By The RX Index Research Team ·
CMS BALANCE Model GLP-1 Eligibility: Who Qualifies, What Costs $50, and What Just Changed
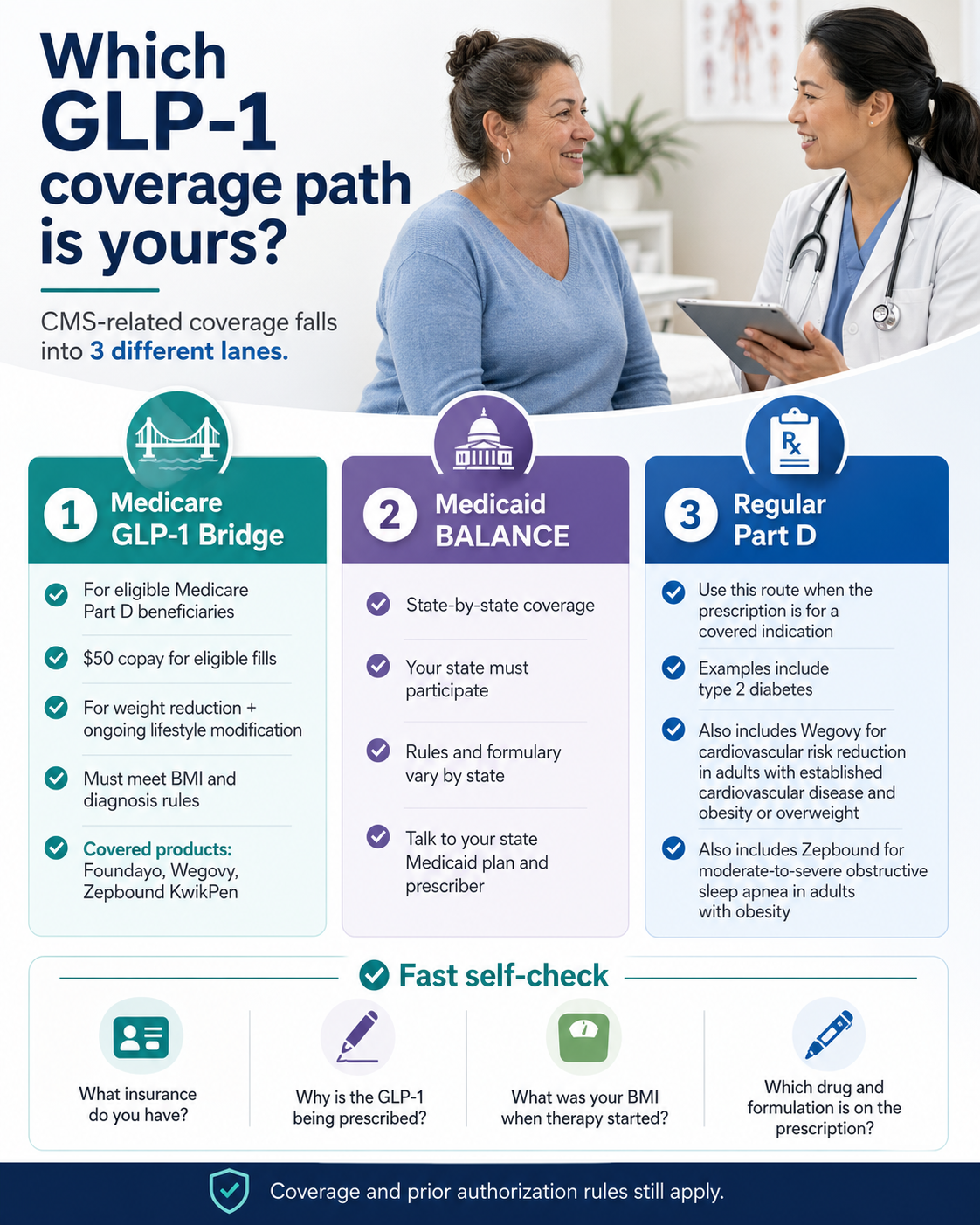
CMS BALANCE Model GLP-1 eligibility isn’t one rule. It’s three. If you’re on Medicare, the live path through 2027 is the GLP-1 Bridge — $50 a month for Wegovy, Zepbound KwikPen, or Foundayo if you meet the BMI and diagnosis criteria below. If you’re on Medicaid, coverage depends on whether your state opts in to BALANCE between May 2026 and January 2027. And if your GLP-1 is being prescribed for diabetes, cardiovascular risk, or sleep apnea, that may be a regular Part D route through your existing plan.
Quick path: find your lane
| Your situation | Likely lane | First step |
|---|---|---|
| On Medicare Part D, prescribed for weight loss, BMI ≥27 with the right diagnosis | Medicare GLP-1 Bridge ($50/mo) | Confirm tier below, then doctor visit |
| On Medicaid in a participating state | Medicaid BALANCE | Check state status below |
| Prescribed for diabetes / cardiovascular risk / sleep apnea | Regular Part D / standard plan PA | Use your plan’s standard prior authorization |
| Don’t qualify or don’t use government insurance | FDA-approved cash-pay | See “If you don’t qualify” section |
| Not sure | Take the 60-second quiz | Personalized routing |
No signup. No provider pitch. We'll tell you whether your next step is Bridge, Medicaid, regular Part D, or another route.
Tap the infographic to take the 60-second matching quiz →
What we actually verified before publishing
Every fact checked against primary sources within the past 7 days.
