By The RX Index Research Team · · Next review: May 27, 2026
CMS BALANCE Model GLP-1 Coverage Criteria: Who Qualifies in 2026–2027
🚨 What changed on April 21, 2026
CMS paused the Medicare Part D portion of the BALANCE Model for 2027. It is not launching in Part D next year. To fill the Medicare gap, CMS extended the Medicare GLP-1 Bridge through December 31, 2027. The Medicaid portion of BALANCE is unaffected and still rolling out state by state.
BALANCE Medicaid
✅ Moving forward
State apps due July 31, 2026. Start dates May 1 – Jan 1, 2027.
BALANCE Medicare Part D
⏸️ Paused for 2027
Won't launch in 2027. CMS cited 80% plan threshold not met.
Medicare GLP-1 Bridge
⏳ Filling the gap
Extended through Dec 31, 2027. $50/month. Nationwide.
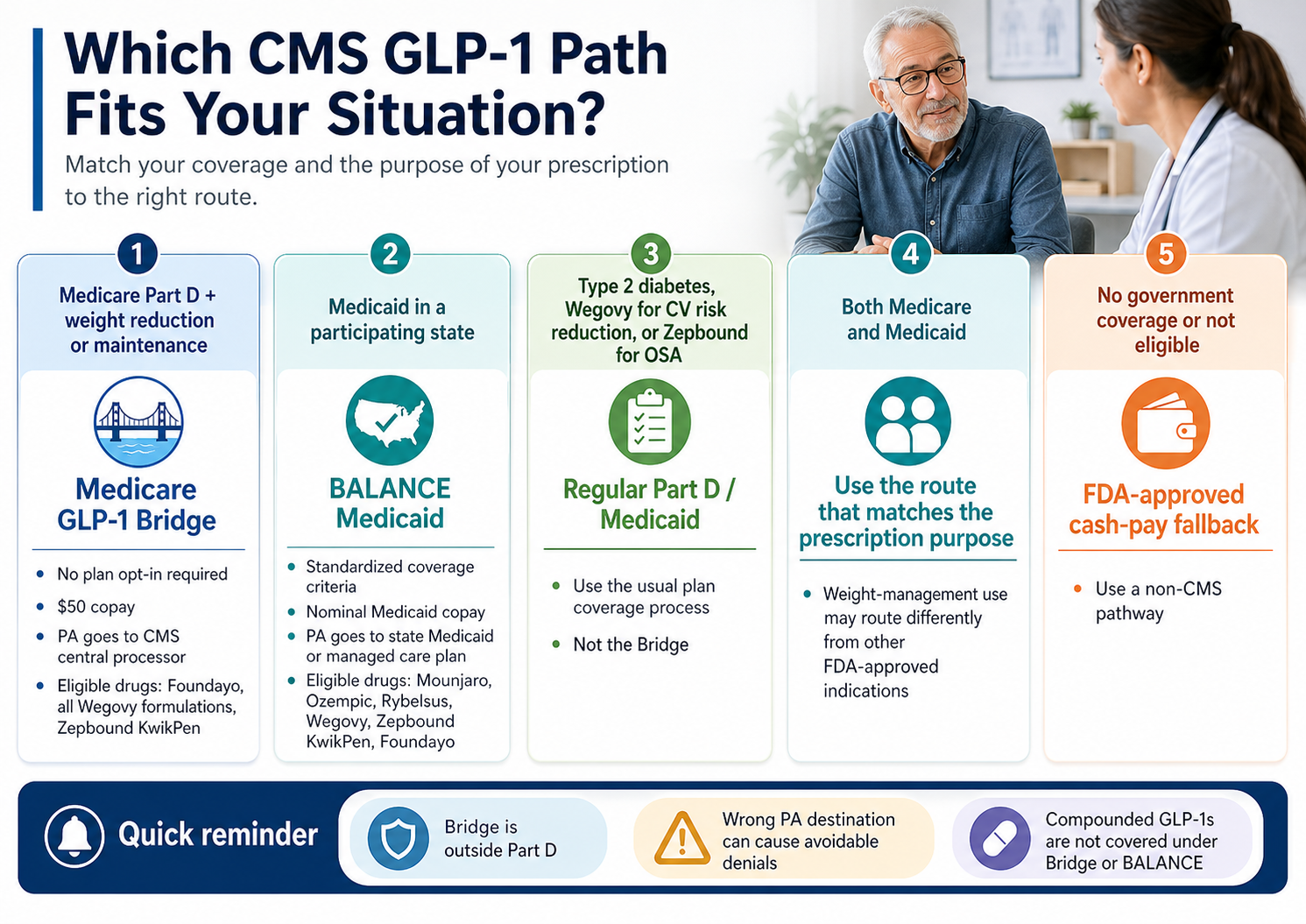
Quick Router: Which CMS GLP-1 Path Are You Actually On?
| If you have… | Start here |
|---|---|
| Medicare Part D + want a GLP-1 for weight management | Medicare GLP-1 Bridge (covered below) |
| Medicaid in a participating state | BALANCE Medicaid (covered below) |
| Type 2 diabetes, CV indication, or sleep apnea + a GLP-1 prescription | Regular Part D / Medicaid for that indication — not Bridge |
| Both Medicare and Medicaid (dually eligible) | Use both pathways, depending on the prescription's purpose |
| Under 65 / no government coverage / you don't qualify | FDA-approved cash-pay fallback (covered below) |
| Honestly, you're not sure | Take the 60-second matching quiz → /find-my-path/ |
Five questions about your coverage, BMI, and diagnoses. Personalized action plan. No signup required.
