GLP-1 Formulary Exception: How to Get Wegovy, Zepbound, or Ozempic Covered When Your Plan Says No
Published:
Written by The RX Index Editorial Team
A GLP-1 formulary exception is the formal request that asks your insurance plan to cover a brand-name GLP-1 — Wegovy, Zepbound, Ozempic, Mounjaro, Saxenda, Foundayo, or Rybelsus — when it isn't on your plan's formulary, or to override a step-therapy or quantity-limit rule. You, your representative, or your prescriber can start the request, but approval requires the prescriber's supporting statement explaining why covered alternatives would be ineffective, would cause adverse effects, or have already failed.
For ACA-compliant commercial plans subject to 45 CFR § 156.122, the plan owes you a standard decision in ≤ 72 hours, or ≤ 24 hours when exigent circumstances apply. Medicare Part D follows the same clock under 42 CFR § 423.578. Most denials lose months not because the case is wrong but because the wrong paperwork was filed. This guide fixes that.
Editorial disclosure: We may earn a commission from some provider links on this page. That doesn't change our editorial conclusions or which providers we recommend.
Jump to
✅ What we actually verified for this guide
- · Federal exception timelines under 45 CFR § 156.122 (ACA / EHB plans) and 42 CFR § 423.578 (Medicare Part D)
- · Internal appeal and external review timelines per HealthCare.gov
- · CMS Medicare GLP-1 Bridge eligibility, drug list, and pricing per CMS (last updated April 21, 2026)
- · CVS Caremark removal of Zepbound from Standard Control, Advanced Control, and Value formulary templates effective July 1, 2025 per Caremark Business
- · FDA-approved indications for Wegovy, Zepbound, and Foundayo via FDA press releases
- · Ro Body program pricing and insurance support per ro.co/weight-loss/pricing (sponsored affiliate link, opens in a new tab) as of April 2026
- · Public external appeal patterns from the New York DFS searchable database
❌ What we did not invent
Specific approval rates. No insurer publishes them, so we describe the documentation profile that recurs in overturned decisions — not made-up percentages.
Start here: which denial do you actually have?
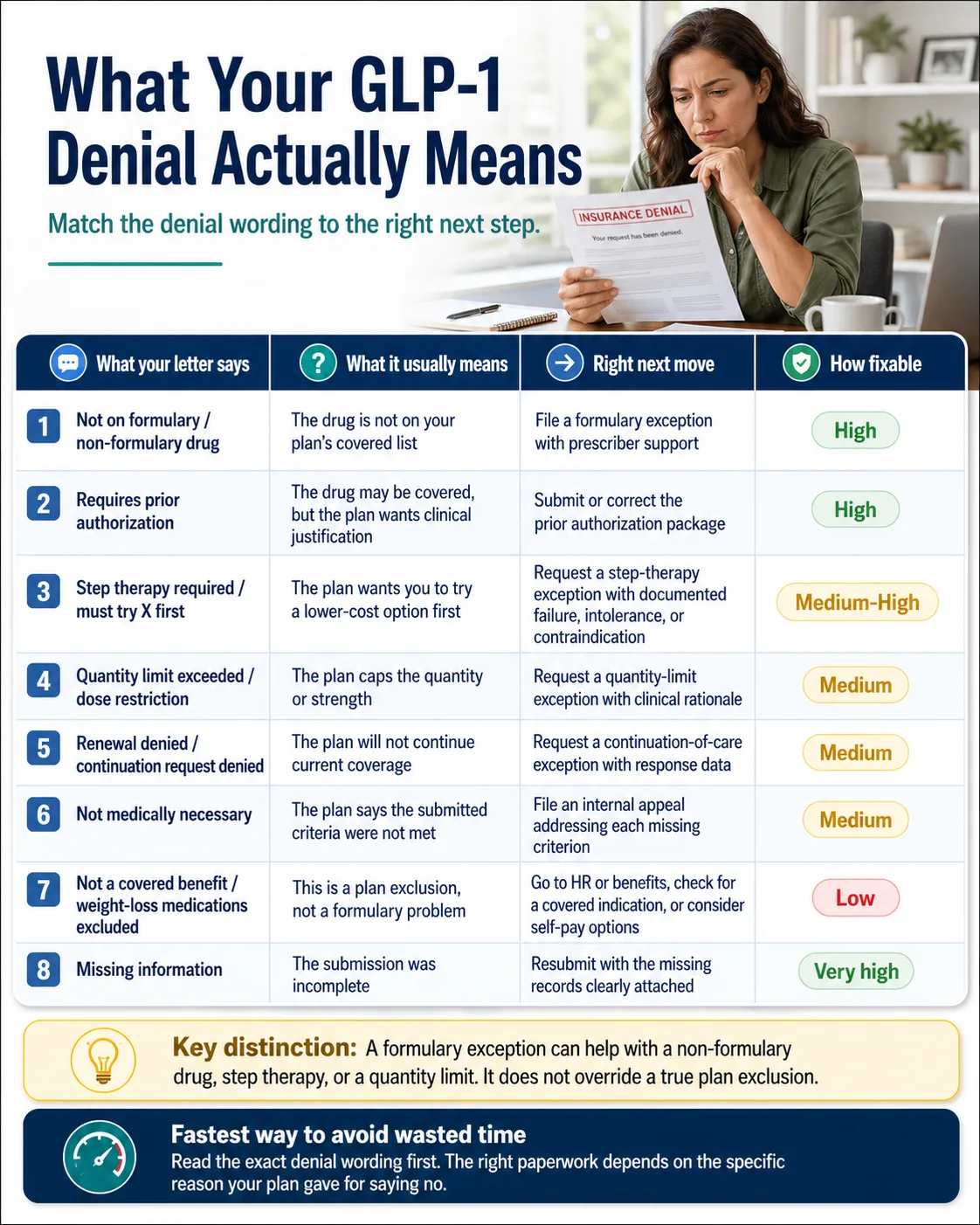
The single biggest reason people lose months on the wrong paperwork is that “denied” can mean five different things, and each one needs a different fix. Read the exact wording in your letter, find your row, and you'll know your move before you finish this page.
| What your letter says | What it usually means | The right next move | How fixable |
|---|---|---|---|
| “Not on formulary” / “non-formulary drug” | The drug isn’t on your plan’s covered list | File a formulary exception with prescriber support | High |
| “Requires prior authorization” | Drug is on formulary; plan wants clinical justification | Submit (or fix) the PA package | High |
| “Step therapy required” / “must try X first” | Plan wants you to fail-first on cheaper alternatives | Step-therapy exception with documented intolerance or contraindication | Medium-High |
| “Quantity limit exceeded” / “dose restriction” | Plan caps the quantity or strength | Quantity-limit exception with clinical rationale | Medium |
| “Renewal denied” / continuation request denied | Plan won’t keep covering you | Continuation-of-care exception with response data | Medium |
| “Not medically necessary” | PA criteria not met (or argued) | Internal appeal that addresses each missing criterion | Medium |
| “Not a covered benefit” / “weight-loss medications excluded” | Benefit was never purchased — this is a plan exclusion | Different game: HR escalation, alternative covered indication, or self-pay | Low |
| “Missing information” | Submission was incomplete | Resubmit with the missing items spelled out | Very high |
If you only do one thing on this page: figure out which of those eight rows you're in. Everything else flows from that.