| Claim | Verified value | Source | Last checked |
|---|---|---|---|
| Bridge dates | July 1, 2026 – December 31, 2027 (extended April 21, 2026) | CMS Medicare GLP-1 Bridge FAQ | Apr 27, 2026 |
| Medicare BALANCE 2027 launch | Delayed; CMS evaluating | CMS HPMS memo, April 21, 2026; AHA News, April 22, 2026 | Apr 27, 2026 |
| Medicaid BALANCE window | States can opt in May 1, 2026 – January 1, 2027; applications open through July 31, 2026 | CMS BALANCE page; AHA News | Apr 27, 2026 |
| Bridge BMI/diagnosis tiers | 3 routes: ≥35, ≥30 + condition, ≥27 + condition | CMS Bridge FAQ | Apr 27, 2026 |
| Bridge drug list | Foundayo (all forms), Wegovy injection/tablets, Zepbound KwikPen only | CMS Bridge FAQ, April 6, 2026 update | Apr 27, 2026 |
| Bridge cost | $50 patient copay; manufacturers provide drugs at $245 net price/month | CMS Bridge FAQ | Apr 27, 2026 |
| Pharmacy reimbursement | Wholesale acquisition cost less the $50 copay, plus dispensing fee and applicable sales tax | CMS Bridge FAQ | Apr 27, 2026 |
| LIS doesn't apply to Bridge copay | Confirmed | CMS Bridge FAQ | Apr 27, 2026 |
| Coupons can't be applied to Bridge claims | Confirmed | CMS Bridge FAQ | Apr 27, 2026 |
| $50 doesn't count toward TrOOP | Confirmed | CMS Bridge FAQ; KFF | Apr 27, 2026 |
| Bridge BIN/PCN | 028918 / MEDDGLP1BR | CMS Bridge FAQ | Apr 27, 2026 |
| Central processor | Humana (current LI NET administrator) | CMS Bridge FAQ | Apr 27, 2026 |
| Pre-BALANCE Medicaid GLP-1 weight-loss coverage | 13 states as of January 2026 | KFF Medicaid GLP-1 brief, January 2026 | Apr 27, 2026 |
| FDA Wegovy CV indication | Approved to reduce risk of major adverse cardiovascular events in adults with established CVD and obesity/overweight | FDA press release | Apr 27, 2026 |
| FDA Zepbound OSA indication | Approved for moderate-to-severe obstructive sleep apnea in adults with obesity | FDA press release | Apr 27, 2026 |
| FDA Foundayo (orforglipron) approval | Approved April 1, 2026 for chronic weight management with diet and physical activity | FDA Novel Drug Approvals 2026 | Apr 27, 2026 |
Pre-BALANCE Medicaid GLP-1 obesity coverage reflects KFF data as of January 2026. BALANCE state participation is listed as “Not publicly posted” until CMS or the state publishes a participation notice.
What “CMS BALANCE Model GLP-1 eligibility” actually means in 2026
CMS BALANCE Model GLP-1 eligibility describes who can get GLP-1 medication coverage through one of three CMS-related paths in 2026 and 2027: the Medicare GLP-1 Bridge demonstration (Part D beneficiaries, $50 copay), Medicaid BALANCE coverage (depends on state opt-in), or regular Medicare Part D coverage when the medication is prescribed for an already-coverable indication. Eligibility is not one rule — it’s a decision tree.
Here’s the part most headlines skipped: BALANCE is the umbrella, not the program you’ll actually use this year.
The BALANCE Model
The BALANCE Model itself ("Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth") is a five-year voluntary CMS initiative announced December 23, 2025 to run through December 31, 2031. It's the negotiation framework that brings manufacturers, state Medicaid agencies, and (originally) Medicare Part D plans to CMS-set pricing and coverage terms for select GLP-1 medications when used for weight management. It also pairs medication access with manufacturer-funded lifestyle support programs.
The Medicare GLP-1 Bridge
The Medicare GLP-1 Bridge is a separate short-term demonstration that runs underneath BALANCE — different legal authority (Section 402 vs. Section 1115A), different administration (CMS central processor vs. state Medicaid programs and Part D plans), and different cost mechanics. The Bridge is what's actually delivering the $50 copay to Medicare beneficiaries between July 1, 2026 and December 31, 2027. Manufacturers participating in the Bridge provide eligible drugs at a $245 net price per monthly supply.
Medicaid BALANCE
Medicaid BALANCE is the state-by-state track. State Medicaid agencies can apply through July 31, 2026 and start participation anywhere from May 1, 2026 through January 1, 2027. Whether your state participates determines whether you have access at all. Note: the publicly verified $245/month Bridge net price applies to the Medicare Bridge specifically; Medicaid BALANCE pricing is negotiated state-by-state.
Regular Part D
Regular Part D still exists. If your prescriber writes for a GLP-1 because of type 2 diabetes, cardiovascular risk reduction in adults with established CVD and obesity/overweight (Wegovy injection), or moderate-to-severe obstructive sleep apnea in adults with obesity (Zepbound), that may be a regular Part D route — subject to your plan's formulary and prior authorization rules. CMS has been explicit that Bridge claims are separate from claims covered under the basic Part D benefit.
What changed on April 21, 2026 — the news every other ranking page is missing
April 21, 2026 CMS announcement
On April 21, 2026, CMS announced via HPMS memo that the Medicare Part D portion of the BALANCE Model will not launch in 2027 as originally planned. The Medicare GLP-1 Bridge — originally scheduled to end December 31, 2026 — has been extended through December 31, 2027 to fill the gap. The Medicaid portion of BALANCE is still moving forward on the original schedule.
Old timeline vs. current timeline
| Element | Original plan | Current (post-April 21) |
|---|---|---|
| Medicare GLP-1 Bridge | July 1 – December 31, 2026 (6 months) | July 1, 2026 – December 31, 2027 (18 months) |
| Medicare Part D BALANCE launch | January 1, 2027 | Delayed; no confirmed relaunch date |
| Medicaid BALANCE | States join May 2026 – January 2027 | Unchanged |
| BALANCE Model end | December 31, 2031 | December 31, 2031 |
Why the Part D portion was paused
CMS required at least 80% of Part D beneficiaries to be enrolled in plans that opted in to BALANCE for the model to launch in Medicare for 2027. The Part D plan application deadline was April 20, 2026. CMS announced the delay one day after the deadline closed and said it would extend the Bridge while it evaluates additional data.
Per Avalere Health’s analysis, plans faced two practical problems: they had to price competitive 2027 bids without any prior claims data for GLP-1s used for weight loss in Medicare (because Medicare has never covered these drugs for weight loss before), and they faced adverse-selection risk from beneficiaries likely to switch plans for GLP-1 access.
If you’re on Medicare
- •The $50/month Bridge is now an 18-month program. Your access window runs July 1, 2026 through December 31, 2027.
- •You don't need to switch Part D plans for 2027 to keep Bridge access.
- •Long-term Medicare coverage is uncertain. CMS didn't announce a relaunch date. Watch fall 2027 open enrollment.
If you’re on Medicaid
- •Nothing changed in the Medicaid track.
- •State Medicaid agencies still have until July 31, 2026 to apply.
- •Start dates run between May 1, 2026 and January 1, 2027.
- •The Medicaid track of BALANCE is the active story right now.
The 60-second quiz accounts for your plan type, state, BMI, and timeline.
