By The RX Index Editorial Team · · Next review: September 11, 2026 or upon CMS guidance update
Medicare Bridge Program Prior Authorization Form: What to Use, Who Submits It, and What CMS Has Released So Far (2026)
The bottom line, before you scroll
If you’re searching for a Medicare Bridge Program prior authorization form to download, print, and bring to your doctor — here is what changed as of June 26, 2026: CMS has published the Medicare GLP-1 Bridge prior authorization form. The form is available at cms.gov/glp-1-bridge.pdf; only the prescriber submits it, through CoverMyMeds or fax 1-800-530-2404. This is a prescriber-submitted request, not a patient-fillable form. The Medicare GLP-1 Bridge is a CMS demonstration program that covers Foundayo, Wegovy (all formulations), and Zepbound (KwikPen formulation only) for weight reduction at a flat $50/month copay. It launched July 1, 2026, and CMS extended it through December 31, 2027 on April 21, 2026. The PA is a prescriber-submitted request that goes to a CMS central processor — administered by Humana/LI NET; SS&C Health processes pharmacy claims through RelayHealth.
Quick Route Check
Find your row, then keep reading.
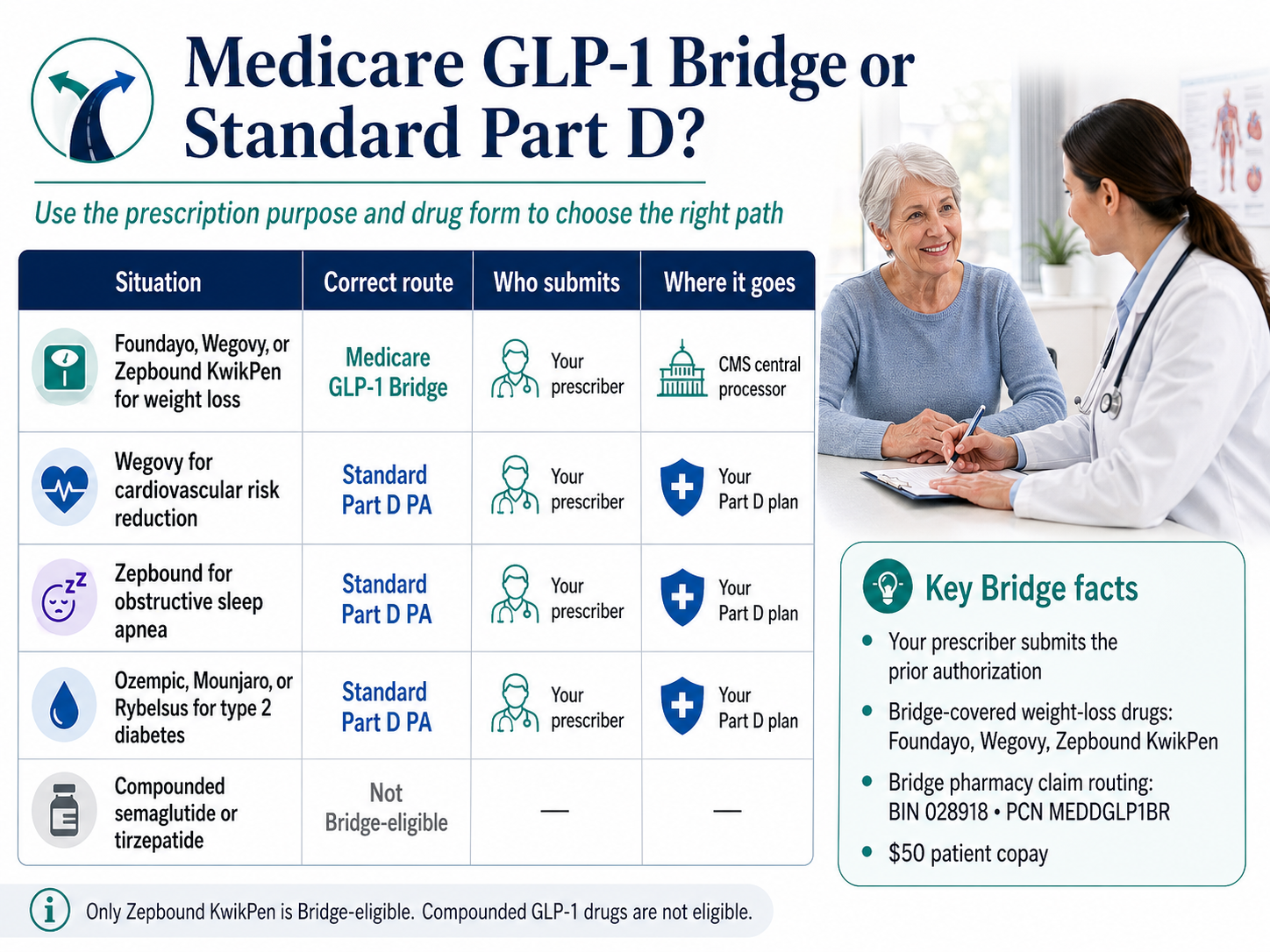
| Your situation | Correct route | Who submits | Where it goes |
|---|---|---|---|
| Foundayo, Wegovy, or Zepbound KwikPen for weight loss | Medicare GLP-1 Bridge | Your prescriber | CMS central processor (Humana / LI NET) |
| Wegovy for CV risk reduction in established CV disease | Standard Part D PA | Your prescriber | Your Part D plan |
| Zepbound for moderate-to-severe OSA with obesity | Standard Part D PA | Your prescriber | Your Part D plan |
| Ozempic, Mounjaro, or Rybelsus for type 2 diabetes | Standard Part D PA | Your prescriber | Your Part D plan |
| Zepbound single-dose vial or single-dose pen | Not Bridge-covered (any indication) | — | Cash pay or Part D for OSA |
| Compounded semaglutide or tirzepatide | Not Bridge-eligible | — | Outside the Medicare GLP-1 Bridge route |
Jump to what you need:
- No patient form to download
- Who submits the PA?