Jump to what you need:
- What changed April 21, 2026
- The four CMS GLP-1 paths
- Coverage criteria, plain English
- BMI tiers (Tier 1/2/3)
- Bridge vs. BALANCE crosswalk table
- Plan-type eligibility matrix
- Decoded comorbidities
- Which drugs are covered
- What it actually costs
- Where the PA actually goes
- Which states are participating
- What to bring to your doctor
- What if you don't qualify
- If you're already on a GLP-1
- Your next 3 steps
- FAQ (12 questions)
- Sources cited
Not sure which path fits? Take the free 60-second quiz →
What Changed on April 21, 2026 — and What It Means for You
On April 21, 2026, CMS announced it will not implement the Medicare Part D portion of the BALANCE Model in 2027 as originally planned. The Medicaid portion is unaffected. To prevent a Medicare coverage gap, CMS extended the Medicare GLP-1 Bridge through December 31, 2027.
The timeline
CMS announces both BALANCE and the Bridge demonstration
Manufacturer applications due. Eli Lilly and Novo Nordisk both apply
CMS publishes the State Medicaid RFA and the Part D Plans RFA. The 80% Part D participation threshold is laid out in Section 2.3.1
Part D plan sponsor applications due
CMS sends an HPMS memo to plan sponsors announcing the Part D pause and the Bridge extension. One day after the deadline
CMS BALANCE Model webpage updated to reflect the new Bridge end date
KFF publishes a Quick Take confirming the extension and pause
Why the pause happened
CMS required Part D plan sponsors covering at least 80% of all Part D beneficiaries to apply. UnitedHealthcare publicly said it was “still working through” whether to participate. Bloomberg reporting indicated CVS Health (Aetna) declined. Without those two, the math didn’t work, and CMS pulled the plug rather than launch with thin participation. The CMS memo phrased the delay as “pending further evaluation and data collection,” not “canceled.” The next signal to watch is the CY2028 Advance Notice, typically released January or February 2027.
What the pause means by situation
On Medicare Part D, planning to use BALANCE for weight management in 2027
Nothing breaks. The Bridge runs an extra year. Use it July 1, 2026 through December 31, 2027 at $50/month, no plan opt-in required.
On Medicaid
Nothing changes from the original plan. Your state still has until July 31, 2026 to apply, and can pick a start date between May 1, 2026 and January 1, 2027.
Dually eligible (Medicare + Medicaid)
Two pathways remain available. The Bridge handles your Medicare-side weight-management prescription. Your state Medicaid program handles the Medicaid side, where applicable.
Shopping plans for 2027 open enrollment
Don't make BALANCE participation a deciding factor. There's nothing to choose between for 2027. Pick the plan that best fits your overall medication needs and watch the CY2028 Advance Notice in early 2027.
The Four CMS GLP-1 Coverage Paths
There are four CMS-related pathways for GLP-1 coverage in 2026–2027. Identifying your pathway before reading the criteria is the single most important step — applying the right rule to the wrong program is the most common reason readers get confused or denied.
- •Nationwide — all 50 states, DC, and US territories
- •Operates outside Part D. Your Part D plan doesn't process the claim
- •No plan opt-in required — eligible plan type is all you need
- •$50 copay at the pharmacy
- •July 1, 2026 through December 31, 2027
- •Eligible drugs: Foundayo, all Wegovy formulations, Zepbound KwikPen only
- •Prescription must be for weight reduction or maintenance
- •Voluntary for states — your state Medicaid agency must opt in
- •State applications due July 31, 2026; start dates May 1, 2026–January 1, 2027
- •Coverage criteria standardized across participating states (Section 2.7.3 State Medicaid RFA)
- •Same criteria apply to fee-for-service and Medicaid managed care
- •Standard nominal Medicaid copays ($0–$8, state-specific)
- •Eligible drugs: all formulations of Mounjaro, Ozempic, Rybelsus, Wegovy; plus Zepbound KwikPen and Foundayo
- •Medicaid Key Terms effective through December 31, 2027 (subject to renegotiation)
- •Wegovy for cardiovascular risk reduction in established CV disease → regular Part D
- •Zepbound for moderate-to-severe OSA in adults with obesity → regular Part D
- •Any GLP-1 for type 2 diabetes → regular Part D or Medicaid
- •Bridge and BALANCE are specifically for the weight-management use
- •CMS actively monitors against shifting covered Part D prescriptions onto the Bridge
- •Originally scheduled for January 1, 2027 launch
- •CMS announced the pause April 21, 2026 via HPMS memo
- •Nothing to enroll in for 2027
- •Next signal: CY2028 Advance Notice, typically released January or February 2027
- •The criteria, drug list, and cost structure from the March 2026 RFA are documented below as reference
CMS BALANCE Model GLP-1 Coverage Criteria, in Plain English
The BALANCE Model coverage criteria require provider attestation that the patient meets one of four routes: (a) type 2 diabetes, (b) noncirrhotic MASH with F2–F3 fibrosis, (c) obstructive sleep apnea, or (d) ongoing lifestyle modification combined with one of three BMI-based clinical tiers. The BMI used for qualification is the BMI at the time of GLP-1 therapy initiation — not your current BMI if you’ve already started losing weight.
The four “gates” you have to pass
You're in a participating pathway.
Medicaid: your state has opted into BALANCE. Bridge: you have Medicare Part D in an eligible plan type.
The drug is on the eligible list.
No compounded GLP-1s. Specific FDA-approved formulations only.