What a GLP-1 formulary exception actually is — and the three cases when it works
A GLP-1 formulary exception is a federally regulated request that asks your insurance plan to cover a drug that isn't on your plan's formulary, or to override a utilization-management rule like step therapy or a quantity limit. It is grounded in two regulations: 45 CFR § 156.122 for ACA / essential-health-benefit plans, and 42 CFR § 423.578 for Medicare Part D. Both regulations require a prescriber's supporting statement explaining why covered alternatives would be less effective, would cause adverse effects, or have already failed under step therapy.
It works in three scenarios:
- The drug is not on your plan's formulary — the classic non-formulary exception.
- Step therapy — the plan wants you to “fail first” on a preferred drug; the exception waives the rule when you can document intolerance, contraindication, or prior failure.
- Quantity limits — the plan caps the dose or supply; the exception requests an override based on clinical need.
A tiering exception is a separate mechanism. It asks the plan to charge a non-preferred drug at a preferred-tier copay. CMS draws this distinction explicitly: formulary exceptions cover off-formulary drugs and rules; tiering exceptions cover cost-sharing. If your goal is a lower copay specifically, ask your prescriber whether a tiering exception applies.
The exception process does not work against a true plan exclusion. We'll come back to that wall in a moment, because it's where most wasted effort happens.
Exception vs. prior authorization vs. appeal vs. plan exclusion
These four terms get treated as interchangeable, and they aren't. Mixing them up is the single most common reason people file the wrong paperwork.
| Term | What it does | Who can file | Federal timing | Can it override? |
|---|---|---|---|---|
| Prior authorization (PA) | Approves a formulary drug for a specific patient | Prescriber | 15 days for treatment requests, 30 days for retrospective claims, 72 hours for urgent care per HealthCare.gov | Approves coverage of a covered drug |
| Formulary exception | Covers a non-formulary drug, or overrides step therapy / quantity limit | Patient, representative, or prescriber (prescriber supporting statement required) | 72 hours standard / 24 hours expedited under 45 CFR § 156.122 and 42 CFR § 423.578 | Overrides formulary, step therapy, quantity limit — not plan exclusion |
| Appeal | Challenges an already-issued denial of either of the above | Patient or prescriber | File internal within 180 days of denial; external review within 4 months of final denial. Medicare Part D Level 1 redetermination must be requested within 65 days. | Reverses an incorrect denial |
| Plan exclusion | A whole benefit category not in plan design | (n/a — set by employer / plan sponsor) | (n/a) | Nothing in the regulatory exception process overrides this |
If you remember one thing from this section: formulary exclusion ≠ plan exclusion. A formulary exclusion means the plan covers the category (weight-loss medications, GLP-1s) but not this specific drug. A plan exclusion means the plan never bought the category at all. The first is a paperwork problem. The second is a benefit-design problem, and you'll need a different lever.
The five denial paths — find yours, file the right one
Every GLP-1 denial we've ever read maps to one of five paths. Each has its own document set, timeline, and likelihood of success.
Path A — “Not on formulary” (formulary exclusion)
This is the strongest path for an exception. The plan covers GLP-1s in some form but not the specific drug your clinician prescribed. The prescriber files a formulary exception request with a supporting statement that all covered alternatives would not be as effective or would have adverse effects.
What wins this: documentation that you've already tried the formulary alternatives by name, dose, and duration, with the specific reason each one failed (side effect, contraindication, inadequate response).
Timing: for ACA / EHB plans, the standard exception decision is due no later than 72 hours after the plan receives the request, and the expedited decision is due no later than 24 hours when exigent circumstances apply.
Real example of the moment this matters most: CVS Caremark removed Zepbound from its Standard Control, Advanced Control, and Value formulary templates available to clients effective July 1, 2025, keeping Wegovy as the preferred GLP-1 (client-specific custom formularies may differ). This created a clear continuation-of-care exception scenario for affected patients stable on Zepbound under those templates.
Path B — “Step therapy required” / “must try X first”
The plan wants you to fail first on a cheaper or preferred drug — typically Contrave, Qsymia, phentermine, or (for GLP-1-class step therapy) the formulary-preferred GLP-1. The exception waives the rule.
What wins this: a documented prior trial of the step-therapy drug — with dates, doses, duration, and the specific outcome (intolerance, contraindication, lack of efficacy) — or a clinical contraindication that means the step drug is unsafe before trying.
State law often wins where stricter than federal. Many states have step-therapy override laws shorter than the federal 72-hour default. Colorado requires standard exception decisions in 72 hours and expedited in 24 hours. Florida requires step-therapy exception decisions in 15 days standard and 72 hours expedited. California gives you 72 hours standard and 24 hours urgent. Always check your state's step-therapy law.
Path C — “Quantity limit” / “dose restriction”
Less common for GLP-1s but it happens, especially at maintenance dosing or when you've titrated up faster than the plan's standard ramp. Same exception process; the supporting statement explains the clinical need for the higher dose, longer supply, or accelerated titration.
Path D — “Not medically necessary”
Technically a prior-authorization denial, not a formulary exception, but the procedural path is parallel. This is the most common GLP-1 denial in commercial plans. The denial letter should list the exact criteria you didn't meet — BMI threshold, comorbidity documentation, prior trial of weight-management interventions, A1C value. The internal appeal must rebut each one specifically.
What wins this: a Letter of Medical Necessity (LMN) that quotes the plan's own clinical policy back to the plan and walks through your case against each criterion. Most plans publish their criteria in medical policy bulletins — read them and cite them.
Path E — “Not a covered benefit” / “weight-loss medications excluded” (the wall)
This is the honest negative. The formulary exception process cannot fix a true plan exclusion. The benefit was never purchased — by you or by your employer — so there's no benefit to grant exceptions against. We'd rather tell you this in 30 seconds than watch you spend three months on paperwork that can't win.
But you have four real options:
- Check whether the same drug has a covered indication. Wegovy is FDA-approved for reducing major adverse cardiovascular events in adults with established cardiovascular disease and obesity or overweight. Zepbound is FDA-approved for moderate-to-severe obstructive sleep apnea in adults with obesity. Wegovy injection is also FDA-approved for MASH (metabolic dysfunction-associated steatohepatitis) in adults with moderate-to-advanced fibrosis. If you have one of those conditions documented, the prescription may be evaluated under a different covered indication; coverage still depends on the plan.