- Plan type eligibility
- Form status tracker (live)
- What your doctor must attest to
- Three BMI tiers explained
- Eligible drugs & NDCs
- Pharmacy BIN/PCN routing
- Cost & what doesn’t apply
- What to bring to your doctor
- Bridge PA vs standard Part D PA
- Six mistakes to avoid
- Denied? Here’s what to do
- Can telehealth help?
- After December 31, 2027
- Copy-paste prescriber & pharmacy scripts
- FAQ (20 questions)
Source: CMS Medicare GLP-1 Bridge official page. Verified July 10, 2026.
Is There a Medicare Bridge Program Prior Authorization Form Patients Can Download?
CMS has published the Medicare GLP-1 Bridge prior authorization form. The form is informational before July 1, 2026 — the prescriber fax submission line is active starting July 1.
The verified workflow is a prescriber-submitted PA request and prescription routed to the CMS central processor (Humana, through LI NET infrastructure). There is no patient-downloadable PA form — submission is handled by your prescriber.
If you’ve been hunting for a PDF, you did the right research with the wrong tool. The Bridge isn’t a normal Part D coverage decision. CMS is using Section 402 demonstration authority to operate the Bridge outside the Part D coverage and payment flow. Your Part D plan doesn’t have to opt in. Your Part D plan isn’t bearing the cost. Your Part D plan isn’t even the decision-maker on a Bridge weight-loss request. That’s why standard Part D coverage-determination forms and plan-specific PA forms are the wrong tool here.
You don’t need to find a form.
You need to bring your doctor the right criteria, the right routing information, and the right records.
If you spent an hour combing CMS.gov for a downloadable PDF, that hour wasn’t wasted
but the search itself is wrong.
The next 10 minutes on this page
are the highest-leverage thing you can do before your appointment.
Who Submits the Medicare Bridge Prior Authorization?
Your medical provider — physician, nurse practitioner, or physician assistant — submits the Bridge PA on your behalf. You cannot submit it yourself. The prescriber does not need to be enrolled in Medicare, but must not appear on the CMS Preclusion List. The PA goes to the central processor (Humana, via LI NET infrastructure), not to your Part D plan.
The submission chain in plain English
You gather your records (listed in the doctor packet section below).
Your prescriber confirms which Bridge route fits — Tier 1 (BMI ≥ 35), Tier 2 (BMI ≥ 30 + qualifying condition), or Tier 3 (BMI ≥ 27 + qualifying condition).
Your prescriber writes the prescription for an eligible drug and submits the PA request to the central processor when CMS publishes the operational submission process.
The central processor reviews the PA against the eligibility criteria.
Once approved, you take the prescription to a pharmacy that submits the claim using the Bridge BIN/PCN routing (BIN 028918, PCN MEDDGLP1BR).
You pay $50 at the counter.
Does the prescriber need special CMS enrollment?
No. Per CMS, the prescriber doesn’t need to be enrolled in Medicare to write a prescription or submit a Bridge PA. The only requirement is that they must not be on the CMS Preclusion List. Most working prescribers in the U.S. are not on it.
Can a telehealth provider submit the Bridge PA?
Possibly, but verify before paying. A licensed telehealth prescriber can in theory submit if they’re licensed in your state, can prescribe the eligible drugs, and have a workflow built for the central processor. Most consumer telehealth GLP-1 platforms don’t yet route through the Bridge. Ask directly: “Do you submit Medicare GLP-1 Bridge PAs to the CMS central processor for Medicare Part D beneficiaries?”