You fit one of the clinical routes
(the ones below)
Your provider attests
to your route, including the lifestyle modification component where required
The Three BMI-Based Clinical Tiers
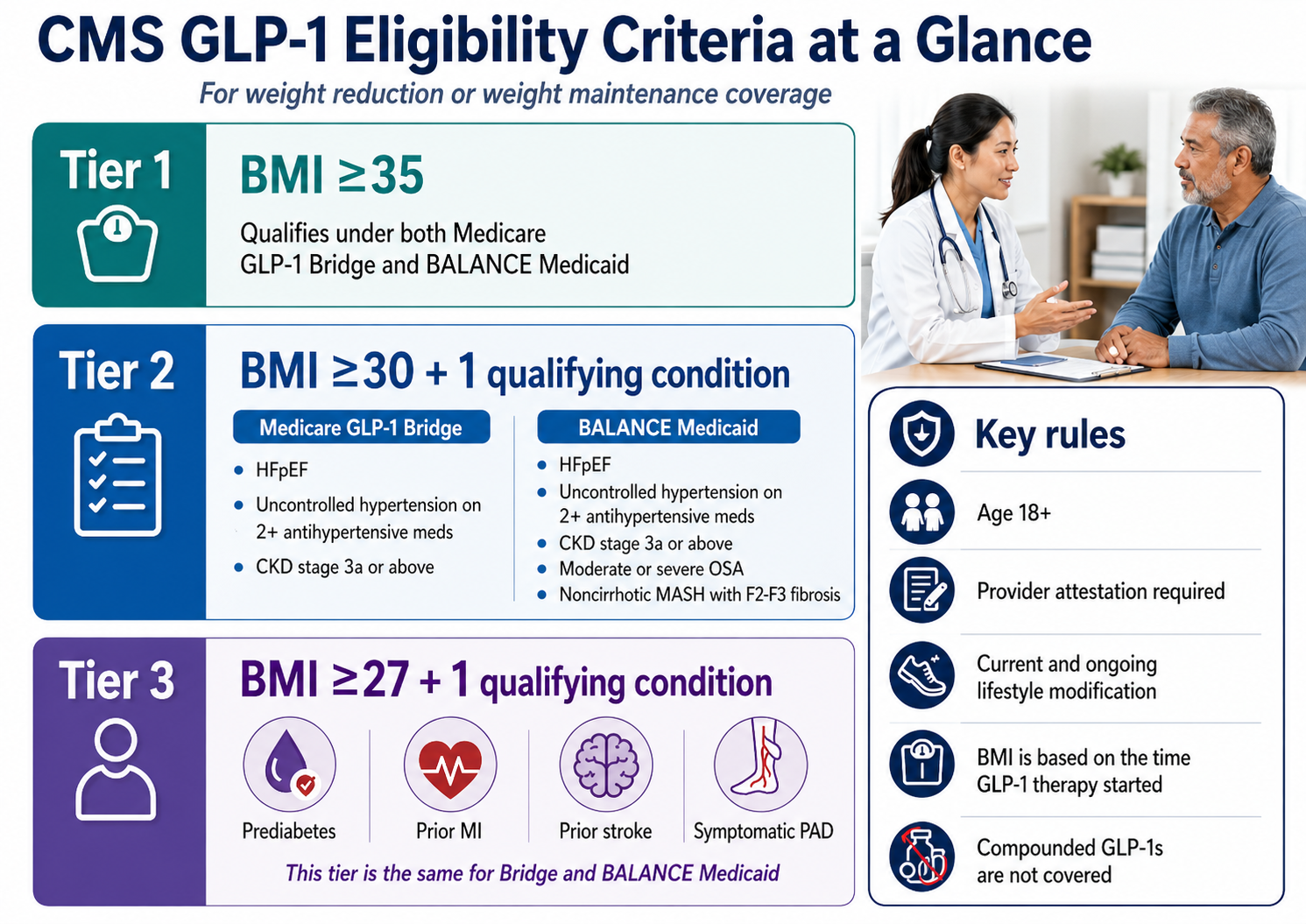
Source: CMS State Medicaid RFA Section 2.7.3 and CMS Medicare GLP-1 Bridge FAQ. Verified April 27, 2026.
The simplest tier. If your BMI was 35 or higher at the time you started (or are about to start) GLP-1 therapy, you qualify on BMI alone. You must be at least 18, and you must be on lifestyle modification (structured nutrition + physical activity per the FDA-approved label).
⏰ BMI at initiation — not your current BMI
If you started Wegovy in September 2024 at BMI 37 and you’re now at BMI 34, your prescriber attests to the BMI ≥35 criterion based on your starting BMI. CMS gave this exact example in the Bridge FAQ. Dig out old chart records before the appointment.
Applies to: Medicare GLP-1 Bridge and BALANCE Medicaid (identical criteria).
This is where BALANCE Medicaid and the Medicare Bridge criteria diverge.
Medicare GLP-1 Bridge (3 conditions)
- ✔Heart failure with preserved ejection fraction (HFpEF)
- ✔Uncontrolled hypertension (SBP >140 OR DBP >90) on 2+ antihypertensive meds
- ✔Chronic kidney disease, stage 3a or above
BALANCE Medicaid (5 conditions)
- ✔HFpEF
- ✔Uncontrolled hypertension on 2+ antihypertensives
- ✔CKD stage 3a or above
- ✔Moderate or severe OSA (AHI >15, no central or mixed sleep apnea)
- ✔Noncirrhotic MASH with F2–F3 liver fibrosis
OSA and MASH are additions not in the Bridge.
Why the Bridge excludes OSA and MASH: Zepbound and Wegovy each have separate FDA-approved indications for those conditions. CMS expects those prescriptions to flow through regular Part D.
Prediabetes
A1C 5.7–6.4%, fasting glucose 100–125 mg/dL, or 2-hr OGTT 140–199 mg/dL (ADA guidelines)
Prior MI
Prior myocardial infarction documented in your medical history
Prior Stroke
Documented ischemic or hemorrhagic stroke with imaging
Symptomatic PAD
Peripheral artery disease with claudication, typically ABI <0.90
BMI 27 with prediabetes is a common combination — far more common than BMI 35 — and both BALANCE and the Bridge accept it. That’s a wider door than most commercial insurance currently uses.
BALANCE Medicaid also covers three additional clinical routes
Per Section 2.7.3 of the State Medicaid RFA, BALANCE also covers GLP-1s when the provider attests the patient: (a) has type 2 diabetes, OR (b) has noncirrhotic MASH with F2–F3 fibrosis, OR (c) has obstructive sleep apnea. These routes exist independently of the BMI tiers — if you have T2D under BALANCE Medicaid, you don’t need a BMI threshold. The Medicare Bridge does not use these additional routes; it’s BMI-tier-only for weight reduction.
The lifestyle modification attestation
CMS doesn’t require you to have completed a specific weight-loss program first. It requires you’re on, or will continue, lifestyle modification appropriate to the FDA-approved label — structured nutrition and physical activity. Your provider attests to this as part of the prior authorization. For BALANCE Medicaid specifically: participating manufacturers are required to fund a lifestyle support program available to all beneficiaries on a model drug for weight management, at no cost to you.
Bridge vs. BALANCE: The Criteria Crosswalk
The Medicare GLP-1 Bridge and the BALANCE Model use similar but not identical clinical criteria, different drug lists, different cost-sharing rules, and completely different prior authorization workflows. This is the table to bookmark. We update it monthly.
| Criterion | Medicare GLP-1 Bridge (begins July 2026) | BALANCE Medicaid (rolling May 2026) | BALANCE Medicare Part D (PAUSED for 2027) |
|---|---|---|---|
| Status as of 4/27/2026 | SCHEDULED to begin July 1, 2026; extended through 12/31/2027 | LAUNCHING — state apps due 7/31/2026 | DELAYED — will not launch in 2027 |
| Authority | Section 402 demonstration; sits outside Part D | Section 1115A model; supplemental rebates with each state | Section 1115A model; was to be inside Part D benefit |
| Plan or state must opt in? | NO — every eligible Part D beneficiary in an eligible plan type can use it | YES — only beneficiaries in participating states qualify | YES — was to require plan opt-in; 80% threshold not cleared |
| Age requirement | ≥18 | ≥18 | ≥18 |
| BMI Tier 1 (≥35 alone + lifestyle modification) | Qualifies | Qualifies | Was to qualify |
| BMI Tier 2 conditions (≥30 + one of:) | HFpEF, uncontrolled HTN (>140 systolic OR >90 diastolic on 2+ meds), CKD stage 3a+ | Same three PLUS moderate/severe OSA (AHI >15 without central or mixed sleep apnea), noncirrhotic MASH F2–F3 | Same as BALANCE Medicaid |
| BMI Tier 3 conditions (≥27 + one of:) | Prediabetes (per ADA), prior MI, prior stroke, symptomatic PAD | Same | Same |
| Lifestyle modification required? | YES (per FDA label) | YES (per FDA label) | YES |
| Eligible drugs | Foundayo, Wegovy (injection + tablets), Zepbound KwikPen | All formulations of Mounjaro, Ozempic, Rybelsus, Wegovy + Zepbound KwikPen + Foundayo | Same list as BALANCE Medicaid |
| Beneficiary cost | $50/month copay | Standard nominal Medicaid copay ($0–$8) | Was: $50 (Enhanced Alternative + EGWP); $125 (Actuarially Equivalent + Basic Alternative) |
| Where the PA goes | CMS central processor (NOT your Part D plan) | State Medicaid agency or managed care plan | Was: participating Part D plan |
| Pharmacy claim routing | BIN 028918 / PCN MEDDGLP1BR / SS&C Health / RelayHealth | Standard state Medicaid pharmacy claim | Was: standard Part D pharmacy claim |
| LIS subsidies apply? | NO — LIS does NOT reduce the $50 Bridge copay | N/A (Medicaid copays already nominal) | Was to follow standard Part D LIS rules |
| Counts toward Part D OOP cap? | NO — Bridge sits outside Part D | N/A | Was to count toward Part D OOP cap |
| Coupons / manufacturer copay cards? | NO — not allowed on Bridge claims | State-specific | Was to follow standard Part D rules |
| Lifestyle support program | Not required | REQUIRED — manufacturer-funded, free to beneficiaries | Was to be required |
| Performance period | 7/1/2026 – 12/31/2027 | Key Terms effective through 12/31/2027; full agreement through 12/31/2031 (subject to change) | Was: 1/1/2027 – 12/31/2031 |
Most important rows for most readers: “Plan or state must opt in?”, “Where the PA goes”, and “Beneficiary cost.” Get those three right and the rest tends to follow. Updated monthly.
Plan-Type Matrix: Which Plans Qualify for Which Path
Eligibility for the Medicare GLP-1 Bridge depends on the type of Part D plan you’re enrolled in. Standalone PDPs and most MA-PD plans are eligible. Private fee-for-service plans, PACE organizations, and several other plan types are not eligible for the Bridge unless you’re also enrolled in a standalone PDP. Many people miss this layer entirely.
| Plan you’re enrolled in | Bridge eligible? | BALANCE Medicaid eligible? |
|---|---|---|
| Standalone Part D PDP | YES | N/A |
| MA-PD (HMO, HMOPOS, Local PPO, Regional PPO) | YES | N/A |
| Special Needs Plan (SNP) | YES (also if enrolled in standalone PDP) | N/A |
| Employer/union group waiver plan (EGWP) | YES | N/A |
| LI NET (Limited Income Newly Eligible Transition) | YES | N/A |
| Defined Standard Part D plan | YES (Bridge) | N/A |
| Private fee-for-service (PFFS) plan | NO — unless also in standalone PDP | N/A |
| Section 1876 cost contract / Section 1833 prepayment | NO — unless also in standalone PDP | N/A |
| PACE organization | NO — unless also in standalone PDP | N/A |
| Religious fraternal benefit plan | NO — unless also in standalone PDP | N/A |
| Fallback plan | NO | N/A |
| Medicaid fee-for-service | N/A unless dually eligible | YES if your state participates |
| Medicaid managed care | N/A unless dually eligible | YES if your state participates (uniform criteria FFS and MCO) |
| Dually eligible (Medicare + Medicaid) | YES if in eligible Part D plan + meet criteria | YES if state participates |
Not sure what type of plan you have? Look at your Annual Notice of Change letter — it states the plan type clearly. Or log in at Medicare.gov.
Decoded Comorbidities: What Each Criterion Means in Your Medical Chart
Your prior authorization succeeds or fails based on whether your medical record contains the specific values, diagnoses, and tests that prove each condition. This table translates each criterion into what your chart needs to actually say and what to ask your doctor about.
| Criterion as written by CMS | What this looks like in your medical chart | What to ask your doctor |
|---|---|---|
| HFpEF (heart failure with preserved ejection fraction) — per AHA/ACC: EF ≥50% with documented HF symptoms | Echocardiogram showing left ventricular ejection fraction ≥50%, with documented heart failure diagnosis | “Have I had an echocardiogram? What was my ejection fraction?” |
| Uncontrolled hypertension | Blood pressure readings consistently above 140 systolic OR 90 diastolic, recorded while on two or more antihypertensive medications | “What are my recent BP readings? What antihypertensive meds am I currently on?” |
| CKD stage 3a or above — KDIGO: stage 3a = eGFR 45–59; 3b = 30–44; 4 = 15–29; 5 = <15, sustained ≥23 months | eGFR <60 confirmed on at least 2 readings 3+ months apart | “What was my last eGFR? Has my kidney function been documented below 60?” |
| Moderate or severe OSA (BALANCE Medicaid only) — AHI >15 without central or mixed sleep apnea | Sleep study with apnea-hypopnea index >15 events per hour | “Have I had a sleep study? What was my AHI?” |
| Noncirrhotic MASH with F2–F3 fibrosis (BALANCE Medicaid only) | Liver biopsy or non-invasive marker (FibroScan, MRE/MRI, ELF, Fibrosure, Fib-4) showing F2 or F3 fibrosis | “Has my liver fibrosis been staged? Do I have a recent FibroScan?” |
| Prediabetes per ADA guidelines — A1C 5.7–6.4%, fasting glucose 100–125 mg/dL, or 2-hour OGTT 140–199 mg/dL | Lab values matching ADA thresholds | “What was my last A1C? Fasting glucose?” |
| Prior MI (heart attack) | Documented MI in your history with troponin elevation, ECG changes, or imaging confirming the event | “Do I have hospital records or a cardiology note documenting a prior heart attack?” |
| Prior stroke | Documented ischemic or hemorrhagic stroke with imaging | “Hospital records or neurology note documenting a prior stroke?” |
| Symptomatic PAD | Diagnosed peripheral artery disease with symptoms — typically claudication confirmed by ABI <0.90 | “Have I had an ankle-brachial index test? Do I experience leg pain when walking?” |
| BMI ≥35 / ≥30 / ≥27 | Calculated as weight in kg ÷ (height in m)². Criteria use BMI at GLP-1 therapy initiation, even if you've since lost weight | “What was my BMI when I started therapy? Can we document that for prior auth?” |
Clinical definitions sourced from American Diabetes Association (prediabetes), KDIGO (CKD staging), AHA/ACC (HFpEF), and AASM (OSA severity by AHI). Always defer to your prescriber’s clinical judgment on diagnosis and documentation.
Which GLP-1 Drugs Are Covered
The Medicare GLP-1 Bridge currently covers Foundayo, all formulations of Wegovy, and the Zepbound KwikPen formulation only. The BALANCE Model covers a broader list: all formulations of Mounjaro, Ozempic, Rybelsus, Wegovy, plus Zepbound KwikPen and Foundayo. Compounded GLP-1s are not covered under either program.
Medicare GLP-1 Bridge — covered drugs
| Drug | Status |
|---|---|
| Foundayo (orforglipron) | ✅ Included — all formulations |
| Wegovy (semaglutide) | ✅ Included — injection + tablets |
| Zepbound KwikPen | ✅ Included — KwikPen only |
| Zepbound single-dose vial | ❌ Excluded |
| Zepbound single-dose pen | ❌ Excluded |
| Ozempic | ❌ Not Bridge-covered |
| Mounjaro | ❌ Not Bridge-covered |
| Rybelsus | ❌ Not Bridge-covered |
| Compounded GLP-1s | ❌ NOT included |
Drug list updated April 6, 2026 (Foundayo addition; Zepbound KwikPen-only clarification).
BALANCE Model — covered drugs
Broader list because BALANCE covers GLP-1s for both weight management and currently-covered Part D/Medicaid indications.
To qualify as a “model drug,” a product must reduce body weight by at least 9.5% on average in an RCT primary or secondary endpoint (at an FDA-approved dose).
Compounded GLP-1s are not the answer on this page
The Bridge payer sheet explicitly states that compounded products are not allowed on Bridge claims. BALANCE is built on FDA-approved manufacturer participation. Separately, the FDA has issued formal warnings about unapproved GLP-1 drugs sold for weight loss, noting that compounded GLP-1 drugs have not been reviewed by the FDA for safety, effectiveness, or quality. If you’re trying to use the CMS BALANCE Model or the Medicare GLP-1 Bridge for coverage, compounded medications are not part of the answer.
What It Actually Costs
Medicare GLP-1 Bridge: $50/month copay, no subsidies, doesn’t count toward Part D OOP cap. BALANCE Medicaid: standard nominal Medicaid copay ($0–$8). BALANCE Part D, if it ever launches, was structured at $50/month (Enhanced Alternative) or $125/month (Actuarially Equivalent and Basic Alternative).
The $50 does not count toward your Part D out-of-pocket cap.
The Bridge sits outside Part D entirely. Whatever you spend on the Bridge has no effect on your TrOOP total. If you were planning to hit your Part D cap, the Bridge doesn't help you get there.
Low-Income Subsidy (LIS / Extra Help) does not reduce the $50.
KFF specifically flagged this concern in their April 2026 brief. If you're an LIS beneficiary and $50 is genuinely unaffordable, the Bridge may be out of reach despite you meeting the clinical criteria.
Manufacturer coupons and copay cards don't apply to Bridge claims.
The Bridge is its own payment mechanism. The $50 is the $50.
How the Bridge $50 compares to cash-pay (April 27, 2026)
| Channel / Program | Drug | Price as of 4/27/2026 |
|---|---|---|
| Bridge ($50 copay) | Foundayo, Wegovy, Zepbound KwikPen | $50/month (if you qualify) |
| Wegovy list price | Wegovy injection | ~$1,350/month |
| Zepbound list price | Zepbound | ~$1,086/month |
| NovoCare (manufacturer direct) | Wegovy pill, lower dose | $149/month |
| NovoCare (manufacturer direct) | Wegovy pill, higher dose | $299/month |
| NovoCare (manufacturer direct) | Wegovy pen | $199/$349/$399 depending on dose and offer |
| LillyDirect (manufacturer direct) | Zepbound KwikPen | Starting at $299/month |
| Ro Body cash-pay | Wegovy pill, Foundayo, Wegovy pen, Zepbound KwikPen | Membership $39 first month / as low as $74/month annual prepay (medication separate, matched to manufacturer pricing) |
Prices change frequently — re-verify before acting on them. Even at $50 with no TrOOP help and no subsidies, the Bridge is the cheapest legitimate FDA-approved branded path for Medicare beneficiaries who qualify.
BALANCE Part D cost structure (for reference if it revives for 2028)
| Part D plan type | Deductible phase | Initial coverage phase | Catastrophic phase |
|---|---|---|---|
| Enhanced Alternative + EGWP | Up to $245 + dispensing fee per 30-day supply | Up to $50/month | $0 (after the 2027 OOP cap of $2,400) |
| Actuarially Equivalent + Basic Alternative | Up to $245 + dispensing fee per 30-day supply | Up to $125/month | $0 (after the 2027 OOP cap of $2,400) |
| Defined Standard | NOT eligible to participate as DS | — | — |
This structure is not operative for 2027. Documented from CMS Part D Plans RFA for reference in case BALANCE Part D revives for 2028.
Where the Prior Authorization Actually Goes
For the Medicare GLP-1 Bridge, the prescriber sends the prior authorization request to a CMS central processor — not to your Part D plan. Sending it to the Part D plan is one of the most avoidable causes of confusing denials.
Step 1 — Prescriber prior authorization
Your prescribing provider submits a Bridge-specific prior authorization request to the CMS central processor, not to your Part D plan. This is the clinical attestation step where the prescriber confirms you meet one of the Bridge clinical routes. CMS continues to publish operational guidance on the prescriber-side process throughout Spring 2026.
Step 2 — Pharmacy claim routing (NCPDP billing)
When you fill the prescription, the pharmacy submits the claim using:
| BIN | 028918 |
| PCN | MEDDGLP1BR |
| Processor | SS&C Health |
| Routed through | RelayHealth |
| Pharmacy help desk | 844-673-0910 |
| Effective date | July 1, 2026 |
| Compounds allowed? | NO |
The wrong-destination problem
A prescriber submits a Bridge-eligible prescription’s prior authorization to your Part D plan instead of the central processor. The Part D plan denies it. The patient assumes they don’t qualify clinically. That’s not what happened — the PA went to the wrong destination. When talking to your prescriber, specifically ask whether the prior authorization is being submitted to the CMS central processor for the Medicare GLP-1 Bridge or to your Part D plan.
BALANCE Medicaid prior authorization
For Medicaid BALANCE, the prior authorization goes through your state Medicaid program — fee-for-service or your Medicaid managed care plan. The State Medicaid RFA requires participating states to apply the same standardized access policy to both FFS and managed care, so the criteria should be the same in both contexts.
Auto-Lookback (BALANCE Part D, if it revives)
The BALANCE Part D RFA included an automated record review process called Auto-Lookback. If your medical history already shows the qualifying diagnosis (T2D, prior MI, etc.), the plan can auto-approve without a separate attestation. If Auto-Lookback fails, the plan must accept appropriate healthcare professional attestation. This was structured into the paused model and will be relevant again if BALANCE Part D revives.
The quiz output includes a printable note naming the Bridge, the PA destination, the relevant criteria for your situation, and the pharmacy claim routing. Bring it to your appointment.
BALANCE Medicaid: Which States Are Participating
As of April 27, 2026, BALANCE Medicaid is in active rollout. State Medicaid agencies have until July 31, 2026 to apply. CMS has not yet published a consolidated list of participating states. The state-by-state picture is changing fast.