- Employer benefits escalation. If your plan is employer-sponsored, the employer chose the benefit design. HR can sometimes change it — KFF's 2025 employer survey found that 43% of firms with 5,000+ workers covered GLP-1s for weight loss in their largest plan, up from 28% the year before. The trend is moving, and HR can sometimes accelerate it for next plan year.
- External review. External review can occasionally overturn an exclusion if the denial mishandled a covered indication or if the plan's process was non-compliant. Worth filing if your case has any of those features.
- Cash-pay path. If exclusion is final, see our GLP-1 cost without insurance guide.
Want to know what your actual plan covers — without filing anything yet?
Ro runs a free GLP-1 Insurance Coverage Checker that contacts your plan and sends a personalized report on whether GLP-1 medications are covered, whether prior authorization is required, and what your estimated copay would be. No commitment, no charge to sign up.
Best for: commercial insurance & FDA-approved brand-name GLP-1 access. If you have Medicare, Medicaid, Tricare, or VA, file your exception directly with your plan instead.
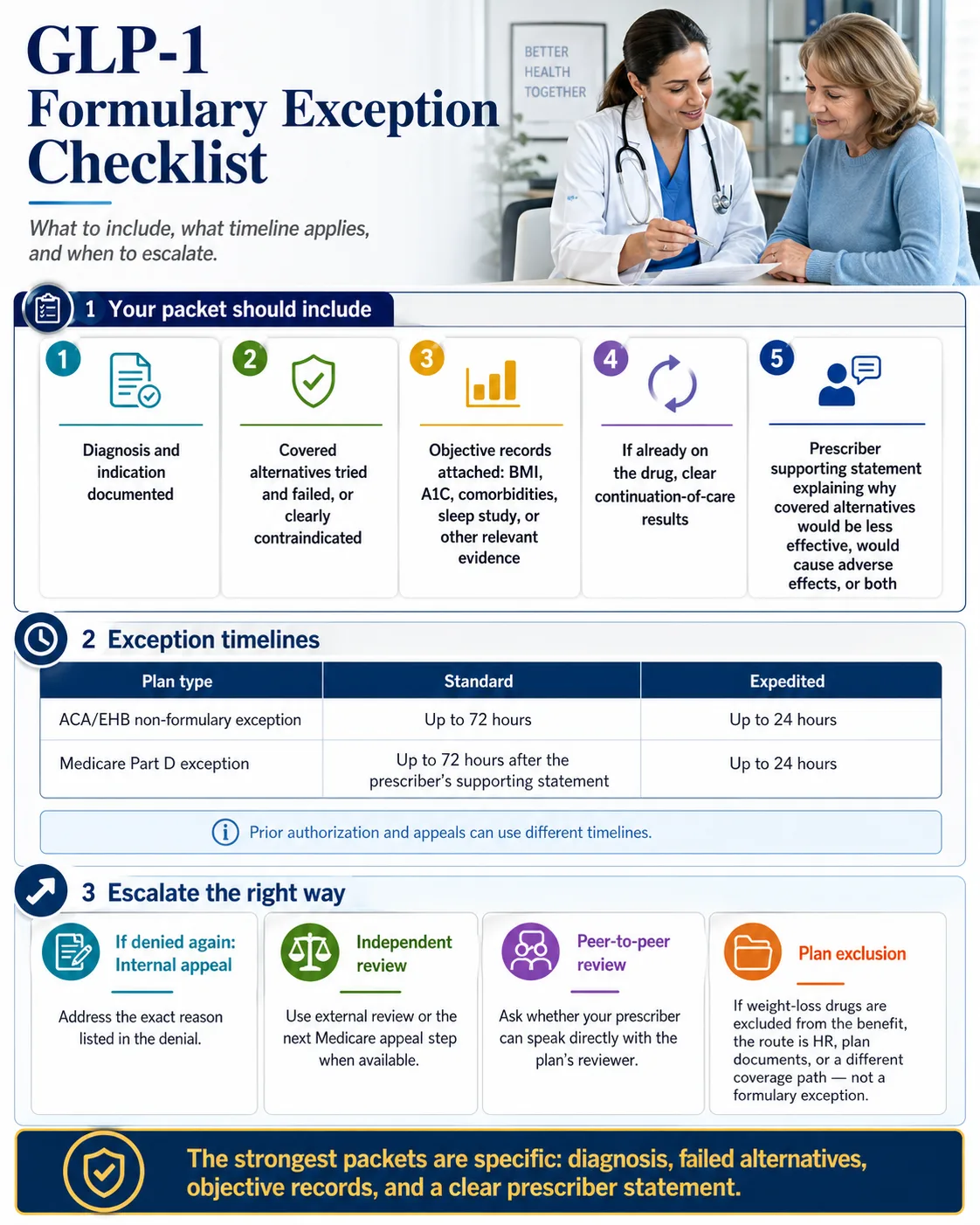
Your formulary exception checklist at a glance
Before you file, your packet should cover five things, and you should know which timeline applies to your plan type. The infographic below is the print-and-hand-to-prescriber version of the rest of this page.
The fixability score: is your exception worth filing?
Before your prescriber spends an hour writing a letter, run your case through this. We built this scoring around the documentation patterns that recur in publicly published external appeal decisions — both wins and losses. Score honestly. The number tells you whether to file as-is, fix the gaps first, or try a different lever.
| Factor | +2 | +1 | 0 |
|---|---|---|---|
| Denial wording | Non-formulary, step therapy, or quantity limit | Missing info / renewal denied / “not medically necessary” | “Not a covered benefit” / weight-loss exclusion |
| Diagnosis match | FDA-approved indication clearly documented (BMI ≥ 30, or BMI ≥ 27 + comorbidity, or T2DM with A1C, or MACE indication) | Indication exists but documentation is incomplete | Off-label or not in chart |
| Alternatives addressed | Tried and failed by name/dose/date, or contraindicated | Some attempts noted | No alternatives addressed |
| Objective records | BMI history, A1C, comorbidity records all attached | Records exist but partial | No records |
| Continuation status | Already stable on this drug with documented response | Recent start | New request, no continuation argument |
| Prescriber support | Strong LMN with chart notes and supporting statement | Basic note | No prescriber statement |
Read your score:
- 9–12 points: Your case has the documentation profile this guide recommends filing with: complete records, alternatives addressed, objective data, and prescriber support. Use the LMN template below and submit. This is not an approval guarantee — no scoring system can be — but it's the documentation profile that most often appears in overturned external review decisions.
- 5–8 points: File only after fixing the gaps. Identify the lowest-scoring rows, gather what's missing, and resubmit.
- 0–4 points: Stop and rethink. You may be on Path E, or your packet isn't where it needs to be yet. Use the alternatives section below.
How long does a GLP-1 formulary exception take?