Who Is Eligible Based on Medicare Plan Type?
The Medicare GLP-1 Bridge is nationwide and available in all states and territories. To use it, you must be enrolled in an eligible 2026 Part D plan type. Most beneficiaries with Part D drug coverage qualify by plan type, but several less-common plan structures are excluded unless you’re also enrolled in a standalone Part D plan.
| Medicare plan type | Bridge eligible? |
|---|---|
| Standalone Prescription Drug Plan (PDP) | ✅ Yes |
| Medicare Advantage Prescription Drug plan (MA-PD — HMO, HMO-POS, Local PPO, Regional PPO) | ✅ Yes |
| Special Needs Plans (SNPs) | ✅ Yes |
| Employer / Union Group Waiver Plans (EGWPs) | ✅ Yes |
| Limited Income Newly Eligible Transition (LI NET) | ✅ Yes |
| Original Medicare without Part D | ❌ No |
| Private Fee-for-Service (PFFS) plans | ❌ No (unless also in standalone PDP) |
| Section 1876 cost contract plans | ❌ No (unless also in standalone PDP) |
| Section 1833 health care prepayment plans | ❌ No (unless also in standalone PDP) |
| PACE organizations | ❌ No (unless also in standalone PDP) |
| Fallback plans | ❌ No (unless also in standalone PDP) |
| Religious fraternal benefit plans | ❌ No (unless also in standalone PDP) |
Source: CMS Medicare GLP-1 Bridge official page, verified July 10, 2026.
Dual eligible and LIS / Extra Help beneficiaries
Dually eligible (Medicare + Medicaid) beneficiaries in eligible Part D plan types qualify for the Bridge if they meet the clinical PA criteria. However, Low-Income Subsidy (LIS / Extra Help) cost-sharing does not apply to the $50 Bridge copay — that’s a structural feature of the demonstration, not a mistake on your plan’s part. If you normally pay $0 to $11.20 for other medications, the $50 Bridge copay may feel high. Talk to your doctor about whether a standard Part D covered indication (CV risk, OSA, T2D) routes you through a path where your LIS subsidies do apply.
If you’re not sure which type of Part D plan you have, log in at Medicare.gov, check your plan documents, or call 1-800-MEDICARE (1-800-633-4227).
What CMS Has Released vs. What’s Still Pending — Bridge Form Status Tracker
As of April 27, 2026, CMS has published the eligibility criteria, the eligible drug list with NDCs, the central processor identity, the pharmacy payer sheet, and the Bridge program duration. CMS has not yet published the prescriber-facing operational submission process.
| Status | Item | Most recent CMS source |
|---|---|---|
| ✅ Released | Three-tier eligibility criteria (BMI + conditions) | CMS GLP-1 Bridge FAQ, March 3, 2026 |
| ✅ Released | Eligible drug list (Foundayo, Wegovy all formulations, Zepbound KwikPen) | CMS Bridge page update, April 6, 2026 |
| ✅ Released | Full NDC list for eligible drugs | CMS Bridge page |
| ✅ Released | Pharmacy BIN (028918) and PCN (MEDDGLP1BR) | CMS Bridge page + payer sheet |
| ✅ Released | Pharmacy payer sheet (SS&C Health processor, RelayHealth routing, help desk 844-673-0910) | CMS GLP-1 Bridge payer sheet, March 16, 2026 |
| ✅ Released | Central processor identity (Humana, via LI NET infrastructure) | CMS Bridge page |
| ✅ Released | Bridge duration extended through December 31, 2027 | CMS announcement, April 21, 2026 |
| ✅ Released | $50 patient copay; $245 net price to manufacturers | CMS Bridge page |
| ✅ Released | LIS subsidies do not apply; coupons not allowed; no paper claims; no direct member reimbursement | CMS Bridge page + payer sheet |
| 🟡 Pending | Prescriber-facing PA submission process | CMS: expected Spring 2026 |
| 🟡 Pending | Additional pharmacy claims processing guidance | CMS: expected Spring 2026 |
| 🟡 Pending | Standard PA decision turnaround time | Not specified in current CMS materials |
| 🟡 Pending | Formal Bridge PA appeals process | Not yet released |
| 🟡 Pending | Pharmacy dispensing fee amount | Not specified |
Sources verified April 27, 2026: CMS Medicare GLP-1 Bridge official page; CMS GLP-1 Bridge payer sheet March 16, 2026; CMS extension announcement April 21, 2026.
What Does Your Doctor Have to Attest to on the Bridge PA?