Do you qualify for the Medicare GLP-1 Bridge? Five checks, not three
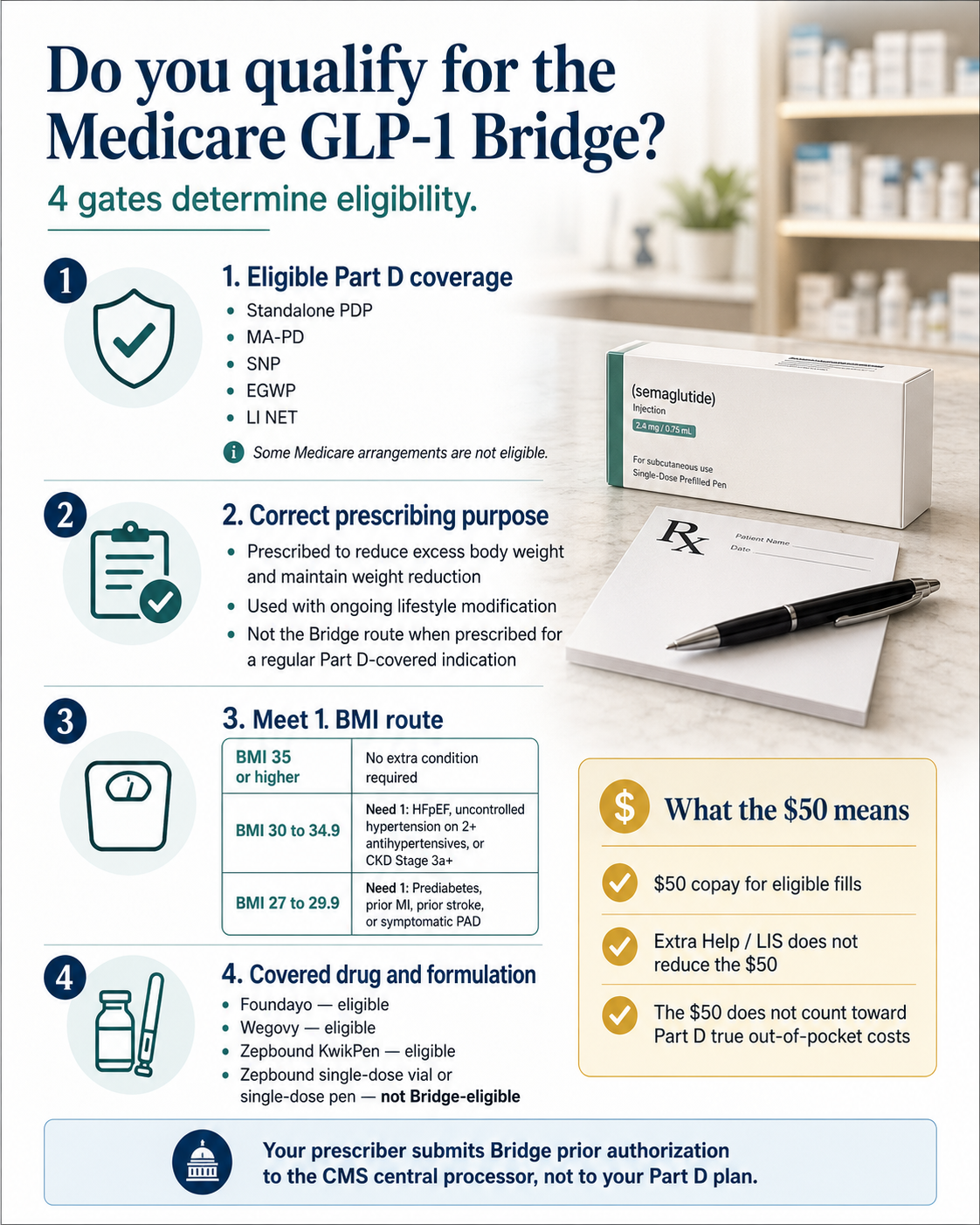
To qualify for the Medicare GLP-1 Bridge, five things have to line up: you’re 18 or older, enrolled in an eligible Part D plan type, the medication is prescribed for weight reduction with ongoing lifestyle modification, you meet one of three BMI/diagnosis routes, and the specific drug formulation is on the Bridge’s covered list. Miss any of the five and the prior authorization gets denied — even if the others are perfect.
Most pages stop at BMI. We’re laying out all five checks because the most common denials we expect to see have nothing to do with BMI.
Tap the infographic to find your Bridge tier →
Age 18 or older
CMS includes adult age (18+) in the clinical criteria. The Bridge is not available to pediatric beneficiaries.
Eligible Part D coverage
Eligible plan types ✓
- ✓Standalone Prescription Drug Plan (PDP)
- ✓Medicare Advantage with drug coverage (MA-PD) — HMO, HMOPOS, Local PPO, Regional PPO
- ✓Special Needs Plan (SNP)
- ✓Employer/union Group Waiver Plan (EGWP)
- ✓Limited Income Newly Eligible Transition (LI NET)
- ✓Dual-eligible (Medicare + Medicaid) enrolled in one of the above
Not eligible ✗
- ✗Private Fee-for-Service (PFFS) without a separate PDP
- ✗Section 1876 cost contract plans
- ✗Section 1833 health care prepayment plans
- ✗PACE organizations
- ✗Fallback plans
- ✗Religious fraternal benefit plans
Not sure which type you have? Check your Medicare Summary Notice, your Part D plan card, or call 1-800-MEDICARE.
Correct prescribing purpose
CMS is precise. The medication must be prescribed “to reduce excess body weight and maintain weight reduction in combination with current and ongoing lifestyle modification including structured nutrition and physical activity consistent with the applicable FDA approved label.”
Important: If your doctor is prescribing Wegovy because you have established cardiovascular disease and obesity, that’s a different (already-coverable) Part D path — not the Bridge. The drug has to be for weight reduction and maintenance, and your prescriber has to attest you’re combining it with lifestyle modification.
One of three BMI/diagnosis routes
Three routes. You only need to meet one.
| Route | BMI at therapy initiation | Extra condition? | Qualifying conditions |
|---|---|---|---|
| Route 1 | ≥35 | No | None — BMI alone qualifies |
| Route 2 | ≥30 (below 35) | Yes — one of three | HFpEF · Uncontrolled hypertension on 2+ meds (SBP >140 or DBP >90) · CKD Stage 3a+ |
| Route 3 | ≥27 (below 30) | Yes — one of four | Prediabetes (per ADA guidelines) · Prior MI · Prior stroke · Symptomatic peripheral artery disease |
Details competitors compress or get wrong:
“Uncontrolled hypertension” has a specific definition. It’s systolic above 140 mmHg or diastolic above 90 mmHg while on two or more antihypertensive medications. Well-controlled hypertension does not qualify under Route 2.
Route 2 requires HFpEF specifically — heart failure with preserved ejection fraction. HFrEF is not on the Bridge list at writing.
Symptomatic PAD, not asymptomatic. Documented intermittent claudication, rest pain, or critical limb ischemia.
Eligible drug and formulation
Bridge-eligible products as of April 6, 2026 update:
- ✓Foundayo (orforglipron) — all formulations
- ✓Wegovy (semaglutide) — injection and tablets
- ✓Zepbound (tirzepatide) — KwikPen ONLY — not single-dose vial, not single-dose pen
- ✗Zepbound single-dose vial / single-dose pen — NOT Bridge-eligible
We'll match your BMI, diagnoses, plan type, and current medications to the right route — and tell you what your prescriber needs to document.
Does BMI 30 alone qualify for the $50 Medicare GLP-1 Bridge?
No.
A BMI of 30 alone is not enough to qualify for the Medicare GLP-1 Bridge. BMI ≥30 only qualifies if you also have heart failure with preserved ejection fraction, uncontrolled hypertension despite two antihypertensive medications, or chronic kidney disease at Stage 3a or above. The only BMI-only route is BMI ≥35.
This is the single most common question we see in public Medicare and weight-loss forums.
| Your situation | Bridge-eligible? |
|---|---|
| BMI ≥35 | ✅ Yes (Route 1) |
| BMI 30–34.9 only | ❌ No |
| BMI 30–34.9 + HFpEF | ✅ Yes (Route 2) |
| BMI 30–34.9 + uncontrolled hypertension on 2+ meds | ✅ Yes (Route 2) |
| BMI 30–34.9 + CKD Stage 3a+ | ✅ Yes (Route 2) |
| BMI 27–29.9 + prediabetes | ✅ Yes (Route 3) |
| BMI 27–29.9 + prior MI / stroke / symptomatic PAD | ✅ Yes (Route 3) |
| BMI <27 | ❌ No |
If you fall into the “no” rows, skip to the “If you don’t qualify” section — we route you to the next-best option.
What if my BMI is lower now because the medication worked?
CMS uses the BMI you had at the time you initiated GLP-1 therapy — not your current BMI. The criteria are designed so successful weight loss doesn’t disqualify you mid-treatment.
CMS’s own Bridge FAQ described this scenario: a beneficiary who initiated GLP-1 therapy in September 2024 with a BMI of 37, and at the time of a July 2026 PA request had a BMI of 34. CMS says the prescribing provider should attest the beneficiary met the BMI ≥35 criterion at the time therapy was initiated.
| Evidence type | Where to get it | Why it helps |
|---|---|---|
| Starting weight | Medical visit before/at initiation | Establishes BMI at the qualifying moment |
| Documented height | Your medical chart | Required to calculate BMI |
| Date of initiation | Pharmacy fill history; clinic note | Anchors the timeline |
| Initiation visit note | Original prescriber's records | Direct attestation source |
| First pharmacy fill | Your pharmacy can print in 2 minutes | Independent confirmation |
Prescriber wording that helps the PA:
“Patient met BMI criterion at initiation of GLP-1 therapy on [date], with documented BMI of [value].”
Which GLP-1 medications are included in CMS BALANCE and the Medicare Bridge?
The Medicare GLP-1 Bridge covers Foundayo, Wegovy (injection and tablets), and Zepbound KwikPen for weight management. The broader BALANCE Model drug list is wider — it includes Mounjaro, Ozempic, and Rybelsus too — but those go through state Medicaid coverage rules under BALANCE-Medicaid, not through the Bridge.
Medicare GLP-1 Bridge — drugs you can get for $50/month
| Drug | Active ingredient | Form | Bridge-covered? | Formulation trap |
|---|---|---|---|---|
| Foundayo | Orforglipron | All formulations | ✅ Yes | None — all forms eligible |
| Wegovy | Semaglutide | Injection (all doses) | ✅ Yes | None |
| Wegovy | Semaglutide | Oral tablet | ✅ Yes | None |
| Zepbound | Tirzepatide | KwikPen only | ✅ Yes (KwikPen) | Only KwikPen — not vial, not single-dose pen |
| Zepbound | Tirzepatide | Single-dose vial | ❌ Not on Bridge | Confirm formulation on the script |
| Zepbound | Tirzepatide | Single-dose pen | ❌ Not on Bridge | Confirm formulation on the script |
| Ozempic | Semaglutide | Any form | ❌ Not for weight loss | Regular Part D path for diabetes |
| Mounjaro | Tirzepatide | Any form | ❌ Not for weight loss | Regular Part D path for diabetes |
| Rybelsus | Semaglutide | Tablet | ❌ Not for weight loss | Regular Part D path for diabetes |
| Saxenda | Liraglutide | Injection | ❌ Not on Bridge list | — |
| Compounded semaglutide / tirzepatide | n/a | Any | ❌ Not FDA-approved | Not on CMS Bridge or BALANCE drug lists |
The Ozempic question (we keep getting this one)
“Ozempic and Wegovy contain the same active ingredient — can I get Ozempic through the Bridge for weight loss?” No. Ozempic is FDA-approved for type 2 diabetes; Wegovy is FDA-approved for chronic weight management. Despite sharing semaglutide as the active ingredient, they’re separate FDA-approved products. The Bridge covers FDA-approved products for the use they’re approved for. Ozempic for weight loss isn’t a Bridge path.
If you have type 2 diabetes, Ozempic may be coverable through your regular Part D plan for the diabetes indication — but that’s a regular Part D claim, not a Bridge claim.
Compounded GLP-1s
What does the $50 Medicare GLP-1 price actually cover?
The $50 is your monthly copay under the Medicare GLP-1 Bridge for an eligible fill — not a universal GLP-1 price. Manufacturers provide eligible drugs at a $245 net price per monthly supply. Pharmacies are reimbursed by the central processor at no less than the wholesale acquisition cost minus the $50 copay, plus a dispensing fee and applicable sales tax. The Bridge operates outside the Part D benefit, which has four practical consequences most articles skip.
How the money flows
| Step | Mechanic |
|---|---|
| You pay at the pharmacy counter | $50 |
| Pharmacy submits the claim | Through the Bridge BIN/PCN (028918 / MEDDGLP1BR) to the central processor |
| Pharmacy gets reimbursed | Wholesale acquisition cost (WAC) of the drug, less the $50 copay, plus a dispensing fee, plus sales tax where applicable |
| Manufacturer net price | $245 per monthly supply for participating manufacturers |
| Coupons / discount programs | Cannot be applied to Bridge claims |
| LIS / Extra Help | Does not reduce the $50 copay |
| TrOOP (Part D OOP cap) | $50 does not count toward TrOOP |
Four consequences most articles skip
1. The $50 doesn't count toward your Part D out-of-pocket cap.
Because the Bridge sits outside the standard Part D benefit, your $50 monthly Bridge copay does not contribute to your true out-of-pocket cost (TrOOP) total. If you're a high-spend Part D beneficiary who would otherwise hit the OOP cap on other medications, your Bridge spending doesn't help you get there.
2. Extra Help / LIS doesn't lower the $50.
The Low-Income Subsidy program (Extra Help) reduces or eliminates Part D cost-sharing for qualifying low-income beneficiaries. Under the Bridge, LIS cost-sharing subsidies do not apply. Per CMS, the Bridge copay is $50, period — even if you would otherwise pay $0 to $4 under LIS for a regular Part D drug. KFF flagged this as a real problem for low- and modest-income beneficiaries.
3. Coupons and discount programs can't be used.
CMS prohibits coupons and discount programs on Medicare GLP-1 Bridge claims. You can't stack a manufacturer copay card on top of the $50.
4. You pay $50 every month.
No introductory price, no annual prepay savings, no graduated cost as you titrate up. It's $50 a month for as long as you remain eligible and the Bridge program is operating, through December 31, 2027.
The honest tradeoff: this is narrower than the headlines suggest
The Bridge is real. It works. It’s a meaningful change for the beneficiaries who qualify. But it is narrower than the headlines suggest: only specific drugs, only specific formulations, only specific BMI/diagnosis combinations, only specific Part D plan types, only between July 1, 2026 and December 31, 2027, only with a $50 copay that doesn’t behave like a regular Part D cost-share. If you read this and conclude the Bridge isn’t your path, that’s a useful answer — and we’ll show you the next-best route below.
How does your doctor submit the Medicare GLP-1 Bridge prior authorization?
For Bridge-covered weight-management prescriptions, the prescriber submits the prior authorization to CMS’s central processor — Humana, the current administrator of the LI NET program — not to your Part D plan. Sending the PA to your Part D plan is one of the most common — and most preventable — denial reasons we expect to see when the program launches July 1, 2026.
The prescriber workflow, step by step
- 1
Confirm your Part D plan type is eligible. (Check 2 above.)
- 2
Confirm the drug and formulation are on the Bridge list. (Foundayo, Wegovy injection/tablets, Zepbound KwikPen only.)
- 3
Confirm your BMI/diagnosis route at therapy initiation. (If you're a continuing patient, this is your BMI when you started, not your current BMI.)
- 4
Confirm the prescription is for weight reduction with ongoing lifestyle modification. (Check 3.)
- 5
Submit the PA to the CMS central processor (Humana) — not your Part D plan, not your plan's PBM, not the pharmacy.
- 6
Pharmacy submits the claim using the Bridge-specific BIN/PCN: 028918 / MEDDGLP1BR.
- 7
You pay $50 at the counter on approved fills.
Bridge-specific BIN/PCN — print and keep with your Medicare card
BIN
028918
PCN
MEDDGLP1BR
Central processor
Humana (LI NET administrator)
Paper claims
Not accepted
Telehealth note
CMS has indicated that a provider does not need to be enrolled in Medicare to prescribe under the Bridge or to submit a PA, but they cannot be on the CMS Preclusion List. If you’re using a telehealth path, ask the platform directly whether their prescribers can submit Bridge PAs starting July 1, 2026.
Doctor-script line you can read aloud
“This is a Medicare GLP-1 Bridge prior authorization for a weight-management prescription. Per CMS, Bridge PAs go to the central processor — Humana — not to my Part D plan. Pharmacy claims use BIN 028918 and PCN MEDDGLP1BR. Can we confirm we’re submitting through the Bridge route?”
Includes the route checklist, documentation list, and pharmacy BIN/PCN note. Personalized to your tier.
How does Medicaid BALANCE Model GLP-1 eligibility work?
Medicaid BALANCE is voluntary and state-by-state. State Medicaid agencies can apply through July 31, 2026 and choose participation start dates between May 1, 2026 and January 1, 2027. Whether you have access depends entirely on whether your state opts in and what eligibility/PA criteria your state Medicaid program adopts. Medicaid BALANCE is not one national rule.
Two important baseline facts
First: Medicaid coverage of GLP-1s for non-weight-loss indications (like type 2 diabetes) is already required in state Medicaid programs. That’s not new. BALANCE doesn’t change that.
Second: Medicaid coverage of GLP-1s for obesity / weight loss specifically is optional for states. As of January 2026, 13 state Medicaid programs covered GLP-1s for obesity treatment under fee-for-service per KFF. BALANCE is the first national framework that makes broader Medicaid weight-loss coverage financially feasible for more states.
Documented Medicaid changes (2025–2026)
| State | What changed | When | Source |
|---|---|---|---|
| California (Medi-Cal) | Eliminated GLP-1 weight-loss coverage for adults 21+ | Effective Jan 1, 2026 | Medi-Cal Rx Contract Drugs List; KFF |
| New Hampshire | Eliminated Medicaid GLP-1 weight-loss coverage | 2025–2026 | KFF January 2026 |
| Pennsylvania | Eliminated Medicaid GLP-1 weight-loss coverage | 2025–2026 | KFF January 2026 |
| South Carolina | Eliminated Medicaid GLP-1 weight-loss coverage | 2025–2026 | KFF January 2026 |
| Michigan | Restricted Medicaid GLP-1 weight-loss coverage | 2026 | KFF January 2026 |
| North Carolina | Eliminated Oct 2025; reinstated Dec 2025 | Late 2025 | KFF January 2026 |
State-by-state Medicaid status tracker
Last verified: Updated as CMS and state Medicaid agencies post BALANCE participation notices. We don’t list a state as “enrolled” without a public posted notice or state Medicaid bulletin.
| State | Pre-BALANCE GLP-1 weight-loss Medicaid coverage | BALANCE intent | Start | Source |
|---|---|---|---|---|
| Alabama | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Alaska | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Arizona | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Arkansas | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| California (Medi-Cal) | Eliminated for adults 21+ as of Jan 1, 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | Medi-Cal Rx; KFF |
| Colorado | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Connecticut | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Delaware | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| DC | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Florida | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Georgia | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Hawaii | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Idaho | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Illinois | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Indiana | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Iowa | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Kansas | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Kentucky | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Louisiana | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Maine | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Maryland | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Massachusetts | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Michigan | Covered under FFS as of January 2026 (verify current PDL for any restrictions) | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Minnesota | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Mississippi | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Missouri | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Montana | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Nebraska | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Nevada | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| New Hampshire | Eliminated in 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| New Jersey | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| New Mexico | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| New York | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| North Carolina | Covered under FFS as of January 2026 (eliminated Oct 2025; reinstated Dec 2025) | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| North Dakota | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026. Note: state insurance mandate (Jan 2025) is separate from Medicaid FFS; verify ND Medicaid PDL. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Ohio | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Oklahoma | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Oregon | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Pennsylvania | Eliminated in 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Rhode Island | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| South Carolina | Eliminated in 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| South Dakota | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Tennessee | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Texas | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Utah | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Vermont | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Virginia | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Washington | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| West Virginia | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Wisconsin | Covered under FFS as of January 2026 | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
| Wyoming | Not listed by KFF among 13 state Medicaid FFS programs covering GLP-1s for obesity as of January 2026; verify current state/MCO formulary. | Not publicly posted as of June 26, 2026. | No public BALANCE start date posted. | KFF Jan 2026 |
Why we’re conservative
We’d rather show an honestly incomplete tracker than confidently list a state wrong. We refresh this table monthly against the current KFF Medicaid GLP-1 brief and direct state Medicaid pharmacy bulletins. If your state’s BALANCE status is not yet posted and you have a local source, email us and we’ll add it with citation.
What to do as a Medicaid beneficiary right now
- 1.
Check the documented changes table above. If your state is listed as eliminating, restricting, or reinstating coverage, that's a meaningful change to the baseline.
- 2.
Call your state Medicaid member services. Ask whether your state has applied for BALANCE participation, when coverage starts, and whether the drug your prescriber recommends will be on the state's BALANCE-Medicaid formulary.
- 3.
Save your state Medicaid pharmacy benefit page. Bookmark the formulary and the prior authorization criteria. Re-check monthly between now and January 2027.
- 4.
Talk to your prescriber. Bring your state's current PA criteria for GLP-1s. The criteria your state applies to BALANCE-Medicaid may differ from the Bridge criteria.
If your state's BALANCE status is not yet publicly posted, the quiz routes you to the fastest confirmed-available path while we monitor for updates.
When should you use regular Part D instead of the Bridge?
Use regular Part D when your GLP-1 is prescribed for an indication that may already be coverable under your plan’s basic Part D benefit — type 2 diabetes, cardiovascular risk reduction in adults with established CVD and obesity/overweight (Wegovy injection), or moderate-to-severe obstructive sleep apnea in adults with obesity (Zepbound). CMS specifically directs that those claims should NOT go through the Bridge.
Diagnosis-to-path table
| Why the GLP-1 is prescribed | Likely path | PA destination |
|---|---|---|
| Weight reduction and maintenance only | Medicare GLP-1 Bridge (if you meet criteria) | CMS central processor (Humana) |
| Type 2 diabetes | Regular Part D / Medicaid covered indication (subject to plan formulary) | Part D plan / PBM |
| Wegovy for cardiovascular risk reduction in adults with established CVD and obesity/overweight | Regular Part D (FDA-approved indication; subject to plan formulary) | Part D plan / PBM |
| Zepbound for moderate-to-severe obstructive sleep apnea in adults with obesity | Regular Part D (FDA-approved indication; subject to plan formulary) | Part D plan / PBM |
| Medicaid weight-loss coverage where state opts in | Medicaid BALANCE / state Medicaid program | State Medicaid PA |
| Cash-pay outside government insurance | FDA-approved cash-pay or telehealth path | Telehealth platform / manufacturer direct |
What could stop you from getting approved even if you seem to qualify?
The seven most preventable Medicare GLP-1 Bridge denial reasons are: wrong plan type, wrong drug formulation (especially Zepbound vial/pen vs. KwikPen), missing BMI-at-initiation documentation, sending the PA to the wrong place, prescribing for an indication that’s actually regular Part D, low-income beneficiaries assuming Extra Help applies, and Medicaid beneficiaries assuming their state opted in. Each is fixable before the prescription is even written.
| Blocker | Why it matters | How to reduce risk |
|---|---|---|
| Wrong plan type | Not all Medicare arrangements are Bridge-eligible | Confirm PDP, MA-PD, SNP, EGWP, or LI NET status |
| Wrong drug formulation | Zepbound KwikPen yes, Zepbound vial/pen no | Confirm the formulation/NDC on the prescription before submission |
| BMI documented at the wrong time | CMS uses BMI at therapy initiation | Bring historical weight/BMI proof; have the prescriber attest to initiation BMI |
| PA sent to your Part D plan | Bridge PA goes to the central processor (Humana) | Use the doctor-script line; have the pharmacy use BIN 028918 / PCN MEDDGLP1BR |
| Prescribing indication that's already regular Part D | OSA / CV risk / diabetes are not Bridge claims | Route based on diagnosis, not just drug name |
| Assuming Extra Help / LIS reduces the $50 | LIS does not apply to the Bridge copay | Budget for the full $50/month |
| Assuming your state Medicaid opted into BALANCE | Medicaid BALANCE is voluntary and state-by-state | Verify against the tracker above and your state's pharmacy bulletin |
On appeals
If a prior authorization gets denied, it’s not necessarily over. The Bridge does not impact your existing Part D appeal rights. Talk to your prescriber’s office and your state’s State Health Insurance Assistance Program (SHIP) — Medicare counseling is free, local, unbiased, and often the fastest way to get an appeal pointed in the right direction (find yours at shiphelp.org).
One important nuance: if you don’t meet a fixed Bridge eligibility criterion (e.g., BMI ≥27 with no qualifying condition), an appeal won’t change that — Bridge criteria are set by CMS, not by your plan. Appeals are the right tool for regular Part D plan utilization-management issues.
What if you don’t qualify for CMS BALANCE or the Medicare GLP-1 Bridge?
Not qualifying for the Bridge or BALANCE-Medicaid doesn’t mean there’s no path. The four next-best routes, in order: regular Part D coverage if your prescription matches an FDA-approved non-weight-loss indication; free local Medicare counseling through SHIP if you’re navigating denials; manufacturer direct programs (which often exclude government-program beneficiaries); or an FDA-approved telehealth provider with insurance support.
If you have type 2 diabetes, established cardiovascular disease with obesity or overweight, or moderate-to-severe obstructive sleep apnea with obesity, traditional Part D coverage already exists for the FDA-approved indication, subject to your plan formulary and PA. Talk to your prescriber about whether your situation matches.
If you’ve been denied or you’re not sure which path applies, SHIP — your State Health Insurance Assistance Program — provides free, local, unbiased Medicare counseling. They can help with appeals, plan comparison, and program eligibility questions you’d otherwise pay a broker for. Find your state’s SHIP at shiphelp.org.
| Program | What to check | Where to verify |
|---|---|---|
| NovoCare (Wegovy) | Pricing varies by form and dose; some doses include time-limited intro offers | novocare.com/patient/medicines/wegovy.html |
| LillyDirect (Zepbound) | Pricing varies by KwikPen dose; lower-dose offers may differ from regular pricing | lilly.com/products/zepbound (LillyDirect) |
| TrumpRx | Pricing on FDA-approved GLP-1s varies | TrumpRx site |
⚠️ Before choosing a provider, two things to know:
Clinician review is required. FDA-approved GLP-1 medications carry product-specific warnings including thyroid C-cell tumor and MEN2 risk language — discuss medical suitability with your prescriber.
Per Ro’s policy, Ro cannot coordinate GLP-1 coverage with government insurance plans. Medicare, Medicare Supplement, and TRICARE members may join Ro Body and pay out-of-pocket cash-pay rates; Medicaid and other government-funded plan members cannot join Ro Body.
Ro Body
Ro carries Zepbound (tirzepatide), Foundayo (orforglipron), Wegovy pill, Wegovy pen, and Ozempic among its FDA-approved cash-pay options, and includes an insurance concierge that handles prior authorization paperwork plus a free GLP-1 Insurance Coverage Checker.
Pricing: get started for $39, then as low as $74/month with annual plan paid upfront. Ro Body membership does not include the cost of medication — medication is charged separately.
Verify current Ro pricing and formulary on ro.co before relying.
See current Ro pricing and run the free Insurance Coverage Checker → (sponsored affiliate link, opens in a new tab)Use this only if you are not pursuing Medicare or Medicaid coverage. Membership is separate from medication cost. Government-plan limitations apply.
Sesame Care
Sesame carries the broadest branded formulary in the FDA-approved telehealth space — Wegovy, Zepbound, Ozempic, Mounjaro, Foundayo, and Saxenda — and offers Costco-member pricing on Wegovy and Ozempic. Strongest if you want maximum provider choice or branded comparison-shopping.
Compare FDA-approved branded options on Sesame Care → (sponsored affiliate link, opens in a new tab)Best if you want broader branded choice (Wegovy, Zepbound, Ozempic, Mounjaro, Foundayo, Saxenda).
What documents should you bring to your doctor?
Bring proof for the exact route you’re trying to use: plan type, drug/formulation, BMI at therapy initiation, qualifying diagnosis documentation, and prior fill history if you’re already on a GLP-1. A prepared patient gets a cleaner prior authorization, a faster decision, and far fewer back-and-forth requests for additional records.
Universal documentation (everyone)
- •Medicare or Medicaid ID card
- •Part D plan card (Medicare beneficiaries) or state Medicaid card (Medicaid)
- •Current weight and height
- •Current medication list
- •Willingness to commit to ongoing lifestyle modification — your prescriber attests to this on the PA
If you’re using Route 1 (BMI ≥35)
- •BMI documentation at therapy initiation (if continuing patient) or current BMI documented in clinic (if starting fresh)
If you’re using Route 2 (BMI ≥30 + condition)
- •BMI documentation
- •For HFpEF: cardiology records, echocardiogram with preserved ejection fraction
- •For uncontrolled hypertension on 2+ meds: 6+ months of BP readings; current antihypertensive regimen showing 2+ medications
- •For CKD Stage 3a+: recent eGFR / creatinine results
If you’re using Route 3 (BMI ≥27 + condition)
- •BMI documentation
- •For prediabetes: A1C 5.7–6.4% or fasting glucose 100–125 mg/dL or 2-hour OGTT 140–199 mg/dL (per ADA guidelines)
- •For prior MI: cardiology records, hospital discharge summary
- •For prior stroke: neurology records, hospital discharge summary
- •For symptomatic PAD: vascular records, ABI testing, documented symptoms
If you’re using Continuing GLP-1 patient
- •Date of GLP-1 therapy initiation
- •Starting weight (or BMI calculation) at initiation
- •Pharmacy fill history (your pharmacy can print this in 2 minutes)
- •Initiation visit clinic note from your original prescriber
If you’re using Medicaid BALANCE
- •Your state Medicaid pharmacy benefit page
- •Your state's current PA criteria for GLP-1 weight-loss prescriptions (if available)
A question to ask out loud at the visit
“Will this prior authorization be submitted to the CMS central processor (Humana) for the Medicare GLP-1 Bridge, to my Part D plan, or to state Medicaid? Which route fits my situation?”
If your prescriber’s office gives the right answer, you’re set. If they hesitate, you’ve spotted a process problem before it becomes a denial.
Common myths — what the headlines got wrong
Six of the most widely circulated claims about the BALANCE Model and the Medicare GLP-1 Bridge are wrong or oversimplified.
Myth 1 — “Medicare now covers GLP-1s for weight loss starting January 2027.”
Reality: Per the April 21, 2026 CMS memo, the Medicare Part D portion of BALANCE is delayed for 2027. Medicare beneficiaries will have access via the Bridge — extended through December 31, 2027 — but the long-term Part D BALANCE rollout has no confirmed launch date.
Myth 2 — “BALANCE and the GLP-1 Bridge are the same program.”
Reality: Different programs, different legal authority (Section 1115A vs. Section 402), different administrators, different timelines, different drug lists. The Bridge is a temporary direct-to-beneficiary mechanism. BALANCE is a five-year voluntary model running through December 2031.
Myth 3 — “If your BMI drops below 35 during treatment, you lose coverage.”
Reality: CMS uses the BMI at the time you initiated GLP-1 therapy, not your current BMI. Successful weight loss does not disqualify continuing patients.
Myth 4 — “All Part D plans automatically participate in BALANCE.”
Reality: Participation is voluntary — and as of April 21, 2026, Part D BALANCE is delayed entirely for 2027. The Bridge runs through CMS’s central processor regardless of which Part D plan you have.
Myth 5 — “The $50 Bridge copay counts toward my Part D out-of-pocket cap.”
Reality: It does not. The Bridge operates outside the Part D benefit, so the $50/month doesn’t apply toward your deductible, initial coverage limit, or true out-of-pocket cap.
Myth 6 — “Compounded semaglutide is covered by BALANCE.”
Reality: Only CMS-listed FDA-approved products and forms are eligible under the Bridge or BALANCE Model. Compounded GLP-1s are not on either drug list.
Dates to watch and what happens after December 31, 2027
| Date | What’s happening |
|---|---|
| Spring 2026 | CMS releases additional Bridge operational guidance (payer sheet, claims processing details) |
| July 1, 2026 | Medicare GLP-1 Bridge launches |
| July 31, 2026 | State Medicaid BALANCE application deadline |
| Oct 15 – Dec 7, 2026 | Medicare Open Enrollment for 2027 |
| January 1, 2027 | Latest scheduled Medicaid BALANCE state start window |
| Oct 15 – Dec 7, 2027 | Medicare Open Enrollment for 2028 |
| December 31, 2027 | Medicare GLP-1 Bridge scheduled end |
| December 31, 2031 | Medicaid BALANCE Model end |
For Medicare beneficiaries
- •Watch for CMS announcements throughout 2027 about Part D plan participation for 2028.
- •Medicare Open Enrollment (Oct 15 – Dec 7, 2027) is when you'd switch plans if BALANCE relaunches and your current plan doesn't participate.
- •If BALANCE doesn't relaunch in Medicare for 2028, Path 3 manufacturer direct programs and Path 4 telehealth options become the practical alternatives.
For Medicaid beneficiaries
- •BALANCE-Medicaid runs through December 31, 2031 independent of the Medicare track.
- •Coverage in your state continues as long as your state Medicaid program continues participation.
- •Many states' applications and start dates won't be public until late 2026 — keep checking the tracker.
Reader friction we found — in their own words
Voice-of-customer quotes from public Medicare and weight-loss forums, used only to identify what people are confused about — not as medical or policy evidence.
“Are you saying this says that we will just pay a $50 copay and nothing else for all doses of Zep?”
— public Reddit thread, r/Zepbound
“Not sure what exactly ‘meet the criteria’ and ‘eligible beneficiaries’ means.”
— public Reddit thread, r/Zepbound
“What is unsaid here is WHO QUALIFIES FOR THAT.”
— public Reddit thread, r/Mounjaro
“I wonder when the states Medicaid programs will start opting in.”
— public Reddit thread, r/GLP1ResearchTalk
“His doc called in the script for Wegovy for his sleep apnea but Medicare denied it. How does all this work?”
— public Reddit thread, r/medicare
We built this guide to be the page that finally gives those questions clean answers. If you read this and still feel uncertain, the quiz routes you to the rest.
Frequently asked questions
The most common follow-up questions from real searches and public forums, with short, direct answers.
1.Is CMS BALANCE the same as the Medicare GLP-1 Bridge?
2.Was the BALANCE Model delayed?
3.When does the Medicare GLP-1 Bridge start and end?
4.Is the Medicare GLP-1 Bridge available in every state?
5.Who qualifies for the $50 Medicare GLP-1 Bridge?
6.Does BMI 30 alone qualify?
7.Does prediabetes qualify?
8.Does sleep apnea qualify for the Bridge?
9.Is Wegovy covered?
10.Is Zepbound covered?
11.Are Ozempic and Mounjaro covered?
12.Are compounded GLP-1s covered?
13.Does the $50 count toward my Part D out-of-pocket cap?
14.Does Extra Help / LIS lower the $50?
15.Can I use a coupon to lower the $50?
16.Who submits the prior authorization?
17.Can a telehealth provider submit the Bridge PA?
18.Will my regular pharmacy accept Bridge prescriptions?
19.Can I use manufacturer direct savings (NovoCare, LillyDirect) if I'm on Medicare or Medicaid?
20.What if my state Medicaid hasn't opted into BALANCE?
21.What happens after December 31, 2027?
22.Where do I find the official CMS pages?
How we verified this page
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We built this guide because the existing public coverage of the BALANCE Model — including major news outlets and well-funded policy analysis — is fractured across at least a dozen sources that don’t reconcile cleanly, and several of them are now outdated since the April 21, 2026 announcement.
Primary sources re-verified within the past 7 days
- •CMS BALANCE Model page
- •CMS Medicare GLP-1 Bridge FAQ
- •CMS press release, December 23, 2025
- •CMS HPMS memo, April 21, 2026 (Part D BALANCE delay)
- •KFF: What to Know About the BALANCE Model for GLP-1s in Medicare and Medicaid (March 24, 2026)
- •KFF: Medicaid Coverage of and Spending on GLP-1s (January 2026)
- •KFF: CMS Extends Medicare's Short-Term Bridge Program for GLP-1 Obesity Drug Coverage
- •AHA News: Medicare won't extend GLP-1 coverage via BALANCE Model in 2027, April 22, 2026
- •Avalere Health: BALANCE Model Analysis
- •Reed Smith: BALANCE Model legal framework
- •FDA Novel Drug Approvals 2026 (Foundayo approval)
- •FDA: Wegovy CV indication press release
- •FDA: Zepbound OSA indication press release
- •NovoCare: Wegovy savings offer
- •LillyDirect: Zepbound pricing
Related guides
- Medicare GLP-1 Bridge Program Providers: Who Can Actually Help in 2026?
- Medicare GLP-1 Bridge Application Process 2026: BIN/PCN, PA Attestations, and What to Bring
- How to Qualify for Medicare GLP-1 Bridge Program 2026 — The 4 Gates and 3 BMI Tiers
- Medicare GLP-1 Bridge Program Eligibility 2026: Full Deep Dive
- Does Medicare Cover Zepbound? Complete Coverage Guide
- Does Medicare Cover Wegovy for Weight Loss?
- GLP-1 FDA Approvals Timeline: Every Drug & Date (2005–2026)
· By The RX Index Research Team · Next re-verification: quarterly and after any CMS update. This page is not medical or legal advice. The RX Index may earn affiliate commissions when readers sign up with telehealth providers featured on this page. That includes Ro and Sesame Care. Eligibility recommendations are editorially independent and based on publicly verified CMS rules. Bridge access through your existing doctor pays us nothing — and is the right path for most readers who qualify. Not affiliated with CMS, Medicare, Humana, Novo Nordisk, or Eli Lilly. If something is out of date, let us know and we’ll fix it within 48 hours.