For ACA-compliant commercial plans subject to 45 CFR § 156.122, a standard non-formulary exception decision is due no later than 72 hours after receipt of a complete request, and an expedited decision is due no later than 24 hours after receipt when exigent circumstances apply. Medicare Part D exceptions follow a similar 72-hour / 24-hour rule after the prescriber's supporting statement. Self-funded employer plans, prior authorizations, internal appeals, Medicaid, and plan exclusions can use different timelines — read your denial notice and Summary Plan Description for what applies to you.
| Plan type | Standard | Expedited | Internal appeal deadline | External review | Citation |
|---|---|---|---|---|---|
| ACA-compliant commercial / EHB plans | ≤ 72 hours after complete request | ≤ 24 hours when exigent | 180 days from denial | 4 months from final denial | 45 CFR § 156.122 |
| ERISA self-funded employer plan | Plan-defined; check Summary Plan Description | Often 72 hours when exigent | 180 days minimum per DOL | Per plan and ACA where applicable | ERISA + ACA |
| Medicare Part D exception | ≤ 72 hours after prescriber's supporting statement | ≤ 24 hours | Level 1 redetermination: 65 days to request; plan has 7 days standard, 72 hours expedited | Level 2 IRE: 60 days after redetermination | 42 CFR § 423.578 |
| Medicaid managed care | State-specific; typically ≤ 14 days standard / ≤ 72 hours expedited | State-specific | State-specific | State fair hearing | 42 CFR § 438.210 |
| State step-therapy laws (override federal where stricter) | CO 72h, FL 15d standard / 72h expedited, CA 72h / 24h urgent | Per state | Per state | Per state | State statute |
When you can request expedited review. Federal regulation defines exigent circumstances as a health condition that may seriously jeopardize your life, health, or ability to regain maximum function — or you're already on the drug and continuation is medically necessary. For GLP-1 patients, that typically includes:
- Established cardiovascular disease and you've been removed from Wegovy mid-treatment
- Type 2 diabetes with rising A1C off the drug
- Documented obstructive sleep apnea with desaturation events
- MASH with progressive fibrosis
- Continuation requests when stopping abruptly poses clinical risk
If any of those apply, the prescriber should check the “expedited” or “exigent circumstances” box on the form. The clock drops from 72 to 24 hours.
What should your prescriber include in a GLP-1 formulary exception request?
The Letter of Medical Necessity is the single most important document in a GLP-1 formulary exception. Federal regulation requires a prescriber's supporting statement; in practice, the plans that approve at the highest rates are reading for four things:
- A diagnosis with ICD-10 codes that matches an FDA-approved or covered indication
- Failure or contraindication of every covered alternative, by name, dose, duration, and outcome
- A specific reference to the plan's own coverage criteria, met point-by-point
- The regulatory supporting-statement language that the alternative would be less effective, cause adverse effects, or has already failed under step therapy
Below is the template structure, then seven plug-in clinical scenarios. Copy whichever scenario matches your case into the template and hand it to your prescriber.
ICD-10 codes shown are examples only. Use the diagnosis code documented by the treating clinician based on the patient's actual condition. The blocks below illustrate documentation structure — they are not coding instructions or a substitute for clinical judgment.
LMN Template Skeleton
[PRESCRIBER LETTERHEAD] [Date] [Plan / PBM Name] Attn: Pharmacy Exception Review Re: Formulary Exception Request — [Patient Name], DOB [XX/XX/XXXX], Member ID [###] Drug: [e.g., Wegovy 2.4 mg / Zepbound 7.5 mg / Ozempic 1.0 mg] Diagnosis (ICD-10): [code from scenario block below] Request type: [ ] Standard formulary exception (45 CFR § 156.122 / 42 CFR § 423.578) [ ] Expedited / exigent circumstances (≤ 24 hours) [ ] Step-therapy exception [ ] Continuation-of-care exception (drug removed from formulary mid-year) [ ] Quantity-limit exception Clinical justification: [INSERT SCENARIO BLOCK A–G BELOW] Prescriber's supporting statement (required by 45 CFR § 156.122 / 42 CFR § 423.578): "All formulary alternatives have been considered and are expected to be [less effective / cause adverse effects / be contraindicated] for this patient because [specific clinical reasoning]." Sincerely, [Prescriber Name, Credentials, NPI, Contact]
Scenario A — Wegovy for obesity (BMI ≥ 30)
Example ICD-10: E66.01 (morbid obesity due to excess calories) or E66.9 (obesity, unspecified)
Plug-in language: “Patient has documented BMI of [X.X] (height [XX in], weight [XX lbs]), meeting FDA-approved criteria for chronic weight management with semaglutide 2.4 mg. Patient previously trialed [Saxenda 3.0 mg / Qsymia 7.5/46 / Contrave 8/90] from [start date] to [end date], discontinued due to [specific side effect, contraindication, or inadequate response as defined by the plan's criteria — for example, the plan's specified weight-loss threshold after a defined trial period]. Patient has completed [duration] of structured lifestyle intervention with documented inadequate weight loss.”
Scenario B — Wegovy for overweight + comorbidity (BMI ≥ 27 + condition)
Example ICD-10: E66.3 (overweight) plus comorbidity code — I10 (hypertension), E11.9 (T2DM), E78.5 (dyslipidemia), G47.33 (OSA), or I25.10 (CV disease)
Plug-in language: “Patient has BMI [X.X] with [comorbidity] confirmed by [lab values, sleep study, etc.], meeting FDA-approved criteria for semaglutide 2.4 mg in adults with overweight and at least one weight-related condition. Failure of formulary alternative [name] documented as above.”
Scenario C — Zepbound for OSA + obesity
Example ICD-10: G47.33 (obstructive sleep apnea, adult) plus E66.01
Plug-in language: “Patient has moderate-to-severe obstructive sleep apnea (AHI [X] confirmed by polysomnography on [date]) with documented obesity (BMI [X.X]). Tirzepatide is FDA-approved for moderate-to-severe OSA in adults with obesity. CMS treats Zepbound for OSA as a Part-D-coverable use distinct from weight-management-only indications.”
Scenario D — Wegovy for MACE risk reduction
Example ICD-10: I25.10 (atherosclerotic heart disease) / I63.x (cerebral infarction sequelae) / I21.x (acute MI history) plus E66.x
Plug-in language: “Patient has established cardiovascular disease ([specific dx with date of event/diagnosis]) with overweight/obesity (BMI [X.X]). Semaglutide 2.4 mg is FDA-approved to reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction, non-fatal stroke) in adults with established cardiovascular disease and obesity or overweight. This indication is distinct from weight-loss-only and may be evaluated under a different covered indication; coverage still depends on the plan.”
This is the scenario that matters most for patients hitting Path E. If you have established CV disease, the MACE indication can route the same prescription through a different — and often covered — benefit category.
Scenario E — Wegovy for MASH
Example ICD-10: K75.81 (nonalcoholic steatohepatitis) plus K76.0 / fibrosis stage if known
Plug-in language: “Patient has biopsy- or imaging-confirmed MASH with moderate-to-advanced fibrosis (F2–F3) per [date and modality]. Wegovy (semaglutide) injection is FDA-approved to treat MASH in adults with moderate-to-advanced fibrosis. Alternative formulary therapies do not have an FDA-approved indication for this condition with this fibrosis stage.”
Scenario F — Continuation-of-care exception
Use when: patient was already established on the drug before formulary removal, drug change, or renewal denial.
Plug-in language: “Patient has been treated with [drug] since [start date] with documented response: baseline [BMI/A1C/weight] of [X], current [BMI/A1C/weight] of [X], representing [Y% improvement]. Abrupt discontinuation poses clinical risk of [weight regain / glycemic loss / withdrawal of cardioprotection / OSA progression]. Continuation-of-care exception is requested.”
This is the highest-conversion scenario when the documentation exists. Continuation-of-care requests are stronger when they document stable response, prior alternatives tried, and why switching is clinically inappropriate.
Scenario G — Step-therapy exception with documented intolerance
Plug-in language: “Patient has previously trialed [step-therapy drug — e.g., Saxenda, Contrave, Qsymia, or formulary-preferred GLP-1] from [start] to [end] at [dose]. Trial was discontinued due to [specific intolerance, contraindication, or inadequate response]. Required step-therapy drug [name] is contraindicated for this patient because [specific clinical reason — e.g., uncontrolled hypertension precluding phentermine, history of seizure precluding Contrave, mood disorder precluding Contrave, prior MTC precluding GLP-1 alternatives].”
What the supporting statement actually has to say
This is the language federal regulation requires, and it's the language that gets bounced when missing. From 42 CFR § 423.578: the prescriber must state that the non-formulary drug is necessary because all covered alternatives would not be as effective for the patient's condition, would have adverse effects on the patient, or — under step therapy — have already failed or are likely to fail.
A LMN missing this exact framing is the single most common reason for “incomplete clinical information” rejections. Use the language; don't paraphrase it.
This is a lot to put on a busy prescriber's plate.
A meaningful share of GLP-1 denials happen not because the patient doesn't qualify but because the documentation didn't make it across the finish line. Ro Body includes a dedicated insurance concierge that handles the prior-authorization package on your behalf for FDA-approved GLP-1s — Wegovy pen, Zepbound pen, and Ozempic are listed as eligible through insurance on Ro's pricing page. Ro Body members also get cash-pay access to Wegovy pill, Zepbound KwikPen, and Foundayo at the same prices as LillyDirect, NovoCare, and TrumpRx.
Pricing (verified April 2026): Ro Body membership is $39 for the first month, then $149/month — or as low as $74/month with annual prepay. Medication is billed separately.
Not for everyone: Ro doesn’t currently coordinate insurance for Medicare, Medicaid, Tricare, or VA plans. FEHB members can use the concierge.
What evidence wins or loses GLP-1 formulary exception appeals?
This is where most pages on this topic stop being useful. They tell you what to write but not what reviewers actually look at when they say yes or no. We pulled patterns from the New York Department of Financial Services external appeals database — a publicly searchable registry of independent external appeal decisions — and read the GLP-1 cases to extract what mattered. NY DFS itself notes these decisions are case-specific and shouldn't be treated as guarantees for other patients. Agreed. But the patterns that recur across decisions are the closest thing to public ground truth on what reviewers reward.
Methodology
We reviewed publicly published external appeal decisions involving GLP-1 medications (Mounjaro, Ozempic, Rybelsus, Wegovy) where formulary exceptions were the issue. We extracted the medication, the diagnosis, the outcome, the evidence reviewers cited, and the practical lesson. This is a pattern review, not a win-rate study. Specific case numbers below can be verified by readers and clinicians directly in the NY DFS database.
Sample decisions and the lesson from each
| Case | Drug / situation | Outcome | What mattered |
|---|---|---|---|
| 202304-161705 | Wegovy denial | Upheld (denied) | The record lacked medical records, BMI documentation, and evidence of a 3-month non-medical weight-management program. |
| 202210-155007 | Mounjaro for obesity | Upheld (denied) | The plan had named formulary alternatives; the record did not show the patient had tried or could not use them. |
| 202305-162818 | Mounjaro for obesity with comorbidities | Overturned (won) | Multiple comorbidities, prior medication attempts including Ozempic and Rybelsus, weight-loss program participation, and tolerability issues with alternatives all documented. |
| 202305-162722 | Mounjaro continuation for type 2 diabetes | Overturned (won) | Trulicity and Victoza failure documented, intolerance to Ozempic and metformin shown, stability on Mounjaro and A1C documented. |
What the upheld (denied) appeals had in common
- Missing medical records. The most common reason for an upheld denial in external review is incomplete documentation. Reviewers can't overturn a plan when there's no chart evidence of the diagnosis, BMI history, lab values, or prior trials.
- Formulary alternatives never addressed. When the plan named specific alternatives, and the appeal didn't address each one specifically, reviewers consistently sided with the plan.
- No documented intolerance or contraindication for required alternatives. “Patient prefers this drug” is not a clinical argument that wins external review.
- The denial was actually a benefit exclusion. External review can sometimes catch this and route the case differently, but a true benefit exclusion can't be overturned via medical-necessity review.
What the overturned (approved) appeals had in common
- Multiple comorbidities documented with their own ICD-10 codes in the chart.
- Prior trial history with specific outcomes — drugs by name, with start/stop dates, doses, and the specific intolerance, contraindication, or inadequate response.
- Continuation stability documented when the patient was already on the requested drug and the appeal showed measurable improvement.
- Objective labs that showed urgency — established CV disease, sleep-apnea desaturation events, very elevated A1C.
- Formulation-specific medical reasons — when the appeal explained why the specific formulation mattered (oral vs. injectable, weekly vs. daily for adherence).
The pattern in plain language
Winning GLP-1 exception appeals answer five questions cleanly:
- Why this drug? (FDA-approved indication match)
- Why not the formulary alternatives? (each one addressed by name)
- What objective data proves the medical need? (BMI, A1C, comorbidity codes, sleep study, fibrosis stage)
- What happened on prior therapies? (dates, doses, outcomes)
- What happens if the patient is forced to switch or stop? (continuation rationale)
Most losing appeals miss two or more of those questions. The complete documentation profile — prior trials, comorbidities, contraindications, and objective records — is the recurring pattern in the public overturned cases we reviewed.
How to find your PBM and the right exception form
Even with the same federal timeline, every PBM has its own form, portal, and quirks. Submitting on the wrong form — or to the wrong fax — is one of the most common reasons for processing delays. Here's how to find what applies to you.
Step 1 — Identify your PBM.
Look at the back of your insurance card. The PBM name and member-services phone number are listed there separately from your medical-coverage carrier. The most common PBMs are CVS Caremark, Express Scripts (Evernorth), OptumRx, Humana Pharmacy Solutions, Prime Therapeutics, and MedImpact. Common pattern: medical carrier = BCBS / Aetna / UHC / Cigna; PBM = a different name (often CVS Caremark, Express Scripts, or OptumRx).
Step 2 — Call the PBM with this script.
“I'm calling about a denied GLP-1 prescription for [drug name]. My denial letter says [exact wording]. Can you tell me whether this is a non-formulary denial, prior-authorization denial, step-therapy denial, quantity-limit denial, or benefit exclusion? Please send me the exact criteria, the correct formulary exception form for my prescriber, the submission method (portal, fax, or phone), the appeal deadline, and a call reference number for this conversation.”
Step 3 — Note what you learn:
- The exact form name (e.g., “Wegovy Prior Authorization Form” vs. “Non-Formulary Exception Request”)
- The correct submission method (most PBMs accept electronic prior authorization through CoverMyMeds, SureScripts, or their own provider portal)
- The fax number if portal isn't available
- Whether expedited review is available and how to flag it
Step 4 — Verify GLP-1-specific notes for your PBM.
Two specific 2026 details worth confirming:
- CVS Caremark (Standard Control / Advanced Control / Value templates): Wegovy is the preferred GLP-1 for 2026; Zepbound was removed effective July 1, 2025. Exception path is open for documented Wegovy intolerance or inadequate response. Client-specific custom formularies may differ.
- BCBS-affiliated plans (often via Prime Therapeutics): Several BCBS affiliates have made benefit-design changes to GLP-1 weight-loss coverage. Confirm whether your specific BCBS affiliate has a benefit exclusion (Path E) versus a formulary exclusion (Path A) — the difference determines whether the exception process can help. See our GLP-1 providers that accept Blue Cross guide for plan-specific details.
Medicare Part D, the GLP-1 Bridge, and what changes in July 2026
For Medicare patients, the formulary exception process exists, but the rules are different. Medicare Part D covers GLP-1s only for FDA-approved indications other than weight loss alone — that's a statutory exclusion dating to the Medicare Modernization Act of 2003. For GLP-1s, that means Part D plans can cover:
- Ozempic, Mounjaro, Rybelsus for type 2 diabetes
- Wegovy for cardiovascular risk reduction in adults with established CV disease and obesity/overweight
- Zepbound for moderate-to-severe obstructive sleep apnea in adults with obesity
If you've been denied a Part-D-coverable use, file the exception under 42 CFR § 423.578. Same 72-hour standard / 24-hour expedited timeline as commercial. If denied, you have 65 days to request Level 1 redetermination, and Level 2 (Independent Review Entity) is 60 days after that.
What changes July 1, 2026: the Medicare GLP-1 Bridge
CMS announced the Medicare GLP-1 Bridge demonstration on December 23, 2025 and updated the program details on April 21, 2026. The Bridge runs from July 1, 2026 through December 31, 2027. Eligible Part D beneficiaries can access certain GLP-1 drugs at a net price of $245 per monthly supply with a flat $50 copay, processed through a separate central processor (Humana, current administrator of the LI NET program) outside the standard Part D benefit flow.
Bridge drugs (per CMS, as of April 2026):
- Foundayo — all formulations
- Wegovy — injection and tablets, all formulations
- Zepbound KwikPen only — Zepbound single-dose vials and single-dose pens are NOT included
Bridge eligibility criteria — three tiers (you only need to meet one):
| Tier | BMI threshold | Required conditions |
|---|---|---|
| Tier 1 | BMI ≥ 35 | None required |
| Tier 2 | BMI ≥ 30 | At least one of: heart failure with preserved ejection fraction (HFpEF); uncontrolled hypertension (BP > 140/90 on 2+ antihypertensive medications); chronic kidney disease stage 3a or above |
| Tier 3 | BMI ≥ 27 | At least one of: pre-diabetes (per ADA guidelines); previous myocardial infarction; previous stroke; symptomatic peripheral artery disease |
BMI is measured at the time of GLP-1 therapy initiation, not at the patient's all-time highest weight.
A few additional things matter:
- The Bridge does not replace your Part D appeal rights. CMS explicitly states that the Bridge does not modify beneficiary appeal rights, including exception requests. If your prescription is for a Part-D-coverable use (T2DM, MACE, OSA), it stays in the regular Part D process — including exceptions and appeals. Don't try to route a Zepbound-for-OSA prescription through the Bridge; that's the regular Part D process.
- Prior authorization goes to the central processor, not your Part D plan. Your prescriber submits the PA to Humana's central processor, not your plan's PBM.
For a deeper walk-through with a tier-by-tier eligibility checker, see our Medicare GLP-1 Bridge program guide.
What to do if your formulary exception is denied
A denied exception is not the end. There are three escalation paths, and which one fits depends on what the denial said.
Internal second-level appeal
Most plans offer a second internal review with new evidence. Commercial plans typically allow up to 180 days from the denial. This is where you fix the gap the first denial called out — missing documentation, an unaddressed criterion, a formulary alternative the prescriber didn't account for. Most denials cite a specific reason; the appeal must address that exact reason.
External / Independent Review Organization (IRO) review
Required by federal law for ACA-compliant plans after internal appeals are exhausted. For Medicare Part D, the parallel path is redetermination (Level 1) → reconsideration by the Independent Review Entity (Level 2) → ALJ (Level 3) → MAC (Level 4) → Federal District Court (Level 5). The IRO reviewer is independent of the plan, and the decision is binding. This is where many cases turn — see the patterns above for what wins external review.
Peer-to-peer review
The prescriber requests a phone conversation with the plan's medical director. It's clinical-to-clinical instead of paperwork-to-bot, and it's free. Always ask if it's available before going to formal external review — it's faster and worth trying.
State insurance commissioner / DOL ERISA complaint
For fully insured plans, your state department of insurance handles complaints about plan compliance. For self-funded employer plans, the federal Department of Labor handles ERISA complaints. Don't file with the wrong regulator — the most common procedural mistake. If your plan is your employer's plan, it's almost certainly ERISA, and your state DOI doesn't have jurisdiction over it.
While you wait — protecting your treatment during the 72-hour window
The federal clock for ACA / EHB exception decisions is 72 hours standard or 24 hours expedited. You don't have to be at zero treatment during that window.
- Ask about a transition fill or continuation fill. If you were already on the drug, ask your plan whether a temporary fill is available. Availability depends on plan type, the formulary-change rules, and your plan's transition policy — most ACA-compliant plans have one, but it isn't universal.
- Manufacturer self-pay options. Wegovy through NovoCare and Zepbound through LillyDirect have published cash-pay options below the $1,300+ retail price.
- Ro matches LillyDirect, NovoCare, and TrumpRx pricing on the medication side, with separate Ro Body membership.
- Bridge with a clinically appropriate alternative. Your prescriber may bridge with a covered alternative for the duration of the appeal. Document the clinical reasoning.
- Don't switch to compounded mid-appeal without a clinician. Compounded GLP-1 medications are not FDA-approved. The FDA has stated that compounded GLP-1 drugs are not FDA-approved and do not undergo FDA review for safety, effectiveness, or quality before marketing. Switching from an FDA-approved drug to a compounded one mid-appeal can complicate documentation and clinical continuity.
Can Ro or Sesame Care help after a GLP-1 formulary denial?
Two telehealth providers come up most for readers in this exact situation, and they fit different cases.
Ro Body — for insurance-sensitive readers wanting brand-name coverage
Ro is the strongest fit when your goal is brand-name FDA-approved GLP-1 access through your insurance. It includes a dedicated insurance concierge (sponsored affiliate link, opens in a new tab) that helps with benefits verification and prior-authorization paperwork. Ro's pricing page lists Wegovy pen, Zepbound pen, and Ozempic as eligible through insurance; the free GLP-1 Insurance Coverage Checker (sponsored affiliate link, opens in a new tab) runs your real plan against the formulary before you commit.
Ro Body members can also access Wegovy (pen, pill), Zepbound (KwikPen, vial), Foundayo, and Ozempic on a cash-pay basis at the same prices as LillyDirect, NovoCare, and TrumpRx.
| What we verified | |
|---|---|
| Best fit | Commercial insurance + FDA-approved brand-name GLP-1 access goal |
| Membership | $39 first month, $149/month monthly plan, or as low as $74/month with annual prepay |
| Insurance concierge | Yes — eligible GLP-1s through insurance listed by Ro: Wegovy pen, Zepbound pen, Ozempic |
| Cash-pay GLP-1s | Wegovy pen and pill, Zepbound KwikPen and vial, Foundayo, Ozempic; medication priced same as LillyDirect, NovoCare, TrumpRx |
| Government insurance | Does not coordinate Medicare, Medicaid, Tricare, or VA. FEHB members can use the concierge |
| Last verified | April 2026 (ro.co/weight-loss/pricing) |
Includes the insurance concierge that handles the prior-authorization package.
Sesame Care — for self-pay branded GLP-1 access without a recurring membership
Sesame is a fit if you've concluded insurance won't work and you want branded GLP-1 access without a recurring concierge membership. Sesame's Costco partnership (sponsored affiliate link, opens in a new tab) gives Costco members access to Ozempic and Wegovy at $349/month, with $199/month for the lowest two doses for the first two months for new patients (per Sesame's published pricing). Costco membership is required for Costco pricing; Sesame doesn't have an insurance concierge and isn't built for fighting denials — that's not its lane.
| What we verified | |
|---|---|
| Best fit | Costco members or self-pay shoppers wanting branded access without a concierge membership |
| Pricing | Ozempic / Wegovy at $349/month; $199/month for lowest two Wegovy doses, first two months, new patients (per Sesame) |
| Costco membership | Required for Costco pricing |
| Insurance support | None for fighting denials |
| Last verified | April 2026 (sesamecare.com) |
Especially useful for Costco members on Ozempic or Wegovy.
Who shouldn't click any provider link yet
- You're on Medicare or Medicaid and your denial is for a Part-D-coverable indication — file the exception with your plan first.
- Your employer plan has a true weight-loss benefit exclusion — start with HR before spending on a membership.
- You're in clinical distress (rising A1C, stopped a stable medication abruptly, recent CV event) — call your prescribing clinician now, not a telehealth signup.
Scripts and templates: what to say to whom
You'll spend less time arguing if you go in with the exact wording that works.
Insurer phone script
“I'm calling about a denied GLP-1 prescription for [drug name]. My denial letter dated [date] says [exact wording from letter]. Can you confirm whether this is a non-formulary denial, prior-authorization denial, step-therapy denial, quantity-limit denial, or benefit exclusion? Please send me the exact criteria, the correct formulary exception form for my prescriber, the submission method (portal, fax, or phone), the appeal deadline, and a call reference number for this conversation.”
Note the call reference number. Note the agent's name. Note the date and time. You'll want it later.
Prescriber message
“My plan denied [drug name] and the denial letter says [exact wording]. They told me the next step is [formulary exception / prior authorization / appeal]. Can your office submit the attached plan-specific form, with chart notes including BMI/A1C history, comorbidity diagnoses, prior medication trials with dates and outcomes, and a Letter of Medical Necessity? I have the LMN scenario block that matches my case below — please feel free to use it as a starting point.”
Attach the LMN scenario block (A through G) that matches your situation.
HR / benefits administrator email
Hi [HR/benefits contact],
My health plan denied [drug name] because [exact denial wording]. I'm trying to determine whether this is an employer-level benefit exclusion or a formulary issue I can resolve through the exception process. Can you confirm:
(1) Does our plan have an anti-obesity medication or weight-management drug benefit?
(2) If excluded, was that a plan-design choice, and is it under review for the next plan year?
(3) If a formulary exception is possible, what's the correct submission path?I'd appreciate any plan documents — Summary Plan Description or Evidence of Coverage — that explain the current benefit. Thanks for the help.
Appeal cover letter skeleton
[Date] [Plan address] Re: Appeal of Formulary Exception Denial Patient: [Name] Member ID: [###] Drug: [Name and dose] Date of denial: [Date] Denial reason cited by plan: [Exact wording] The plan's denial dated [date] is appealed for the following reasons: 1. [Specific factual or clinical correction] 2. [Plan criteria addressed point-by-point] 3. [Regulatory citation — 45 CFR § 156.122 / 42 CFR § 423.578] Attached: - Original denial letter - Letter of Medical Necessity - Updated chart notes - Prior medication trial log - BMI/A1C history - [Other supporting records] Sincerely, [Patient name and signature] [Prescriber name, NPI, signature]
What to do if insurance is still a dead end
If you've worked through the paths above and concluded insurance won't cover the drug — true plan exclusion, exhausted appeals, or your plan year ends in months and the next year's plan is no better — these are the practical alternatives, in order of how readers most often use them.
- Open enrollment plan shopping. If open enrollment is coming, compare formularies before you enroll. Specifically check: does the plan cover anti-obesity medications? Which GLP-1s are on formulary? Is prior authorization required? Is step therapy required? Are renewals based on baseline BMI or current BMI? Are CV / OSA / MASH indications handled differently from weight-loss-only?
- Manufacturer-direct cash pay. Wegovy through NovoCare and Zepbound through LillyDirect publish cash prices substantially below pharmacy retail. Legitimate path that doesn't require a membership.
- Telehealth with insurance support (FDA-approved). Ro Body for FDA-approved branded access with the concierge handling paperwork.
- Telehealth for self-pay branded (no recurring concierge). Sesame Care, particularly for Costco members.