The state landscape changed several times in the past year, even outside BALANCE:
| State | Pre-BALANCE Medicaid FFS coverage (Jan 2026) | BALANCE status | Source |
|---|---|---|---|
| All 50 states + DC + territories in MDRP | Per KFF: 13 states covered; specific names verified monthly via state Medicaid PDLs | Pending consolidated CMS list | Updated monthly |
| California | Eliminated obesity coverage 2025–2026 | Decision pending | State DHCS |
| New Hampshire | Eliminated obesity coverage 2025–2026 | Decision pending | State Medicaid |
| Pennsylvania | Eliminated obesity coverage 2025–2026 | Decision pending | State Medicaid |
| South Carolina | Eliminated obesity coverage 2025–2026 | Decision pending | State Medicaid |
| North Carolina | Reinstated obesity coverage Dec 2025 | Decision pending | State Medicaid |
State participation tracker: updated monthly through 2027. State application deadline: July 31, 2026. CMS retains discretion to allow late-joining states.
Check current obesity GLP-1 coverage (outside BALANCE)
Look up your state Medicaid PDL on your state Medicaid agency website. Search for “semaglutide” or “tirzepatide” and check the prior authorization criteria.
Check BALANCE participation
Look for any state Medicaid agency announcement of a BALANCE State Agreement, a State Plan Amendment (SPA) related to GLP-1 supplemental rebate agreements, or a public statement from the state Medicaid director.
What to Bring to Your Doctor’s Appointment
The strongest BALANCE or Bridge prior authorization is one where the medical record clearly documents your BMI at therapy initiation, your qualifying diagnosis or comorbidity, your current lifestyle modification, and (for the Bridge) confirmation that the prescription is for weight reduction or maintenance. Walk in with the right documents so your prescriber can submit the cleanest request the first time.
Universal documents (everyone brings these)
Route-specific documentation
| Your route | Records that help your prior auth |
|---|---|
| BMI ≥35 alone | Height/weight record at initiation; growth chart if BMI fluctuates |
| BMI ≥30 + HFpEF | Cardiology note + most recent echo report with EF value |
| BMI ≥30 + uncontrolled HTN | BP log (home or office), current antihypertensive medication list showing 2+ meds |
| BMI ≥30 + CKD 3a+ | Recent eGFR labs (within 12 months ideally), nephrology or PCP note |
| BMI ≥30 + moderate/severe OSA (BALANCE Medicaid only) | Sleep study report with AHI |
| BMI ≥30 + MASH F2–F3 (BALANCE Medicaid only) | FibroScan, MRE, ELF, Fibrosure, or Fib-4 result; hepatology note |
| BMI ≥27 + prediabetes | A1C 5.7–6.4% or fasting glucose 100–125 mg/dL |
| BMI ≥27 + prior MI/stroke | Hospital discharge summary, cardiology or neurology note |
| BMI ≥27 + symptomatic PAD | Ankle-brachial index test result, vascular medicine note |
Doctor script you can use verbatim
“I’m trying to figure out whether my prescription should go through the Medicare GLP-1 Bridge, regular Part D, BALANCE Medicaid, or somewhere else. The Bridge is a CMS demonstration that begins July 1, 2026 and runs through 2027, and the prescriber submits the prior authorization to a CMS central processor — not to my Part D plan. I think I qualify on [your route], and I have [the relevant documentation]. Can your office handle the routing, or do you need information from me to get this to the right place?”
What If You Don’t Qualify or Your State Isn’t in BALANCE
Not qualifying for one CMS pathway doesn’t mean you have no GLP-1 path. It means you’re using the wrong program for your situation.
If you have type 2 diabetes (Ozempic, Mounjaro, Rybelsus), an FDA-approved cardiovascular risk reduction indication for Wegovy, or moderate-to-severe OSA in adults with obesity (Zepbound), your prescription should go through regular Part D or your state Medicaid program. For most people in this situation, that's the fastest path.
If your state didn't cover GLP-1s for obesity before BALANCE and isn't joining BALANCE, your Medicaid coverage for weight-management GLP-1s is unlikely. If you're in one of the 13 states that covered them under fee-for-service as of January 2026, you may already have a path — check your state Medicaid PDL directly.
Usually the cheapest cash-pay path for FDA-approved branded GLP-1s. LillyDirect: Zepbound KwikPen starting at $299/month. NovoCare: Wegovy pill from $149 (lower dose) / $299 (higher dose); Wegovy pen $199/$349/$399 depending on dose. We do not earn a commission on these routes. We're showing them because for cost-only optimization, they're often the right answer.
Who Ro fits well for
- ✔Under 65 / not on Medicare or Medicaid
- ✔FEHB (Federal Employees Health Benefits) + want help navigating coverage
- ✔Commercial insurance + want a free coverage check
- ✔Don't qualify for Bridge or BALANCE, want FDA-approved branded options
Honest limitations
- ⚠Ro is not the cheapest path. Membership $39 first month, then as low as $74/month annual / $149 month-to-month. Medication is on top.
- ⚠Ro's insurance concierge can't coordinate GLP-1 coverage for government insurance (Medicare, Medicaid, TRICARE) — exception for FEHB.
- ⚠Refills require a 45-day check-in window. Missing it can move you to higher pricing tiers.
Get started for $39, then as low as $74/month with annual plan. Medication billed separately.
Disclosure: The RX Index may earn a commission if you use this Ro link. Affiliate compensation never changes CMS-verified facts.
If your situation is unusual or doesn't fit cleanly into any of the above, the quiz is built to handle edge cases. Five questions, sixty seconds, personalized output.
If You’re Already on a GLP-1, What Changes
You're on Ozempic for type 2 diabetes through your Part D plan.
Nothing changes. The Bridge doesn't include Ozempic. Your existing Part D coverage for diabetes continues exactly as it has been.
You're on Wegovy for cardiovascular risk reduction.
Your Part D coverage continues, and CMS expects your prescription to flow through your Part D plan, not the Bridge.
You're paying cash-pay for Wegovy or Zepbound for weight loss, and you have Medicare Part D.
This is where the Bridge may genuinely change things. Once the Bridge begins July 1, 2026, if you meet the clinical criteria and you're in an eligible Part D plan type, your provider can submit a Bridge prior authorization. If approved, your monthly cost drops from cash-pay pricing to $50.
You're on a compounded GLP-1 for weight loss.
The Bridge doesn't include compounded GLP-1s. To use the Bridge, your prescriber would need to switch you to one of the included FDA-approved branded options (Foundayo, Wegovy injection, Wegovy tablets, or Zepbound KwikPen) and submit a Bridge PA. That's a clinical decision you and your prescriber make together.
You're on a GLP-1 through your state Medicaid program already.
If your state joins BALANCE Medicaid, your access pathway may change. Confirm your state Medicaid PDL, managed-care rollout, and PA process before assuming continuity.
Your Next 3 Steps
Step 1: Identify your pathway.
Medicare Part D + weight management → Bridge. Medicaid + participating state → BALANCE Medicaid. Non-obesity FDA-approved indication → regular Part D or Medicaid. None of the above → cash-pay alternative or quiz.
Step 2: Gather your documentation.
Use the route-specific table above. Pull from your patient portal if possible — the more your prescriber can see in your existing chart, the faster the prior auth goes.
Step 3: Schedule with your prescribing provider.
Bring the documentation and the doctor script. Confirm the prior authorization is being routed to the right destination (central processor for the Bridge, your state Medicaid for BALANCE Medicaid, your Part D plan for non-obesity indications).
Frequently Asked Questions about CMS BALANCE Model GLP-1 Coverage Criteria
1.Is the BALANCE Model still happening?
2.Why was BALANCE Medicare Part D paused?
3.Does BMI 30 alone qualify under CMS BALANCE GLP-1 criteria?
4.What's the difference between the BALANCE Model and the Medicare GLP-1 Bridge?
5.Which GLP-1 drugs are included in the Medicare GLP-1 Bridge?
6.Do compounded GLP-1s qualify for the Bridge or BALANCE?
7.Does the $50 Bridge copay count toward my Part D out-of-pocket cap?
8.Does Extra Help (LIS) reduce the $50 Bridge copay?
9.Where does the Medicare GLP-1 Bridge prior authorization go?
10.Will my Medicaid plan cover GLP-1s under BALANCE?
11.Does prediabetes qualify?
12.Does sleep apnea qualify?
Still Not Sure Which GLP-1 Program Is Right for You?
The CMS programs are real, the criteria are clear, and the next step is yours. If you want a personalized action plan that takes into account your Medicare or Medicaid situation, your BMI tier, your state, your current GLP-1 use (if any), and what to watch for in 2026 open enrollment — answer five questions and we’ll build it for you.
No signup required. No medical claims. No upsell. Just the answer.
Sources Cited on This Page
We pull directly from primary CMS documents. Last verified April 27, 2026. Next re-verification: May 27, 2026.
- ✓CMS Medicare GLP-1 Bridge program page and FAQ (last updated April 6, 2026 to add Foundayo)
- ✓CMS BALANCE Model program page (verified April 27, 2026)
- ✓CMS BALANCE Model State Medicaid Request for Applications (PDF, March 2026 — Section 2.7.3 coverage criteria; Section 2.4.2 standardized access policy)
- ✓CMS BALANCE Model Part D Plans Request for Applications (PDF, March 2026 — Section 2.2.5 clinical criteria; Section 2.3.1 the 80% participation threshold)
- ✓CMS GLP-1 Bridge payer sheet (NCPDP claim billing fields for pharmacy)
- ✓KFF: “What to Know About the BALANCE Model for GLP-1s in Medicare and Medicaid” (March 24, 2026, with April 21 editorial note)
- ✓KFF Quick Take on Bridge extension and BALANCE Part D pause (April 23, 2026)
- ✓KFF: “Medicaid Coverage of and Spending on GLP-1s” (January 2026)
- ✓FDA postmarket safety information on unapproved GLP-1 drugs sold for weight loss
- ✓Ro Body pricing page (verified April 27, 2026)
- ✓Cross-referenced against AHA News, TechTarget, Becker's Hospital Review, Avalere Health, Advisory Board, and Reed Smith April 2026 coverage of the Part D pause
- ✓Clinical definitions: American Diabetes Association (prediabetes), KDIGO (CKD staging), AHA/ACC (HFpEF), AASM (OSA severity by AHI)
Used as background context only (not for primary current-fact verification): KFF, AMCP, Reed Smith, Becker’s, Avalere — several published before the April 21 Bridge extension and may be out of date on those specific points.
Related guides on The RX Index
- Medicare Bridge Program Prior Authorization Form: What to Use, Who Submits It (2026)
- Foundayo vs Rybelsus: 7 Key Differences, Costs & Who Each Pill Fits (2026)
- Foundayo for PCOS: Eligibility, Cost & Safety (2026)
- Does Medicare Cover Zepbound for Weight Loss?
- Does Medicare Cover Wegovy for Weight Loss?
- Mounjaro vs Wegovy for PCOS: An Honest Comparison
· Next scheduled re-verification: May 27, 2026 · By The RX Index Research Team · The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. This guide is for informational purposes only and is not medical advice or a guarantee of eligibility. Confirm specifics with your prescriber, your plan, and your state Medicaid agency. The RX Index may earn a commission when readers use the Ro link in this article. This does not influence the eligibility criteria, plan-type matrix, drug list, state participation framework, or alternative-paths guidance — those are built directly from CMS source material and are unaffected by any commercial relationship.