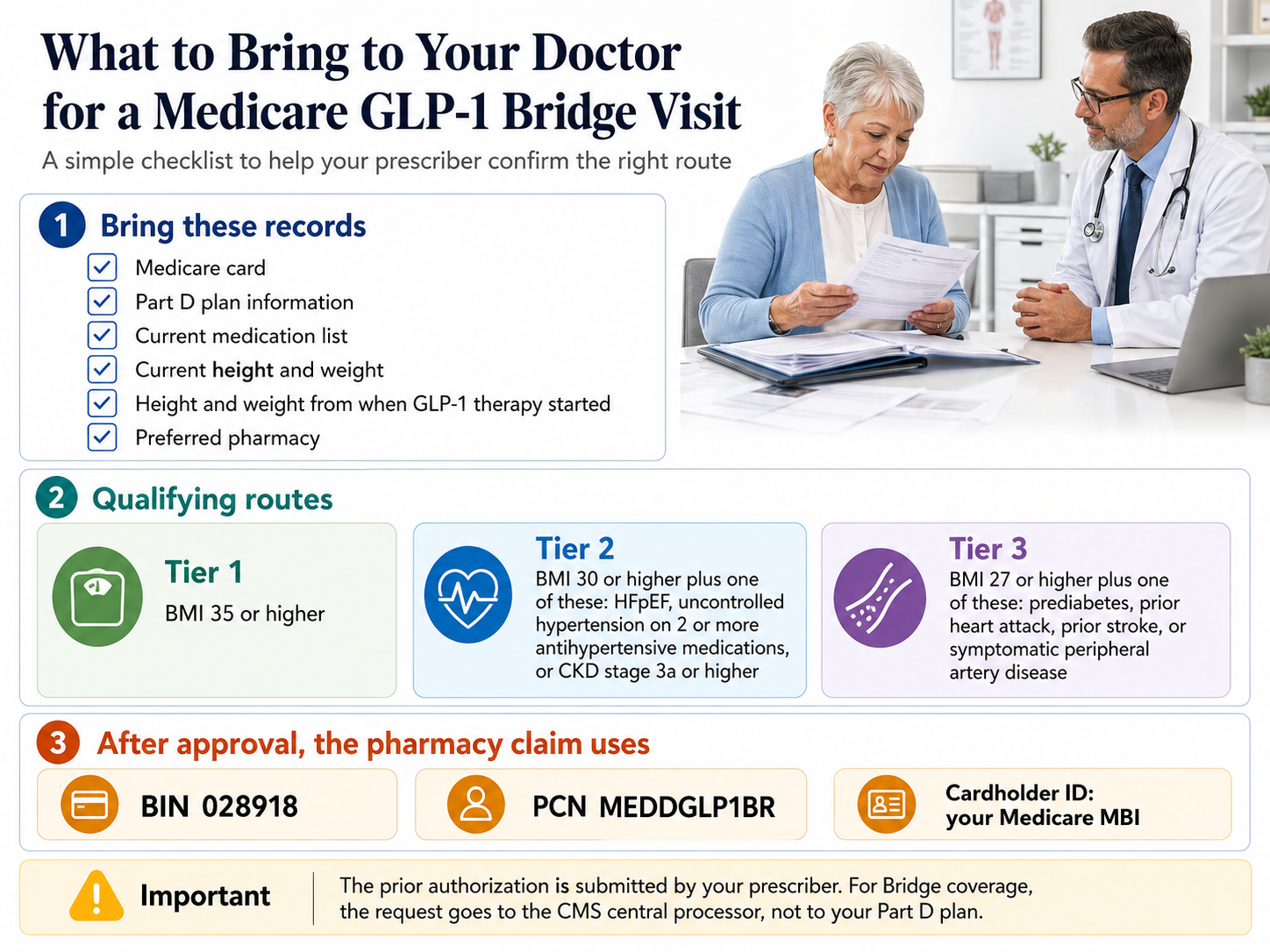
The prescriber must attest that you’re being prescribed an eligible GLP-1 to reduce body weight and maintain weight reduction in combination with ongoing lifestyle modification; that you’re at least 18; and that you meet one of three BMI/diagnosis tiers at the time GLP-1 therapy was initiated — not your current BMI.
Three Eligibility Tiers Explained
| Tier | BMI requirement (at GLP-1 initiation) | Plus one of these conditions | Records that support it |
|---|---|---|---|
| Tier 1 | BMI ≥ 35 | None required | Documented height/weight at the time you started, or current measurement if new to GLP-1s |
| Tier 2 | BMI ≥ 30 | Heart failure with preserved ejection fraction (HFpEF), OR uncontrolled hypertension (SBP > 140 or DBP > 90) on two or more antihypertensive medications, OR chronic kidney disease stage 3a or above | Cardiology note (HFpEF); BP logs + medication list showing ≥2 antihypertensives (HTN); eGFR / nephrology records (CKD) |
| Tier 3 | BMI ≥ 27 | Prediabetes per ADA guidelines, OR prior myocardial infarction, OR prior stroke, OR symptomatic peripheral artery disease (PAD) | A1C / fasting glucose (prediabetes); hospital discharge summary or cardiology/neurology note (MI/stroke); vascular study (PAD) |
You only need to meet one tier. If you meet Tier 1 (BMI ≥35), you don’t need any comorbidity. If you’re between BMI 30 and 35 with one of the Tier 2 conditions, you’re in. Same for Tier 3.
⏰ The BMI-at-initiation rule that nobody talks about
If you’re already on a GLP-1 and you’ve lost weight, your current BMI may be lower than the threshold. But CMS says the criterion is your BMI at the time of GLP-1 therapy initiation. CMS’s own example: a beneficiary who started in September 2024 at BMI 37 and is now BMI 34 still attests to ≥35 because that’s what they were when therapy began. Dig out your old chart records — your doctor’s office should be able to pull height/weight from the original visit.
Which GLP-1 Drugs the Medicare Bridge Actually Covers
The Bridge currently covers Foundayo (all formulations), Wegovy (all formulations — injection and oral tablet), and Zepbound KwikPen formulation only. Zepbound single-dose vials and single-dose pens are explicitly excluded. Ozempic, Mounjaro, Rybelsus, Saxenda, and any compounded GLP-1 are not covered. Drug list last updated by CMS: April 6, 2026.
| Medication | Bridge eligible? | Formulations included | Notes |
|---|---|---|---|
| Foundayo (orforglipron) | ✅ Yes | All formulations | Added April 6, 2026. Once-daily oral tablet. |
| Wegovy (semaglutide) | ✅ Yes | Injection + oral tablet (Wegovy pill) | All formulations included. |
| Zepbound (tirzepatide) — KwikPen | ✅ Yes | KwikPen only | Multi-dose autoinjector pen format. |
| Zepbound — single-dose vial | ❌ No | — | Excluded from Bridge entirely. |
| Zepbound — single-dose pen | ❌ No | — | Excluded from Bridge entirely. |
| Ozempic (semaglutide) | ❌ No | — | Diabetes indication; goes through standard Part D. |
| Mounjaro (tirzepatide) | ❌ No | — | Diabetes indication; goes through standard Part D. |
| Rybelsus (oral semaglutide) | ❌ No | — | Diabetes indication; goes through standard Part D. |
| Saxenda (liraglutide) | ❌ No | — | Not on the Bridge eligible list. |
| Compounded semaglutide / tirzepatide | ❌ No | — | Bridge payer sheet states: “Compounds not allowed.” |
Full NDC list for your pharmacist
Foundayo NDCs: 0002-4178-31, 0002-4503-31, 0002-4794-31, 0002-4803-31, 0002-4839-31, 0002-4953-31
Wegovy NDCs: 0169-4525-14, 0169-4505-14, 0169-4501-14, 0169-4517-14, 0169-4524-14, 0169-4415-31, 0169-4404-31, 0169-4409-31, 0169-4425-31, 0169-4572-14
Zepbound KwikPen NDCs: 0002-3566-11, 0002-3555-11, 0002-3544-11, 0002-3533-11, 0002-3522-11, 0002-3511-11
Source: CMS Medicare GLP-1 Bridge official page, verified April 27, 2026. CMS notes the list may be updated over the course of the demonstration.
Why your indication changes everything
If your prescription is for an indication that’s already coverable under standard Part D — Wegovy for cardiovascular risk reduction in established CV disease, Zepbound (any formulation) for moderate-to-severe OSA, or any GLP-1 for type 2 diabetes — the Bridge does not apply. Your doctor must complete the regular Part D utilization-management process through your plan instead. CMS is monitoring for plans that try to push covered Part D requests onto the Bridge.
The Pharmacy Payer Sheet — What Your Pharmacist Needs
The Bridge pharmacy claim routes electronically through SS&C Health (the processor) via RelayHealth, using BIN 028918 and PCN MEDDGLP1BR, with help desk 844-673-0910. Your Medicare Beneficiary Identifier (MBI) — the number on your red, white, and blue Medicare card — is used as the cardholder ID. Paper claims and direct member reimbursement are not accepted.
| Field | Value |
|---|---|
| Payer name | CMS Medicare Part D |
| Plan / group | GLP1Bridge |
| BIN | 028918 |
| PCN | MEDDGLP1BR |
| Processor | SS&C Health |
| Routing | RelayHealth |
| Effective date | July 1, 2026 |
| Help desk | 844-673-0910 |
| Cardholder ID | Beneficiary’s MBI (from Medicare card) |
| Compounds | Not allowed |
| Paper claims | Not accepted |
| Direct member reimbursement | Not accepted |
| Manufacturer coupons / discount cards | Not allowed |
| Coordination of benefits | Bridge is primary; does not coordinate with other payers |
Source: CMS GLP-1 Bridge payer sheet, March 16, 2026; cross-referenced April 27, 2026.
Pharmacy script you can use
If you walk in on July 5 and your pharmacy charges you $400 instead of $50, say this:
“Could you check whether this is a Medicare GLP-1 Bridge claim instead of a standard Part D claim? CMS published the Bridge payer sheet — BIN 028918, PCN MEDDGLP1BR, plan group GLP1Bridge, processor SS&C Health, routed through RelayHealth, effective July 1, 2026. The help desk is 844-673-0910.”
That sentence will save you an hour at the counter. Print it. Take it.
Does my pharmacy have to opt in to the Bridge?
No. CMS has confirmed that pharmacies do not need to separately opt in. Once CMS publishes additional pharmacy claims processing guidance (expected Spring 2026), most pharmacies that already process Medicare claims will be able to handle Bridge claims using the BIN/PCN routing above. If your preferred pharmacy doesn’t recognize the routing in the first week of July, ask them to call the Bridge help desk at 844-673-0910.
How Much the Bridge Actually Costs (and What Doesn’t Apply)
The Bridge copay is $50/month, the manufacturer net price is $245/month, the copay does not count toward your Part D out-of-pocket cap, manufacturer coupons cannot be used, and Low-Income Subsidy (LIS / Extra Help) cost-sharing does not apply.
| Cost item | Bridge answer |
|---|---|
| Patient copay | $50/month |
| Manufacturer net price (CMS pays the rest) | $245/month |
| Counts toward your Part D deductible? | No |
| Counts toward your Part D out-of-pocket maximum (TrOOP, $2,100 in 2026)? | No |
| LIS / Extra Help reduces the $50? | No — LIS cost-sharing subsidies do not apply to the Bridge |
| Manufacturer coupon / savings card allowed? | No — coupons and discount programs not allowed on Bridge claims |
| Direct member reimbursement available? | No — pharmacy must process electronically |
Sources: CMS Medicare GLP-1 Bridge page; Medicare.gov 2026 Part D cost details; verified April 27, 2026.
What to Bring to Your Doctor — The Pre-Visit Checklist
Bring proof of Medicare Part D enrollment, your current and prior height/weight records, documentation of any qualifying condition for Tier 2 or Tier 3, your current medication list, and the Bridge PA criteria so your doctor can confirm fit and attest correctly. Doctor visits are short. The Bridge is brand-new. The fastest path to an approved PA is walking in with everything pre-organized.
Source: CMS Medicare GLP-1 Bridge eligibility criteria. Verified April 27, 2026.
Universal records (everyone brings these)
Tier-specific records
| If you’re going for… | Bring this | Where to get it |
|---|---|---|
| Tier 1 (BMI ≥ 35) | Documented height/weight at GLP-1 initiation, or current measurement | Prior chart visit, or current visit |
| Tier 2 — HFpEF | Cardiology note documenting HFpEF | Cardiologist’s office |
| Tier 2 — Uncontrolled HTN | BP logs (home or office), current medication list showing two or more antihypertensives | Your records + pharmacy printout |
| Tier 2 — CKD stage 3a+ | eGFR result or nephrology note | Lab portal, PCP, or nephrologist |
| Tier 3 — Prediabetes | A1C or fasting glucose meeting ADA prediabetes thresholds | Lab portal or PCP |
| Tier 3 — Prior MI / Stroke | Hospital discharge summary or cardiology / neurology note | Hospital records or specialist |
| Tier 3 — Symptomatic PAD | Vascular study, ABI, or vascular specialist note | Vascular specialist |
What to say to your prescriber
“I have Medicare Part D coverage, and I think I may meet the CMS Medicare GLP-1 Bridge criteria for weight reduction starting July 1, 2026. Could we review which BMI tier I fit, and if I’m eligible, can your office submit the Bridge prior authorization to the CMS central processor (Humana / LI NET) rather than my Part D plan? Here’s the criteria packet — it has the routing details and the pharmacy payer sheet for your reference.”
That paragraph will save your appointment. Most patients walk in saying “I want Wegovy” and lose half the visit explaining the Bridge. You walk in with the criteria and routing, and the visit becomes about your eligibility — not about the program.
Bridge PA vs. Standard Part D PA — Which One Applies to You?
The Bridge PA only applies when the prescription is specifically for weight loss using one of the three eligible drugs in the eligible formulations. If the same drug is prescribed for an indication coverable under standard Part D, the PA goes through your Part D plan, not the Bridge. The indication on the prescription determines the route.
| Prescription scenario | PA goes to | Cost path |
|---|---|---|
| Wegovy (any formulation) for weight loss | Bridge central processor (Humana) | $50 Bridge copay |
| Wegovy for CV risk reduction in established CV disease + obesity/overweight | Your Part D plan | Plan’s standard cost-share |
| Zepbound KwikPen for weight loss | Bridge central processor (Humana) | $50 Bridge copay |
| Zepbound (any formulation, including KwikPen) for moderate-to-severe OSA | Your Part D plan | Plan’s standard cost-share |
| Foundayo for weight loss | Bridge central processor (Humana) | $50 Bridge copay |
| Ozempic, Mounjaro, or Rybelsus for type 2 diabetes | Your Part D plan | Plan’s standard cost-share |
| Zepbound single-dose vial or pen for any indication | Not Bridge eligible — Part D for OSA only | Plan’s cost-share or cash |
| Compounded semaglutide or tirzepatide | Not Bridge eligible (compounds not allowed) | Outside the Medicare GLP-1 Bridge route |
What if you have both obesity and another condition (OSA or CV disease)?
The answer is whichever indication is on the prescription. CMS is monitoring for plans and prescribers shifting requests between pathways to game the system, so the indication must match what’s clinically appropriate and documented. The Bridge isn’t a discount card you layer on top; it’s a separate program for a specific indication.
Six Mistakes to Avoid Before July 1
These are the mistakes that turn a 30-minute appointment into a three-month delay.
What If Your PA Gets Denied, Sent to the Wrong Place, or You Don’t Qualify?
Sign: The denial comes from your Part D plan and references a “weight loss exclusion” or “not a covered indication.”
What happened: Your prescriber’s office submitted to your Part D plan instead of the Bridge central processor.
What to do: Ask your prescriber’s office to confirm which payer received the request. If it went to the Part D plan for a Bridge-eligible weight-loss indication, they need to resubmit through the Bridge process. The Part D plan’s denial isn’t a clinical denial of your Bridge eligibility.
Sign: The denial mentions missing BMI documentation, missing diagnosis, or unclear records.
What happened: The PA attestation didn’t have enough records behind it for the central processor to confirm the criteria.
What to do: Pull the missing records (old chart visit for BMI at initiation, A1C for prediabetes, eGFR for CKD, etc.) and have the prescriber’s office resubmit. This is the most common, most fixable denial.
Sign: The denial confirms you don’t meet any of the three tiers, even with full records.
What happened: You don’t have a qualifying combination of BMI and condition for the Bridge.
What to do: Two real options:
About Ro as a backup path
If your prescriber’s office isn’t equipped to handle the Bridge — or you don’t qualify and need an FDA-approved cash-pay option — Ro is one of the few telehealth platforms that carries multiple FDA-approved GLP-1 options, including Foundayo, Wegovy pill, Wegovy pen, Zepbound KwikPen, and Ozempic.
Cash-pay or commercial-insurance backup. Not a verified Medicare Bridge submission route. Ro Body: $39 first month, then as low as $74/month with annual plan.
Can a Telehealth Provider Help With the Medicare Bridge PA?
Maybe — but verify before paying. As of April 27, 2026, the consumer telehealth platforms we checked do not publicly confirm Medicare GLP-1 Bridge PA submission to the CMS central processor. Ro’s published pricing FAQ explicitly states Ro currently can’t help coordinate GLP-1 medication coverage for government insurance plans (which includes Medicare). Other major platforms haven’t published Bridge-specific Medicare PA support either.
What to ask any telehealth provider before paying
Commercial insurance vs. Medicare Bridge — they’re not the same animal
| Feature | Commercial insurance PA | Medicare GLP-1 Bridge PA |
|---|---|---|
| Payer | Commercial insurer / PBM | CMS Bridge central processor (Humana / LI NET) |
| Form | Insurer- or PBM-specific | CMS Bridge process (operational details still pending from CMS) |
| Telehealth handles it? | Often, if the platform has insurance concierge | Not yet — Ro publicly says it can’t coordinate government insurance |
| Patient cost if approved | Plan’s copay/coinsurance | $50/month flat |
| Coupons / savings cards | Often yes | No |
| LIS / Extra Help applies | N/A (not Medicare) | No |
What Happens After December 31, 2027?
CMS extended the Medicare GLP-1 Bridge through December 31, 2027 in its April 21, 2026 announcement. CMS originally designed the Bridge as a six-month bridge to the BALANCE Model, which was scheduled to launch in Medicare Part D on January 1, 2027 — but CMS announced that BALANCE will not launch in 2027 as originally planned.
| Period | Status |
|---|---|
| 2026 (July–December) | Bridge active. $50 copay through the central processor. |
| 2027 (January–December) | Bridge active (extended). $50 copay continues through the central processor. |
| 2028 and beyond | Not yet defined. CMS has not published details on what replaces the Bridge after December 31, 2027. |
If you start a Bridge prescription in July 2026, you currently have approximately 18 months of coverage at the $50 copay before the next transition.
The Prescriber and Pharmacy Scripts (Copy-Paste These)
“I’d like to be evaluated for the Medicare GLP-1 Bridge prior authorization for weight management. The Bridge launches July 1, 2026 and CMS extended it through December 31, 2027. I’ve prepared a one-page criteria packet to bring to the visit. Could you confirm the office is set up to submit Bridge PAs to the CMS central processor (Humana, via LI NET infrastructure) rather than to my Part D plan?”
“This prescription should be a Medicare GLP-1 Bridge claim, not a standard Part D claim. The Bridge BIN is 028918, PCN is MEDDGLP1BR, plan group is GLP1Bridge, processor is SS&C Health, routed through RelayHealth, effective July 1, 2026. The help desk is 844-673-0910. The cardholder ID is my Medicare MBI.”
“Was this submitted through the Medicare GLP-1 Bridge or as a regular Part D claim? Could you check the BIN and PCN on the rejection?”
Frequently Asked Questions
1.Is there a Medicare Bridge Program prior authorization form patients can download?
2.Who submits the Medicare GLP-1 Bridge prior authorization?
3.Does the Medicare GLP-1 Bridge PA go to my Part D plan?
4.What is the Medicare GLP-1 Bridge BIN and PCN?
5.What drugs are covered by the Medicare GLP-1 Bridge?
6.Does Ozempic qualify for the Medicare Bridge?
7.Does Mounjaro qualify for the Medicare Bridge?
8.Does Zepbound qualify for the Medicare Bridge?
9.Do compounded GLP-1s qualify for the Bridge?
10.Does my pharmacy have to opt in to the Bridge?
11.Can a telehealth provider submit the Bridge PA?
12.Does the $50 copay count toward my Part D out-of-pocket cap?
13.Can I use a manufacturer coupon with the Bridge?
14.Does Extra Help / LIS reduce the $50?
15.What if I already started Wegovy, Zepbound, or Foundayo before July 2026?
16.What if my doctor sent the PA to my Part D plan by mistake?
17.What if I don’t qualify for the Bridge?
18.Was the Medicare GLP-1 Bridge extended into 2027?
19.When will CMS release the actual Bridge PA submission process for prescribers?
20.Where can my prescriber’s office send technical questions about the Bridge?
What We Verified for This Page
Built from CMS primary sources. Last verified July 10, 2026. Next review: September 11, 2026 or upon CMS guidance update.
What we deliberately did not include because CMS has not released it: the provider-facing operational PA submission process or template; standard PA decision turnaround time; the formal Bridge PA appeals process; the pharmacy dispensing fee amount.
Used as background context only (not for current facts): KFF, AMCP, Reed Smith, Lexology, NCPA — several published before the April 6 drug-list update and the April 21 Bridge extension and may be out of date on those specific points.
Still Not Sure Which GLP-1 Program Is Right for You?
Whether the Medicare GLP-1 Bridge fits depends on your BMI, your conditions, your Part D enrollment, your medication preference, and whether your prescriber is equipped to handle the new PA workflow. If you’re unsure, our 60-second matching tool walks you through the right path based on your situation.
Commercial insurance or cash-pay backup. Not a verified Medicare Bridge submission route.
Related guides
- Foundayo vs Rybelsus: 7 Key Differences, Costs & Who Each Pill Fits (2026)
- Foundayo for PCOS: Eligibility, Cost & Safety (2026)
- Does Insurance Cover Zepbound for Weight Loss?
- Zepbound for Sleep Apnea: Coverage and Eligibility
- How to Switch From Mounjaro to Zepbound: Step-by-Step
- Mounjaro vs Wegovy for PCOS: An Honest Comparison
· By The RX Index Editorial Team · Next scheduled review: May 27, 2026 or upon CMS guidance update, whichever comes first. The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. This guide is for informational purposes only and is not medical advice. Always consult your healthcare provider before starting any medication. Some links on this page are affiliate links — if you purchase through these links, we may earn a commission at no extra cost to you. Affiliate compensation never changes CMS-verified facts. Prices and program details change — verify with CMS and your prescriber before making any decisions. The prescriber CMS technical contact is [email protected].