- Self-pay compounded. Compounded GLP-1 medications are not FDA-approved. The FDA has warned against marketing compounded GLP-1s as generics or as having clinically proven results, and they should not be described as interchangeable with FDA-approved brand medications. If your clinician concludes a compounded option is appropriate for your case, that's a clinical conversation to have with them. We compare cash-pay paths in our GLP-1 cost without insurance guide.
Frequently asked questions
Who actually files the formulary exception — me or my doctor?
You, your representative, or your prescriber can start the request. Approval requires the prescriber's supporting statement that the non-formulary drug is medically necessary, so in practice the exception cannot succeed without your prescriber's involvement. You can prompt the process, request the form, and provide your prescriber with the documentation they need.
How long does a GLP-1 formulary exception take?
For ACA-compliant commercial plans, the standard exception decision is due within 72 hours of a complete request, or 24 hours for expedited review under exigent circumstances. Medicare Part D follows a similar 72/24-hour rule. Self-funded employer plans set their own timelines but often align with the federal default for pre-service requests.
Can a formulary exception override a plan that excludes weight-loss medications?
No. A formulary exception works against the formulary and against utilization rules like step therapy and quantity limits. A plan exclusion is a benefit-design decision — the plan didn't purchase that benefit at all — and the exception process can't grant a benefit that wasn't included.
What's the difference between a formulary exception and a prior authorization?
A prior authorization is required approval for a drug that is on your plan's formulary. A formulary exception is a request to cover a drug that isn't on the formulary, or to override step therapy or a quantity limit. Both use the same 72-hour federal timeline for ACA / EHB plans, but they solve different problems. Prior authorization timing for some claim types differs — HealthCare.gov says insurers must notify you within 15 days for treatment requests, 30 days for retrospective claims, and 72 hours for urgent care.
My GLP-1 was on formulary last year and got dropped for 2026. What can I do?
Request a continuation-of-care exception. Plans must address mid-year formulary changes for established patients, and continuation-of-care requests are stronger when documentation includes baseline measurements, current measurements, treatment response, and the clinical risk of stopping or switching. CVS Caremark removed Zepbound from its Standard Control, Advanced Control, and Value formulary templates effective July 1, 2025; affected patients with documented stable response on Zepbound have a clean continuation-of-care path.
Does the Medicare GLP-1 Bridge replace formulary exceptions?
No. CMS has explicitly stated the Bridge does not modify beneficiary appeal rights or exception requests. Part D plans must continue handling formulary exceptions for Part-D-coverable uses (T2DM, MACE, OSA) through the regular process. The Bridge runs in parallel from July 1, 2026 to December 31, 2027 and is a separate pathway specifically for weight-management uses.
Will an approved formulary exception lower my copay?
Not necessarily. Approval may let the plan cover the drug, but cost-sharing depends on the tier the plan assigns. Some plans state explicitly that an approved exception does not change out-of-pocket costs. If your goal is a lower copay specifically, ask your prescriber whether a tiering exception (separate from a formulary exception) applies.
What's the success rate for GLP-1 formulary exceptions?
There's no single published success rate, and we won't invent one. What's consistently documented in the public external review record is that complete documentation of prior trials, comorbidities, contraindications, and objective records is the recurring pattern in overturned cases.
Can I file my own exception without my doctor?
You can initiate a coverage-determination request, but federal regulation requires a prescriber's supporting statement before the plan can approve. In practice, the exception cannot succeed without your prescriber's involvement.
Does Ro's insurance concierge handle formulary exceptions?
Ro's insurance concierge helps with benefits verification and prior-authorization paperwork. Per Ro's pricing page, eligible GLP-1s through insurance are Wegovy pen, Zepbound pen, and Ozempic. Ro doesn't currently coordinate insurance for Medicare, Tricare, Medicaid, or VA plans; FEHB members can use the concierge. Ro Body membership is $39 first month / $149 monthly / as low as $74/month with annual prepay (verified April 2026).
What if my doctor refuses to write the letter?
Ask whether they can complete the plan's formulary exception form even without a full LMN — many plans accept the form alone with chart notes attached. If the prescriber believes the medication isn't appropriate for you, ask what alternative they'd recommend and whether that alternative is on your formulary.
Can I use a compounded GLP-1 while my exception is pending?
Discuss this with a licensed clinician before doing it. Compounded GLP-1 medications are not FDA-approved and should not be described as interchangeable with FDA-approved brand medications. The FDA has stated that compounded GLP-1 drugs do not undergo FDA review for safety, effectiveness, or quality before marketing. Switching from an FDA-approved drug to a compounded one mid-appeal can complicate documentation and clinical continuity.
Methodology and limitations
We built this guide from primary sources: the Code of Federal Regulations, CMS guidance on Part D exceptions, HealthCare.gov on internal appeals, the FDA's published GLP-1 approvals, the New York Department of Financial Services external appeals database, CMS guidance on the Medicare GLP-1 Bridge, payer-published policy bulletins, and current provider pricing pages.
What we can't tell you: whether your specific exception will succeed. Insurance plans vary by employer, state, plan year, diagnosis, medication, and prescriber documentation. This guide helps you classify the denial and prepare the right next step. Only your insurer, your plan documents, and your clinician can confirm what applies to your case. This is not medical, legal, or insurance advice.
Last verified: April 29, 2026. Next scheduled review: July 2026, timed to the launch of the Medicare GLP-1 Bridge demonstration.
Still not sure which GLP-1 path is right for you?
You might leave this page knowing your denial is fixable and exactly what to do — that's the goal. But if you're still weighing whether to fight insurance, switch to manufacturer cash-pay, find a telehealth concierge, or wait out open enrollment, the right next step depends on details we haven't asked you about.
No email required · 5 questions · Personalized recommendation
We'll ask about your insurance, your medication, your goals, and your situation, then give you a specific recommendation — including whether to file an exception, who can help with paperwork, and which provider matches your case.
If you already know what you want next:
- Want someone to handle the exception paperwork for FDA-approved GLP-1s? See if Ro Body fits your case → (sponsored affiliate link, opens in a new tab) $39 first month, as low as $74/month with annual prepay, insurance concierge included.
- Want self-pay branded access without a recurring concierge membership? Compare Sesame Care pricing → (sponsored affiliate link, opens in a new tab) particularly useful for Costco members on Ozempic or Wegovy.
- Need the letter of medical necessity itself? Use our GLP-1 LMN guide.
- Decided cash-pay is the path? Read our GLP-1 cost without insurance guide.
- On Medicare and want to know if you'll qualify for the Bridge? See our Medicare GLP-1 Bridge program guide.
- Want to know which providers work with which insurers? See Best GLP-1 providers that accept insurance and GLP-1 providers that accept Blue Cross.
Medical disclaimer: This content is for informational purposes only and does not replace professional medical advice. Always consult your healthcare provider before starting any new medication. Regulatory and pricing information reflects verified data as of April 29, 2026 and may change.
Related guides
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers.