesity coverage (Jan 2026) | BALANCE application status | Last verified |
|---|---|---|---|
| All 50 states + DC + territories | See KFF baseline — 13 states with FFS GLP-1 obesity coverage as of January 2026 | Status pending — applications due July 31, 2026; start dates May 1, 2026 – Jan 1, 2027 |
We commit to populating this table state-by-state as agreements are publicly executed. Most cells will read “Status pending” through May; we expect meaningful state announcements to begin in June and accelerate through July.
If you're on Medicaid and trying to plan, your single most useful action is calling your state Medicaid agency directly and asking whether they've applied to BALANCE for obesity coverage and when they expect a decision.
Want a head start on state-by-state Medicaid GLP-1 coverage today?
The existing coverage baseline you can act on now, while the BALANCE state applications process plays out.
See our GLP-1 Medicaid Coverage by State Guide →What to do during 2026 Medicare Open Enrollment (October 15 – December 7, 2026)
The 2027 Open Enrollment checklist (when BALANCE is paused)
- 1
Inventory your medications. Make a complete list of every prescription you currently take, including dose and frequency.
- 2
Use Medicare Plan Finder (medicare.gov/plan-compare) to compare plans on coverage of your full medication list. Plug in every drug. The total annual cost projection is what matters, not the headline monthly premium.
- 3
For your GLP-1, check the indication. If your GLP-1 is purely for weight loss, the Bridge covers it regardless of plan. If it's for a covered indication (diabetes, CV risk reduction), the formulary still matters.
- 4
Check pharmacy network. Your current pharmacy may not be preferred under your 2027 plan.
- 5
Ignore plan marketing claiming “BALANCE coverage.” No 2027 plan offers BALANCE-style integrated GLP-1 weight-loss coverage because BALANCE Part D didn’t launch. This is a red flag from any broker or plan-finder tool.
- 6
Confirm your 2027 plan type is Bridge-eligible. PDP, MA-PD, SNP, EGWP, dual-eligible, and LI NET are all eligible.
- 7
Don’t switch carriers solely based on Bridge participation rumors. The Bridge doesn’t require plan participation. Carriers can’t differentiate themselves on Bridge “exclusivity” because there is no exclusivity.
When you should call your plan vs. when you shouldn't
✓ Call your plan for:
- • Your formulary coverage of non-GLP-1 medications
- • Prior authorization rules for indication-based GLP-1 coverage (diabetes, CV, OSA)
- • Network pharmacy disputes
- • Appeal rights on Part D claims
✗ Don't call your plan for:
- • Bridge eligibility interpretation
- • Bridge prior authorization submission
- • Confirming whether you "got into BALANCE" — the answer is: there is no BALANCE plan to get into
What if you're not using Medicare Part D or Medicaid
The Medicare GLP-1 Bridge and the BALANCE Model only apply to people on government insurance (Medicare Part D or Medicaid). If you're on commercial insurance, uninsured, or self-paying — or you're under 65 without Medicare eligibility — your path runs through entirely different channels. (Note: Medicare isn't only for people 65+. People can qualify earlier due to disability, ESRD, or ALS. What determines whether the Bridge pathway applies is whether you're enrolled in eligible Medicare Part D or Medicaid coverage — not your age.)
The realistic options for people without Medicare or Medicaid:
- •Commercial insurance with weight-loss GLP-1 coverage. Some employer-sponsored plans cover Wegovy, Zepbound, or Foundayo for weight management with prior authorization. Coverage has tightened significantly in 2025 and 2026. Check your plan's formulary and PA criteria.
- •Manufacturer self-pay programs. LillyDirect (Zepbound, Foundayo, Mounjaro), NovoCare (Wegovy, Ozempic), and TrumpRx sell brand-name FDA-approved GLP-1s on a cash-pay basis without insurance involvement. Pricing varies by product and dose; verify each on the publish date before relying on a specific number.
- •HSA/FSA. Eligibility can depend on plan rules and documentation; check your administrator.
- •Telehealth providers with insurance concierge support. Telehealth platforms that prescribe FDA-approved GLP-1s and help with prior authorization or self-pay setup.
For the FDA-approved telehealth path with insurance concierge support:
For readers without straightforward employer coverage, Ro carries Zepbound® (tirzepatide) and Foundayo™ (orforglipron), runs a free GLP-1 Insurance Coverage Checker that contacts your specific commercial plan to verify coverage before you spend a dollar, and provides an insurance concierge that handles the prior authorization paperwork. Ro Body membership is $39 for the first month, $149/month ongoing, or as low as $74/month with annual prepay.
Not the right path for Medicare or Medicaid coverage questions.
Not sure where you fit?
Covers Medicare, Medicaid, commercial, and self-pay paths in one 60-second quiz.
Take the Free 60-Second GLP-1 Path Checker →What we actually verified for this page
This page was built from primary CMS sources, cross-checked against the most recent policy analyses and reputable trade reporting, with each claim tied to a named source and a date.
| Claim | Verified? | Primary source | Last checked |
|---|---|---|---|
| Medicare Part D BALANCE delayed for CY 2027 | ✅ | CMS BALANCE / AHA News / Avalere Health | |
| Bridge extended through December 31, 2027 | ✅ | CMS Bridge FAQ | |
| 80% projected enrollment threshold not met | ✅ | Becker's / Optum Advisory Board | |
| Bridge does not require Part D plan opt-in | ✅ | CMS Bridge FAQ | |
| Medicaid component continues; state applications due July 31, 2026 | ✅ | CMS BALANCE / AHA News | |
| Bridge drug list (Wegovy injection + tablets, Zepbound KwikPen, Foundayo) | ✅ | CMS Bridge FAQ (last updated April 6, 2026) | |
| Bridge $50 copay; $245 negotiated net price; no TrOOP credit; no LIS | ✅ | CMS Bridge FAQ / KFF Quick Take | |
| Humana serves as Bridge central processor; BIN 028918 / PCN MEDDGLP1BR | ✅ | CMS Bridge FAQ | |
| UnitedHealthcare Bridge / BALANCE statements | ✅ | UnitedHealth Q1 2026 earnings / Reuters | |
| CVS/Aetna BALANCE non-participation | ✅ | Reuters | |
| Specific 2027 Part D BALANCE plan list | ❌ Not available | Does not exist | |
| State-by-state Medicaid agreement executions | ⏳ In progress | Needs monthly verification through July 31, 2026 |
Refresh cadence — what we re-verify and how often
| Element | Cadence | Verification method |
|---|---|---|
| Part D BALANCE pause status / any relaunch | Monthly + on any HPMS memo or CMS announcement | CMS BALANCE page; AHA News; KFF |
| State Medicaid participation list | Twice monthly through July 31, 2026; monthly thereafter | State Medicaid bulletins; CMS Innovation Center |
| Plan sponsor public statements | Quarterly (earnings cycle) + on breaking news | Earnings transcripts; Reuters; Becker's |
| Bridge end date and successor plans | Quarterly | CMS Bridge FAQ |
| Bridge-eligible drug list and NDCs | Quarterly + on FDA approvals | CMS Bridge FAQ "last updated" date |
| Eligibility BMI tiers and clinical criteria | Quarterly | CMS Bridge FAQ |
| $50 copay and $245 net price | Quarterly + on negotiated changes | CMS Bridge FAQ |
| Provider CTA facts (pricing, formulary) | Monthly | Official provider pages |
Last verified: . Next scheduled verification: May 12, 2026.
Frequently asked questions
Is there a CMS BALANCE Model participating plans list for Medicare Part D?
No. As of April 28, 2026, no actionable list exists because CMS paused the Medicare Part D component of the BALANCE Model on April 21, 2026 after the 80% projected enrollment threshold was not met. CMS instructed plan sponsors not to indicate BALANCE participation in HPMS or the Bid Pricing Tool for CY 2027. The Medicare GLP-1 Bridge — which doesn't require plan participation — is the access path for weight-loss GLP-1s through December 31, 2027.
Did CMS cancel the BALANCE Model entirely?
Not entirely. The Medicaid component of BALANCE is moving forward on schedule, with state applications open through July 31, 2026 and start dates between May 1, 2026 and January 1, 2027. The Medicare Part D component is delayed indefinitely for 2027, with CMS describing the pause as "pending further evaluation and data collection." Watch the CY2028 Advance Notice (typically released January or February 2027) for the next signal on Part D BALANCE.
Does my Part D plan have to opt in to the Medicare GLP-1 Bridge?
No. CMS administers the Bridge directly through a single central processor (Humana, working through the LI NET infrastructure), outside the regular Part D benefit and payment flow. Part D sponsors don't have to opt in for eligible beneficiaries to access Bridge-covered medications, and your individual plan has no role in approving or processing your Bridge prescription.
Is Humana the only plan that can use the Bridge?
No. Humana serves as the Bridge's central processor — an administrative role for all eligible beneficiaries, not just Humana plan members. You can use the Bridge regardless of which Part D plan you're enrolled in, as long as you're in an eligible plan type (PDP, MA-PD, SNP, EGWP, LI NET, or dual-eligible in one of these).
Which GLP-1 drugs are covered by the Medicare GLP-1 Bridge?
The Bridge covers all formulations of Wegovy® (injection and tablets), the Zepbound® KwikPen® formulation only, and all formulations of Foundayo® for eligible weight-management use. It does not cover Zepbound single-dose vials or pens, Ozempic, Mounjaro, Rybelsus, Saxenda, or any compounded GLP-1.
Are Ozempic and Mounjaro covered for weight loss under the Bridge?
No. Ozempic is FDA-approved for type 2 diabetes (and cardiovascular and chronic kidney disease risk reduction) and Mounjaro is FDA-approved for type 2 diabetes — neither is approved for weight loss, so neither is on the Bridge drug list. Both are coverable through your regular Part D plan when prescribed for their FDA-approved indications, subject to your plan's formulary and prior authorization rules.
Does the $50 Bridge copay count toward my Part D out-of-pocket cap?
No. Because the Bridge operates outside the regular Part D benefit structure, your $50 copay does not count toward your Part D True Out-of-Pocket cap (TrOOP), which is $2,100 in 2026 and $2,400 in 2027. Bridge spending also doesn't help you reach the catastrophic phase of your Part D benefit on your other medications.
Does Low-Income Subsidy (LIS) or Extra Help apply to the Bridge?
No. LIS and Extra Help cost-sharing reductions don't apply to Bridge claims, even if you have full LIS on your other Part D medications. Every eligible beneficiary pays the same $50 copay regardless of income, which is a known limitation that disproportionately affects the lowest-income Medicare enrollees.
Can I use a manufacturer savings card or coupon with the Bridge?
No. CMS has stated that coupons and discount programs cannot be applied to Bridge claims. Your $50 copay is the $50 copay.
Can a telehealth provider submit my Bridge prior authorization?
Yes, in principle. CMS doesn't require the prescribing provider to be enrolled in Medicare to write a prescription or submit a PA for Bridge drugs, though the provider can't be on the CMS Preclusion List. The PA must include the Bridge-required attestations. CMS will release detailed submission processes in spring 2026; your provider should be tracking that guidance.
What happens after December 31, 2027?
As of April 28, 2026, no successor program is confirmed. CMS could extend the Bridge again, relaunch BALANCE for plan year 2028 with revised terms, or build a different mechanism. The CY2028 Advance Notice (expected January or February 2027) is the next document to watch. We update this answer as guidance becomes available.
Should I switch Part D plans for 2027 to "join BALANCE"?
No. There is no BALANCE-participating Part D plan to switch into for 2027 because the Part D component is paused. Choose your 2027 Part D plan based on coverage of your other medications, network pharmacies, premiums, deductibles, and star ratings. The Bridge can cover your weight-loss GLP-1 access regardless of which eligible plan type you pick, provided you meet the BMI/diagnosis criteria.
What's the difference between BALANCE participating plans and the Medicare GLP-1 Bridge?
BALANCE was designed to integrate GLP-1 coverage into participating Part D plans' benefits with a broader drug list and Part D-integrated cost-sharing; that integration didn't launch in 2027. The Bridge is a temporary, CMS-administered demonstration that operates outside Part D, covers a narrower drug list (Wegovy, Zepbound KwikPen, Foundayo), charges a flat $50 copay, and runs through December 31, 2027. Right now the Bridge is the only active Medicare path for weight-loss GLP-1 coverage.
Your next step
If you're still here, you've now seen what nobody else is saying clearly: there is no BALANCE participating Part D plan list to shop for in 2027, you don't need one, and the Bridge can cover your weight-loss GLP-1 access at $50/month through December 31, 2027 if you qualify — regardless of which eligible Part D plan you're in. Pick the path that matches your situation:
If you're on Medicare and likely qualify for the Bridge
Start the conversation with your prescriber now so the prior authorization is ready when the Bridge opens July 1, 2026.
Read our full Medicare GLP-1 Bridge walkthrough →If you're on Medicaid
Check your state Medicaid agency's BALANCE application status and existing GLP-1 obesity coverage.
See our GLP-1 Medicaid coverage by state guide →If you're not on Medicare or Medicaid
Your path runs through commercial insurance, manufacturer self-pay programs, or telehealth platforms with insurance concierge support.
See current GLP-1 cash-pay pricing →If you're not sure where you fit
We built the matching quiz for exactly this moment.
Take the free 60-second matching quiz →Still not sure which GLP-1 program is right for you?
Take our free 60-second matching quiz. We ask about your insurance type, state, current medication, and goals — then route you to the exact path that fits. No email. No signup. Personalized recommendation in under a minute.
Whether that's the Bridge, your state Medicaid program, an FDA-approved self-pay option, or something else entirely.
Take the Free 60-Second Matching Quiz →Update log
- — Page published. Reflects CMS April 21, 2026 HPMS announcement (as reported by AHA News, Reuters, Avalere Health) pausing Part D BALANCE for CY 2027 and extending the Medicare GLP-1 Bridge through December 31, 2027. All current Bridge eligibility, drug coverage, cost, and PA workflow details verified against CMS source pages.
- Next scheduled verification: May 12, 2026. What we'll re-check: State Medicaid agreement executions; any new public insurer statements; CMS spring 2026 operational guidance on Bridge claims processing; any FDA actions affecting the Bridge drug list.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup