By The RX Index Editorial Team ·
Medicare GLP-1 Bridge Program Providers: Who Can Actually Help in 2026?
Bottom line up front
Medicare GLP-1 Bridge program providers are not a special CMS-approved network. They are licensed clinicians — MDs, DOs, NPs, PAs — who can document your eligibility, write the prescription, and submit the prior authorization to CMS’s central processor. CMS specifically says the prescriber does not need to be enrolled in Medicare. They only need to not be on the CMS Preclusion List.
Three paths cover almost everyone:
- 1.Your existing clinician if they already have your BMI history and diagnosis records.
- 2.A Medicare-accepting online clinic like Form Health, knownwell, or Shapely — if you don't have a current PCP or yours won't help.
- 3.An FDA-approved cash-pay program like Ro — if you can't wait until July 1, 2026, don't qualify for the Bridge clinical tiers, or your doctor declined.
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We are not affiliated with CMS, Medicare, or any of the clinical providers on this page. We are not a medical practice and do not provide medical advice.

What we actually verified for this page
Sources cited inline.
| Item | Status |
|---|---|
| Bridge runs July 1, 2026 → December 31, 2027 (extended after BALANCE Medicare delay) | ✅ Verified — cms.gov BALANCE FAQ, April 2026 |
| Eligible drugs: all formulations of Foundayo®, all formulations of Wegovy®, and Zepbound® KwikPen® only | ✅ Verified — cms.gov |
| Excluded: Zepbound single-dose vial and single-dose pen | ✅ Verified — cms.gov |
| Patient cost: $50 monthly copay (does not count toward Part D TrOOP or $2,100 cap; manufacturer coupons not applied; LIS does not reduce) | ✅ Verified — cms.gov + KFF |
| Manufacturers provide eligible GLP-1 drugs at a net price of $245 per monthly supply | ✅ Verified — cms.gov |
| Central processor: Humana, using the LI NET infrastructure | ✅ Verified — cms.gov |
| Pharmacy claim routing: BIN 028918 / PCN MEDDGLP1BR, Processor SS&C Health, routed through RelayHealth, help desk 844-673-0910 | ✅ Verified — CMS GLP-1 Bridge Payer Sheet (3/16/2026) |
| Compounded medications not allowed on the Bridge claim | ✅ Verified — CMS GLP-1 Bridge Payer Sheet |
| Prescriber requirement: licensed; not on Medicare's Preclusion List; does NOT need Medicare enrollment | ✅ Verified — cms.gov |
| Form Health publicly states it accepts Medicare | ✅ Provider-stated — formhealth.co |
| knownwell publicly states it accepts Medicare and most major commercial insurance nationwide | ✅ Provider-stated — knownwell.co |
| Shapely publicly states it accepts Original Medicare and most Medicare Advantage PPO plans in CA, FL, NY, TX | ✅ Provider-stated — getshapely.com |
| Ro states it currently cannot help coordinate GLP-1 medication coverage for government insurance plans | ✅ Provider-stated — ro.co |
| Bridge-specific PA submission by Form Health, knownwell, Shapely, Ro, or Sesame | Not publicly confirmed as of June 26, 2026. CMS posted operational guidance in Spring 2026, but no telehealth platform has publicly confirmed end-to-end central-processor integration. Confirm directly with each clinic before booking. |
Quick start: which path fits your situation?
| If you are… | Best first move | Why |
|---|---|---|
| Already prescribed Foundayo, Wegovy, or Zepbound by your doctor | Stay with your current clinician | They already have your BMI history, diagnosis records, and a clear paperwork trail |
| New to GLP-1s and on Medicare, with a regular PCP | Start with your PCP | Lowest-friction path; they can usually bill visits through your existing Medicare coverage |
| Need a Medicare-accepting online clinic | Form Health or knownwell | Both publicly accept Medicare nationwide and work with FDA-approved branded medications |
| Live in CA, FL, NY, or TX and want help with insurance navigation | Shapely | Publicly accepts Original Medicare and most MA PPO plans in those states |
| Don't qualify for Bridge tiers or can't wait until July 1, 2026 | Ro (FDA-approved cash-pay) | Month-to-month membership; FDA-approved formulary; useful as a non-Bridge cash-pay backup |
| Considering a compounded GLP-1 telehealth platform | Not a Bridge path | The Bridge covers only FDA-approved Foundayo, Wegovy, and Zepbound KwikPen; compounded products are explicitly disallowed |
Document checklist, doctor script, pharmacy talking points. One page; print it and hand it to your doctor.
Safety checkpoint before any provider link
Foundayo, Wegovy, and Zepbound are prescription medications. Whether they’re appropriate for you is a clinical decision your prescriber makes. These drugs carry meaningful warnings and contraindications, including a boxed warning related to thyroid C-cell tumors and contraindications in personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). Don’t combine GLP-1 medications unless your prescriber specifically directs it. Talk to your doctor before starting or changing any medication. The RX Index is not a medical practice.
What are Medicare GLP-1 Bridge program providers, exactly?
A Medicare GLP-1 Bridge program provider is any licensed medical provider — MD, DO, NP, or PA — who can document your eligibility, write the prescription for an eligible product (Foundayo, Wegovy, or Zepbound KwikPen), and submit a prior authorization request to the Bridge central processor. CMS does not maintain a special “Bridge provider network.”
If you’ve been searching for a directory of approved Bridge clinics, you can stop. There isn’t one. CMS chose to build the Bridge outside the standard Part D benefit on purpose — it operates through a single central processor that any licensed clinician can submit to, regardless of whether that clinician is in your Part D plan’s network or accepts Medicare assignment for their own visits.
The two requirements (and why most clinicians meet them)
1. Licensed to prescribe the specific Bridge-eligible product in your state.
Standard prescribing authority. NPs and PAs count where state law permits. Almost every working primary care or obesity medicine clinician meets this for Foundayo, Wegovy, and Zepbound KwikPen.
2. Not on Medicare’s Preclusion List.
The Preclusion List is CMS’s list of providers precluded from Medicare Advantage items/services or Part D drug payment. The list isn’t publicly searchable — CMS makes it available to MA and Part D plans. If you want to confirm a specific prescriber, ask the clinic directly, or ask your Part D or MA-PD plan to verify.
That’s it. Those are the federal requirements.
The hidden rule that breaks most articles
Competitors keep flattening this: does the provider have to accept Medicare?
For Bridge medication coverage: no. CMS is explicit on that. For everything else around the Bridge — the office visit, the labs, the follow-up — yes, it matters a lot. If you go to an out-of-network clinic, the medication might still process at $50 through your pharmacy, but the visit might cost $200–$400 out of pocket. That’s the trap a lot of people will fall into when telehealth GLP-1 platforms market “Bridge support” without explaining what they will and won’t bill to Medicare.
Our framing throughout this guide: separate the medication path from the visit path. They run on different rules.
One honest caveat before you keep reading
CMS releases the operational guidance for provider PA submissions in Spring 2026. As of June 2026, the central processor’s submission portal details and provider outreach materials are still rolling out. That means no telehealth platform has publicly confirmed integration with the central processor yet. We mark every “supports Bridge PA submission” claim as unconfirmed — and we mean it. Confirm directly before you book.
Document checklist, doctor script, pharmacy talking points. One page; print it and hand it to your doctor.
Who qualifies for the Medicare GLP-1 Bridge?
To use the Medicare GLP-1 Bridge, you need to be enrolled in a standalone Part D Prescription Drug Plan (PDP) or a Medicare Advantage plan with drug coverage (MA-PD) for calendar year 2026. You also need to meet one of three clinical tiers based on BMI and qualifying conditions, measured at the time GLP-1 therapy was initiated — not necessarily your BMI today.
Plan eligibility
You’re eligible if enrolled in:
- ✓A standalone Part D Prescription Drug Plan (PDP)
- ✓A Medicare Advantage plan with prescription drug coverage (MA-PD) — HMO, HMOPOS, Local PPO, or Regional PPO
- ✓A Special Needs Plan (SNP)
- ✓An employer/union group waiver plan (EGWP)
- ✓The Limited Income Newly Eligible Transition (LI NET) program
- ✓Dual-eligible (Medicare + Medicaid), if enrolled in one of the above plan types
You’re not eligible if only enrolled in:
- ✗Original Medicare with no Part D drug plan
- ✗Private fee-for-service (PFFS) without a separate PDP
- ✗Section 1876 cost contracts
- ✗Section 1833 health care prepayment plans
- ✗PACE organizations ⚠️ (see PACE warning — contact your PACE organization before making any changes)
- ✗Fallback plans
- ✗Religious fraternal benefit plans
If you’re not sure which type of plan you have, call 1-800-MEDICARE (1-800-633-4227) or check at Medicare.gov.
Clinical eligibility — the three tiers
CMS lists three pathways. You only need to meet one.
| Tier | BMI at therapy initiation | Additional condition? | Qualifying conditions |
|---|---|---|---|
| Tier 1 | ≥ 35 | None | (BMI alone is enough) |
| Tier 2 | ≥ 30 | One of: | Heart failure with preserved ejection fraction (HFpEF); uncontrolled hypertension (systolic >140 or diastolic >90 on two antihypertensives); OR chronic kidney disease stage 3a or above |
| Tier 3 | ≥ 27 | One of: | Prediabetes (per ADA criteria); prior myocardial infarction; prior stroke; OR symptomatic peripheral artery disease |
Source: CMS Medicare GLP-1 Bridge FAQ. For reference: a 5’6” person at 217 lbs has a BMI of approximately 35. A 5’10” person at 209 lbs has a BMI of approximately 30.
“Therapy initiation” — the nuance most people miss
CMS evaluates eligibility based on your BMI at the time you started GLP-1 therapy, not your BMI on the day of the prior authorization request. If you’ve already been on a GLP-1 for two years and have lost 60 pounds, your current BMI might be 26 — which would normally disqualify you. But if your BMI was 37 when you started, you still qualify under Tier 1. CMS’s example in their official FAQ describes exactly this scenario.
Practical implication: Dig up your old records. Pre-treatment BMI, weight history, lab results, diagnosis codes from the visit when GLP-1 therapy started. If you switched doctors mid-treatment, request records from the original prescriber. That documentation is what your provider needs in the Bridge prior authorization.
Document checklist, doctor script, pharmacy talking points. One page; print it and hand it to your doctor.
Which medications are covered through the Medicare GLP-1 Bridge?
The Medicare GLP-1 Bridge covers all formulations of Foundayo®, all formulations of Wegovy®, and only the KwikPen® formulation of Zepbound® when prescribed for weight loss. Zepbound single-dose vial and single-dose pen are explicitly not available through the Bridge. Compounded GLP-1 medications are not covered.
What’s included — by product and NDC code
CMS publishes specific National Drug Codes (NDCs) eligible under the Bridge. These are the codes your pharmacy uses to route the claim. Worth printing.
Foundayo® (orforglipron) — all formulations
0002-4178-31 · 0002-4503-31 · 0002-4794-31 · 0002-4803-31 · 0002-4839-31 · 0002-4953-31
Wegovy® (semaglutide) — all formulations (injection and tablet)
0169-4525-14 · 0169-4505-14 · 0169-4501-14 · 0169-4517-14 · 0169-4524-14 · 0169-4415-31 · 0169-4404-31 · 0169-4409-31 · 0169-4425-31 · 0169-4572-14
Zepbound® (tirzepatide) — KwikPen formulation only
0002-3566-11 · 0002-3555-11 · 0002-3544-11 · 0002-3533-11 · 0002-3522-11 · 0002-3511-11
Source: CMS Medicare GLP-1 Bridge eligible drugs and NDCs at cms.gov. CMS may update this list.
| Product / formulation | Bridge-eligible? |
|---|---|
| Zepbound® single-dose vial | ❌ No — explicitly excluded by CMS |
| Zepbound® single-dose pen | ❌ No — explicitly excluded by CMS |
| Compounded semaglutide | ❌ No — compounds not allowed on Bridge claims |
| Compounded tirzepatide | ❌ No — compounds not allowed on Bridge claims |
| Ozempic, Mounjaro, Rybelsus | ❌ Not on Bridge list — may be covered via standard Part D for approved indications other than weight loss |
Indication routing — Bridge vs. standard Part D
A GLP-1 prescription for weight loss goes through the Bridge, but the same medication for a different FDA-approved indication goes through your regular Part D plan.
| Use case | Pathway |
|---|---|
| Wegovy for weight loss / weight maintenance | Bridge (if you qualify) |
| Wegovy for cardiovascular risk reduction in adults with established CV disease | Standard Part D |
| Zepbound KwikPen for weight loss / weight maintenance | Bridge (if you qualify) |
| Zepbound for moderate-to-severe obstructive sleep apnea in adults with obesity | Standard Part D |
| Foundayo for weight loss / weight maintenance | Bridge (if you qualify) |
| Ozempic for type 2 diabetes | Standard Part D |
| Mounjaro for type 2 diabetes | Standard Part D |
| Compounded GLP-1 for weight loss | Cash-pay only (not Bridge, not Part D) |
Who is the best provider path for the Medicare GLP-1 Bridge?
For most people, the best first move is the clinician who already prescribed your medication or your existing primary care doctor. We are deliberately not naming a single “best” provider — the right answer depends on whether you already have a doctor, what plan you’re on, and where you live.
Path 1: Your current clinician
This is the cheapest, fastest path for most readers. If you’ve ever been prescribed a GLP-1, your existing clinic already has your BMI history (the key Tier 1/2/3 documentation), your diagnosis records, your medication history, your current labs, and a working pharmacy on file.
What they may not have yet is awareness of the Bridge workflow. CMS is conducting provider outreach in Spring 2026, but if your clinic hasn’t seen the materials yet, you may have to walk them through it yourself. That sounds like a problem. It’s actually a reason this path still wins — your existing clinic already has every record they’d need; you just bring them the script and the documentation checklist.
Path 2: A Medicare-accepting online clinic
When your current doctor isn’t an option, three online clinics stand out for Medicare-facing care: Form Health, knownwell, and Shapely. All three publicly accept Medicare in some form. None has publicly confirmed Bridge-specific PA integration yet — confirm directly before booking.
Path 3: A cash-pay FDA-approved telehealth program
For readers who can’t wait until July 1, 2026, don’t qualify for the Bridge clinical tiers, or whose doctor declined. Ro is the cleanest fallback — FDA-approved Foundayo, Wegovy, and Zepbound on a month-to-month basis, with no long-term contract.
Which online GLP-1 providers look most Bridge-ready right now?
Form Health, knownwell, and Shapely are the strongest publicly verifiable Medicare-facing online GLP-1 providers as of June 2026. Ro is the best non-Bridge fallback for readers who need FDA-approved cash-pay options.
Form Health — strongest online Medicare-facing candidate
Best for
- •Medicare beneficiaries who want a dedicated obesity medicine team
- •People who don't have a current PCP willing to prescribe
- •Readers who want clinical follow-up beyond just the prescription
- •Anyone who specifically wants FDA-approved-only care
What we verified
- ✓Accepts Medicare and most major commercial insurance (formhealth.co)
- ✓Bills visits, labs, and medications through insurance when applicable
- ✓FDA-approved medications only (no compounded GLP-1s)
- ✓Self-pay option exists if insurance not accepted in your state
Patient care experience quotes
“They are always pleasant, available and professional.” — Clinton C.
“It’s so convenient to set up appts and get questions/concerns answered!” — Mary D.
Quotes from Form Health’s public testimonials page. Presented as care-experience quotes — not as evidence of medication effectiveness or typical weight-loss results. Individual results vary.
knownwell — best nationwide Medicare-friendly virtual and in-person care
Best for
- •Medicare beneficiaries in states without a strong local obesity-medicine option
- •Readers who like the mix of virtual care plus in-person where available
- •Anyone who wants both weight management and broader primary-care coverage in one place
What we verified
- ✓Accepts Medicare and most major commercial insurance nationwide (knownwell.co)
- ✓Virtual care available where in-person locations are not nearby
- ✓FDA-approved branded medications
Shapely — best regional fit for Medicare and MA PPO patients in 4 states
Best for
- •Medicare beneficiaries in California, Florida, New York, or Texas
- •People on Medicare Advantage PPO plans who want insurance navigation help
- •Readers who'd benefit from a clinic that builds insurance support into the model
What we verified
- ✓Accepts Original Medicare and most Medicare Advantage PPO plans in CA, FL, NY, TX (getshapely.com)
- ✓Provides insurance navigation and prior authorization support as part of the service
- ✓Membership cost does not include medication or labs
- ✓For Bridge purposes, only Shapely's FDA-approved brand-name medication path applies — not their self-pay compounded options
Ro — strongest FDA-approved cash-pay backup, not a Bridge-primary pick
| Item | Verified detail (June 11, 2026) |
|---|---|
| Body Program first month | $39 |
| Ongoing monthly | $149/mo, or as low as $74/mo with annual prepay |
| Medication | Billed separately at FDA-approved cash-pay pricing |
| FDA-approved formulary | Foundayo pill, Wegovy pill, Wegovy pen, Zepbound pen, Zepbound KwikPen |
| Government insurance coordination | Not currently available |
| Long-term contract | No — month-to-month |
Note on formulation: If you’re using Ro as a cash-pay bridge to the actual Bridge later, ask your Ro clinician for the KwikPen formulation of Zepbound — that’s the only Zepbound version eligible when you transition.
Damaging admission, done honestly: Ro is more expensive than the Bridge will be. If you qualify for the Bridge, the Bridge wins on price every single time. $50/month vs. Ro membership plus medication is not close.
Disclosure: The RX Index may earn a commission. Ro is a cash-pay fallback, not a Bridge path.
What we are intentionally not featuring on this page
Compounded GLP-1 telehealth platforms. They prescribe compounded semaglutide or tirzepatide — not Foundayo, Wegovy, or Zepbound. The Medicare GLP-1 Bridge covers only the FDA-approved products CMS lists, and the CMS GLP-1 Bridge payer sheet explicitly disallows compounds on Bridge claims. The FDA has separately issued warnings about unapproved GLP-1 products. If you are exploring compounded GLP-1s as a separate cash-pay decision, that is a different conversation — but it is not a Bridge path.
Med spas. Most med spas don’t process Medicare and aren’t structured to submit Bridge prior authorizations. Theoretically possible, practically rare.
Do providers have to accept Medicare to submit Bridge paperwork?
No — not for the Bridge medication itself. CMS says the prescriber doesn’t need to be enrolled in Medicare to submit a Bridge prior authorization, only that they must not be on the Preclusion List. But Medicare acceptance still matters for visit costs, lab fees, and ongoing care, which run on a separate billing track from the Bridge medication.
| Question | Answer |
|---|---|
| Does the provider need to accept Medicare for the Bridge medication to be covered at $50? | No. CMS does not require Medicare enrollment to submit a Bridge PA. |
| Does Medicare acceptance still matter? | Yes — for the visit, the labs, and any ongoing care. Those bill separately. |
| Does the provider need to be a licensed medical clinician? | Yes. They need authority to prescribe the eligible product and document eligibility. |
| Can a telehealth provider submit a Bridge PA? | Potentially yes — if they support the workflow. Confirm directly. |
| Can a provider on the CMS Preclusion List submit a Bridge PA? | No. The drug would not be coverable. |
What this means in practice — two scenarios
Scenario A — In-network PCP
You see your in-network PCP. They submit the Bridge PA. The medication processes at $50/month at your pharmacy. Your visit is covered by Medicare at your normal copay (often $0–$20). Your follow-up labs are covered.
Total out-of-pocket: $50/month medication + small visit copay every few months.
Scenario B — Out-of-network online clinic
You see an out-of-network online clinic that “supports the Bridge.” They submit the Bridge PA. The medication still processes at $50/month at your pharmacy. But the visit is $200 cash-pay. Labs are billed separately. Membership might be $99/month.
Total out-of-pocket: $50 medication + $99 membership + $200 visit + lab costs.
The medication path is identical. The visit path is everything.
What to ask any provider before you book
“Hi — I’m a Medicare beneficiary and I’m asking about the Medicare GLP-1 Bridge program. I have two questions before I book.
1. Will your clinicians submit a prior authorization for the Bridge to CMS’s central processor for an eligible Part D beneficiary? If not, do you support standard Part D prior authorizations for indications like type 2 diabetes or sleep apnea?
2. Are your visits and follow-up labs billed to Medicare directly, or do I pay cash for the visit even if my medication runs through the Bridge?”
Two questions. The clinic’s answers tell you whether they’re a fit.
Document checklist, doctor script, pharmacy talking points. One page; print it and hand it to your doctor.
How does the Medicare GLP-1 Bridge prior authorization actually work?
Your provider submits the Bridge prior authorization request and prescription to a single CMS central processor — not to your Part D plan. CMS has selected Humana to operate the central processor, using the existing LI NET infrastructure. Once the PA is approved, your pharmacy submits the claim using BIN 028918 and PCN MEDDGLP1BR.
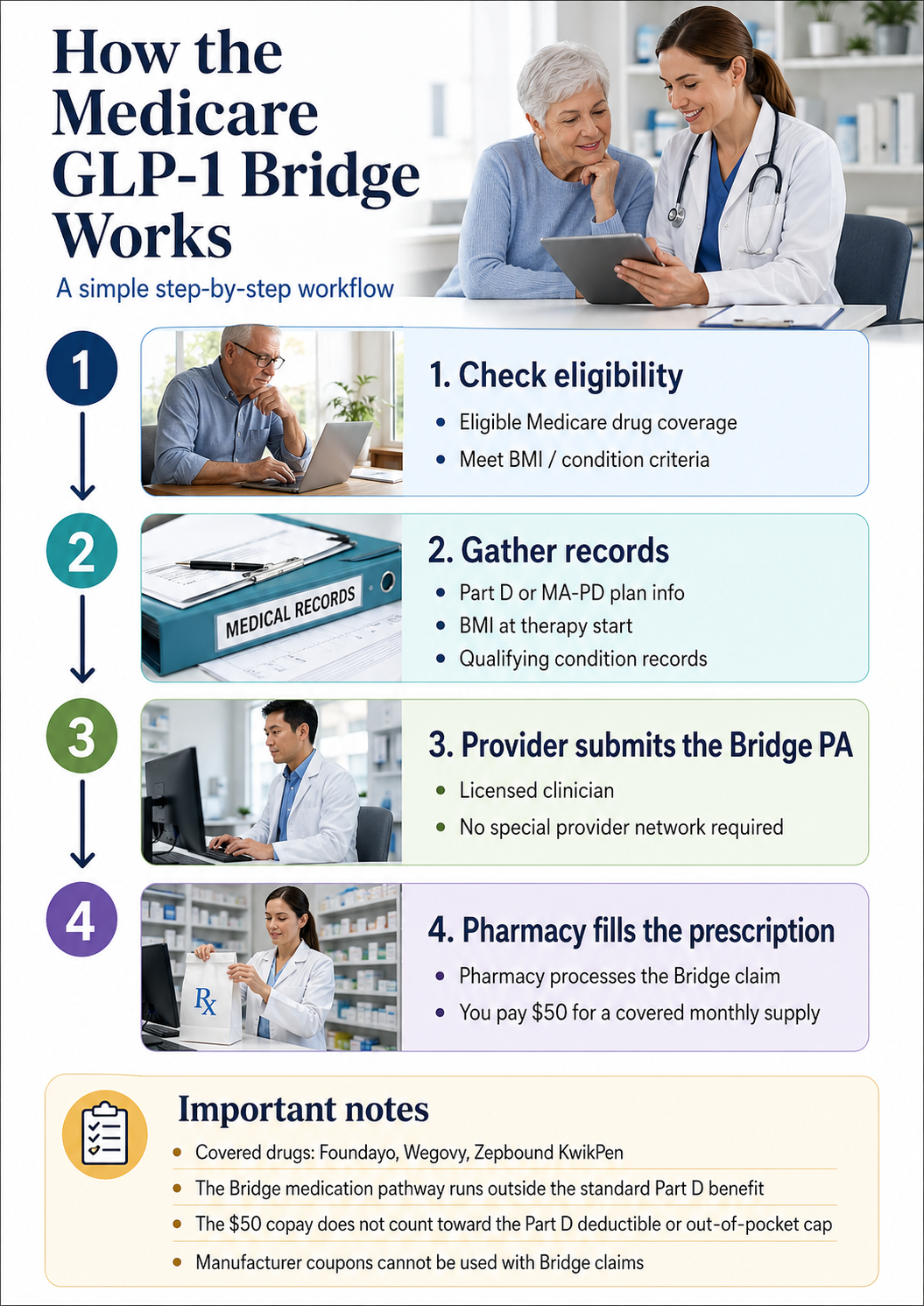
The plain-English workflow
- 1
You confirm you likely qualify — one of three BMI/condition tiers, on an eligible Part D plan.
- 2
Your provider documents — your BMI at therapy initiation, qualifying condition if applicable, and current medication need.
- 3
Your provider submits the Bridge PA — to the CMS central processor. This is not the same submission as a regular Part D prior authorization. CMS will release detailed submission portal instructions in Spring 2026.
- 4
The central processor reviews the PA — Bridge-specific turnaround targets have not been published as of June 2026.
- 5
Your pharmacy fills the prescription — using BIN 028918 and PCN MEDDGLP1BR. Pharmacies don't need to opt in — CMS will provide processing instructions to all pharmacies in the coming months.
- 6
You pay $50 — at pickup.
Pharmacy payer-sheet details — print this and keep it with your Medicare card
| Field | Value |
|---|---|
| Plan / Group Name | GLP1Bridge |
| BIN | 028918 |
| PCN | MEDDGLP1BR |
| Processor | SS&C Health |
| Routing | All claims routed through RelayHealth |
| Provider Relations Help Desk | 844-673-0910 |
| Effective | July 1, 2026 |
| Compounds allowed? | No — compounds not allowed on Bridge claims |
Source: CMS GLP-1 Bridge Payer Sheet, NCPDP Version D, dated March 16, 2026. Verify against the current CMS payer sheet before your first fill.
Pharmacy script — for the day your prescription is ready
“This is a Medicare GLP-1 Bridge prescription, not a standard Part D claim. The Bridge uses BIN 028918 and PCN MEDDGLP1BR. The processor is SS&C Health, routed through RelayHealth. The CMS payer sheet is dated March 16, 2026 and is on cms.gov. The provider relations help desk is 844-673-0910. Can you check your processing instructions?”
What if you’re denied?
The Bridge does not modify your Part D appeal rights. CMS will release more details on Bridge-specific appeal pathways in Spring 2026. Practical first step if you’re denied: have your provider re-document the qualifying tier explicitly. The most common denial reason we expect to see is incomplete BMI-at-therapy-initiation documentation.
Document checklist, doctor script, pharmacy talking points. One page; print it and hand it to your doctor.
What should you bring before asking a provider for Bridge help?
Walk in with documentation, not just intent. Bring your Medicare Part D card, your BMI at the time GLP-1 therapy started (or your starting weight and height if you’ve never been on one), records of any qualifying conditions, current medication list, and any prior authorization or denial letters from previous attempts. This is the single biggest thing you can do to avoid a denied first PA submission.
| Document | Why it matters |
|---|---|
| Medicare Part D plan information | Confirms eligibility plan type and pharmacy processing |
| Medication name and formulation (Foundayo, Wegovy, or Zepbound KwikPen) | Bridge eligibility is drug- and formulation-specific |
| BMI at GLP-1 therapy initiation | The qualifying number for all three Bridge tiers |
| Current BMI | Useful for clinical follow-up |
| Records of qualifying diagnoses | Required for Tier 2 and Tier 3 |
| Prior GLP-1 prescription history | Establishes therapy history |
| Prior PA approvals or denials | Helps your provider avoid repeating mistakes |
| Pharmacy name and location | Needed for claim routing |
| Current medication list | Safety and interaction review |
| Recent labs (A1C, kidney function, lipid panel) | Provider may require for clinical decision-making |
The full checklist also includes:
- •The exact CMS three-tier eligibility language so your doctor sees what they need to attest to
- •A doctor visit script for Medicare beneficiaries
- •A pharmacy script with the BIN, PCN, processor, and help desk number
- •The CMS payer sheet details in print so your pharmacy doesn't have to hunt for them
- •What to do if denied — three-step appeal pathway
Document checklist, doctor script, pharmacy talking points. One page; print it and hand it to your doctor.
How much does the Bridge cost, and what does the $50 copay not cover?
The Medicare GLP-1 Bridge medication copay is $50 per monthly supply. That’s the medication cost — not your visit cost, not labs, not the membership fee for any telehealth platform. The $50 copay does not count toward your Part D deductible, does not count toward the $2,100 Part D out-of-pocket cap, cannot be reduced by manufacturer coupons, and is not eligible for the Part D Low-Income Subsidy.
| Issue | What it means for you |
|---|---|
| Coupons cannot be applied | Novo Nordisk and Eli Lilly's manufacturer savings programs already exclude government insurance — the Bridge codifies that in the program rules. |
| No paper or direct-member reimbursement | Pharmacies must submit electronically through the central processor. If your pharmacy can't or won't, you can't pay out-of-pocket and submit for reimbursement. Find a pharmacy that processes correctly. |
| Copay does not count toward Part D TrOOP | The True Out-of-Pocket cost calculation under Part D — the one that determines when you hit the $2,100 cap — does not include this $50. Your other prescriptions still need to do that work. |
| Low-Income Subsidy doesn't apply | If you qualify for LIS on your other Part D prescriptions, that subsidy doesn't reduce your Bridge copay. The $50 is the same for everyone. |
| Visit and lab costs are separate | Whatever your provider bills for the visit and any labs runs through your normal Medicare or Medicare Advantage benefits. The Bridge handles only the medication. |
Cost comparison — verified base values
| Path | Medication | Visit / membership |
|---|---|---|
| Bridge + existing clinician | $50/mo = $600/year | Plan-specific Medicare visit and lab costs |
| Bridge + Medicare-accepting online clinic | $50/mo = $600/year | Plan-specific or self-pay visit and lab costs; varies by clinic |
| Cash-pay Ro Body Program (no Bridge) | Medication billed separately at FDA-approved cash-pay pricing | $39 first month + $149/mo ongoing, or as low as $74/mo with annual prepay |
| Standard Part D (for diabetes, CV risk, or sleep apnea) | Plan copay (varies by plan and tier; counts toward $2,100 OOP cap) | Standard Medicare visit copay |
The math is clear: the Bridge is dramatically cheaper than any cash-pay path if you qualify. The cash-pay path only makes sense for readers who don’t qualify, can’t wait, or have specific reasons (their doctor declined, they want to try the program before July 2026 launch).
What if your doctor, your plan, or your pharmacy is confused?
Confusion is likely, especially in the first six months of the program. The fastest fix is to identify which step is broken and address that step specifically. Here are scripts for the four most common confusion points.
"My doctor said Medicare doesn't cover weight-loss drugs"
That answer is incomplete for Bridge-eligible prescriptions starting July 1, 2026. Standard Part D still doesn't cover obesity-only prescriptions in the usual way, but the Bridge is a CMS demonstration that operates outside the standard Part D benefit, designed exactly to fill this gap.
"I understand that standard Part D excludes weight-loss medications. I'm asking specifically about the Medicare GLP-1 Bridge — that's CMS's demonstration program for eligible Part D beneficiaries that runs from July 2026 through December 2027. The prior authorization goes through CMS's central processor, not through my Part D plan. Can your office submit the Bridge PA?"
"My Part D plan denied it"
The Bridge PA does not necessarily route through your Part D plan in the standard way. A standard Part D denial may not be a Bridge denial. CMS strongly encourages Part D sponsors to return a message directing the provider to the central processor when a Bridge request is mistakenly submitted to the Part D plan.
"Was this denial issued by my Part D plan or by the CMS Bridge central processor? Those are separate review pathways. If the denial came from my Part D plan, my doctor needs to submit the PA to the central processor instead. The Bridge runs outside the Part D benefit."
"My pharmacy can't process it"
The pharmacy needs to use the Bridge-specific BIN, PCN, and processor. If they're processing it as a standard Part D claim, it'll bounce.
"This is a Bridge claim, not a standard Part D claim. The BIN is 028918 and the PCN is MEDDGLP1BR. The processor is SS&C Health, routed through RelayHealth. The CMS GLP-1 Bridge payer sheet is dated March 16, 2026. If you need help, the provider relations help desk is 844-673-0910."
"The telehealth clinic I called only does commercial insurance"
Some online GLP-1 platforms only handle commercial insurance and cash-pay — not Medicare. That's a clean disqualification.
- 1.Ask your existing PCP first. (Cheapest path; almost always works.)
- 2.Try Form Health or knownwell — both publicly accept Medicare nationwide.
- 3.If you're in CA, FL, NY, or TX on a Medicare Advantage PPO plan, try Shapely.
- 4.If none of those work and you can't wait, Ro's FDA-approved cash-pay options are a stopgap — but remember Ro can't coordinate government insurance coverage.
Document checklist, doctor script, pharmacy talking points. One page; print it and hand it to your doctor.
What happens after December 31, 2027?
As of CMS’s most recent guidance, the Medicare GLP-1 Bridge runs through December 31, 2027. CMS originally planned for the BALANCE Model to take over starting January 1, 2027. On April 21, 2026, CMS announced that BALANCE would not implement in Medicare Part D in 2027, and the Bridge was extended through 2027 to continue coverage. What happens after December 2027 has not yet been announced.
If you saw headlines about “BALANCE delayed” in late April 2026 and panicked:
You’re getting more time, not less. The original 6-month bridge has been extended to a roughly 18-month program. The original Bridge would have ended December 2026. Now it runs through December 2027.
What to monitor through 2027
- •CMS Bridge page updates (cms.gov/medicare/coverage/prescription-drug-coverage/medicare-glp-1-bridge)
- •Medicare Open Enrollment (October 15 – December 7 each year) — Part D plans may add or change GLP-1 coverage
- •Your Part D plan's annual notice of change — sent each fall
- •Provider-side updates from any telehealth platform you're using
- •Eligible drug and NDC list — CMS may update which products and formulations are covered
What to do now if you’re worried about post-2027 coverage
Lock in the Bridge while it exists. Eighteen months of coverage at $50/month is meaningful even if 2028 is uncertain.
Stay enrolled in a Part D plan during 2027 open enrollment. CMS has signaled that any longer-term GLP-1 Medicare program will likely flow through Part D plans, so plan enrollment is the foundation.
Build a backup plan. If you've found a cash-pay path you trust, keep that relationship warm.
Frequently asked questions about Medicare GLP-1 Bridge program providers
Who can submit a Medicare GLP-1 Bridge prior authorization?
Can I check the CMS Preclusion List myself?
Can a telehealth provider submit the Medicare GLP-1 Bridge prior authorization?
Do Medicare GLP-1 Bridge providers have to accept Medicare?
Which online GLP-1 providers accept Medicare?
Which medications are included in the Medicare GLP-1 Bridge?
Is Foundayo included in the Medicare GLP-1 Bridge?
Is Zepbound KwikPen different from Zepbound vial or single-dose pen for the Bridge?
Are Ozempic and Mounjaro included in the Bridge?
Are compounded GLP-1 medications covered by the Medicare GLP-1 Bridge?
Can Ro help with Medicare or government insurance coverage for GLP-1s?
Does the $50 Bridge copay count toward my Part D out-of-pocket cap?
Can I use a manufacturer coupon with the Bridge?
What payer sheet details should my pharmacist use for the Bridge?
What if my doctor says Medicare doesn't cover weight-loss drugs?
What if I started a GLP-1 before I went on Medicare?
What if I'm currently paying over $1,000/month out of pocket for Wegovy or Zepbound?
What happens after December 31, 2027?
Recap and your next move
1. Your existing clinician is usually the best Bridge path if they’re licensed to prescribe Foundayo, Wegovy, or Zepbound KwikPen, are willing to submit the Bridge PA, and you meet CMS criteria. No special network. No special enrollment.
2. If you need an online clinic, Form Health, knownwell, and Shapely are the strongest publicly verifiable Medicare-facing options. Confirm Bridge-specific PA support directly with each clinic before booking.
3. The Bridge is dramatically cheaper than any cash-pay path if you qualify. Cash-pay through Ro is the right call only if you don’t qualify, can’t wait, or your doctor declined.
How we built this guide
We compared CMS Medicare GLP-1 Bridge rules, the CMS GLP-1 Bridge payer sheet (NCPDP claim billing/rebill payer sheet, dated 3/16/2026), the CMS BALANCE Model FAQ, FDA statements on FDA-approved versus compounded drugs, manufacturer savings program restrictions, KFF policy analysis, NCPA pharmacy guidance, and public provider pages. We separated three claim types throughout: (1) verified CMS rules, cited to cms.gov directly; (2) provider-stated commercial facts, cited to each provider’s public site; and (3) editorial judgments — including which provider path fits which reader — explicitly framed as our editorial conclusions based on the verified facts above.
We flagged Bridge-specific provider integration as unconfirmed everywhere we couldn’t confirm it directly, because we’d rather be useful and transparent than confident and wrong.
Material connections: The RX Index earns affiliate commissions when readers sign up with certain telehealth providers, including Form Health, knownwell, Shapely, Ro, and Sesame Care. Bridge access through your existing doctor pays us nothing — and is the cheapest path for most readers, which is why we recommend it first.
Sources
- Centers for Medicare & Medicaid Services — Medicare GLP-1 Bridge
- CMS GLP-1 Bridge Payer Sheet (NCPDP Version D, dated 3/16/2026)
- CMS — BALANCE Model FAQ
- CMS — Preclusion List overview
- KFF — What Medicare's Temporary Program Covering GLP-1s for Obesity Means for Beneficiaries
- KFF — CMS Extends Medicare's Short-Term Bridge Program for GLP-1 Obesity Drug Coverage (April 2026)
- NCPA — CMS kicks the can on weight loss GLP-1 drugs (April 23, 2026)
- Reuters — Delay in Medicare pilot for obesity drugs may not hurt near-term demand
- Form Health — FAQs (Medicare acceptance)
- knownwell — Insurance
- Shapely — Medicare Coverage
- Ro — Body Program (sponsored affiliate link, opens in a new tab)
- FDA — FDA's Concerns with Unapproved GLP-1 Drugs Used for Weight Loss
- NovoCare — Wegovy Savings Offer
- Zepbound — Savings Options
Related guides
- Medicare GLP-1 Bridge Program Application Process [2026] — BIN/PCN, PA attestations, and what to bring
- How to Qualify for Medicare GLP-1 Bridge Program 2026 — the 4 gates and 3 BMI tiers
- Medicare GLP-1 Bridge Program Eligibility: Full Deep Dive
- Does Medicare Cover Zepbound? Complete Coverage Guide
- Does Medicare Cover Wegovy for Weight Loss?
- GLP-1 FDA Approvals Timeline: Every Drug & Date (2005–2026)
· By The RX Index Editorial Team · Next re-verification: quarterly and after any CMS update. This page is not medical or legal advice. The RX Index is not affiliated with CMS, Medicare, Humana, Form Health, knownwell, Shapely, Ro, Novo Nordisk, or Eli Lilly. If something here is out of date, please let us know and we’ll fix it within 48 hours.