How to Bypass Step Therapy for GLP-1: 6 Grounds, Scripts, and the Real 2026 Timeline
Published:
By The RX Index Editorial Team • Last verified: April 17, 2026 • Published April 18, 2026 • Next recheck: July 2026
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers.
Not medical, legal, or insurance advice. For plan-specific questions, contact your insurer directly.
“Bypassing” step therapy is shorthand for using the exception and appeal paths your plan already has on the books. Most readers who get denied for step therapy have a real case under one of six grounds — prior trial failure, contraindication, expected ineffectiveness, stability on current therapy, risk of harm from delay, or clinical judgment. Your prescriber files the request. Under state-regulated plans, most insurers must respond within 72 hours (24 hours for urgent cases). Under ACA rules, you generally have up to 180 days to file an internal appeal.
One honest thing first: if your plan completely excludes weight-loss medications as a benefit, a step-therapy appeal can’t unlock coverage. We’ll show you how to spot that in two minutes so you don’t burn 45 days on the wrong fight.
See which exception ground fits your denial — 60-second matcher
Get matched to your strongest exception ground →1. What “Bypass Step Therapy for GLP-1” Actually Means
Step therapy — sometimes called “fail first” — is when your insurance requires you to try one or more preferred or cheaper medications for a set time before it’ll cover the medication your doctor prescribed. For GLP-1s, the step-one drugs vary by plan and indication. Common examples include metformin (for diabetes-indicated requests), phentermine or Contrave (for weight-management requests), orlistat, Qsymia, or an older/cheaper GLP-1 like Saxenda or Victoza.
There are five legitimate ways out of a step therapy denial. You only need one.
Correct the prior authorization
Sometimes the denial is a documentation gap, not a real rejection. Fixable in 48 hours.
Request a step therapy exception
Your prescriber (or you, on Medicare Part D) files a specific request citing one of the six grounds in Section 4.
Request a continuity of care / prior-approval transfer
If you’re already stable on a GLP-1 under a prior plan.
File an internal appeal
After an exception denial, ACA-regulated plans give you up to 180 days to escalate. Medicare Part D uses shorter windows.
Request an external review
After a final internal denial, generally within four months for ACA-regulated plans. Binding on the insurer.
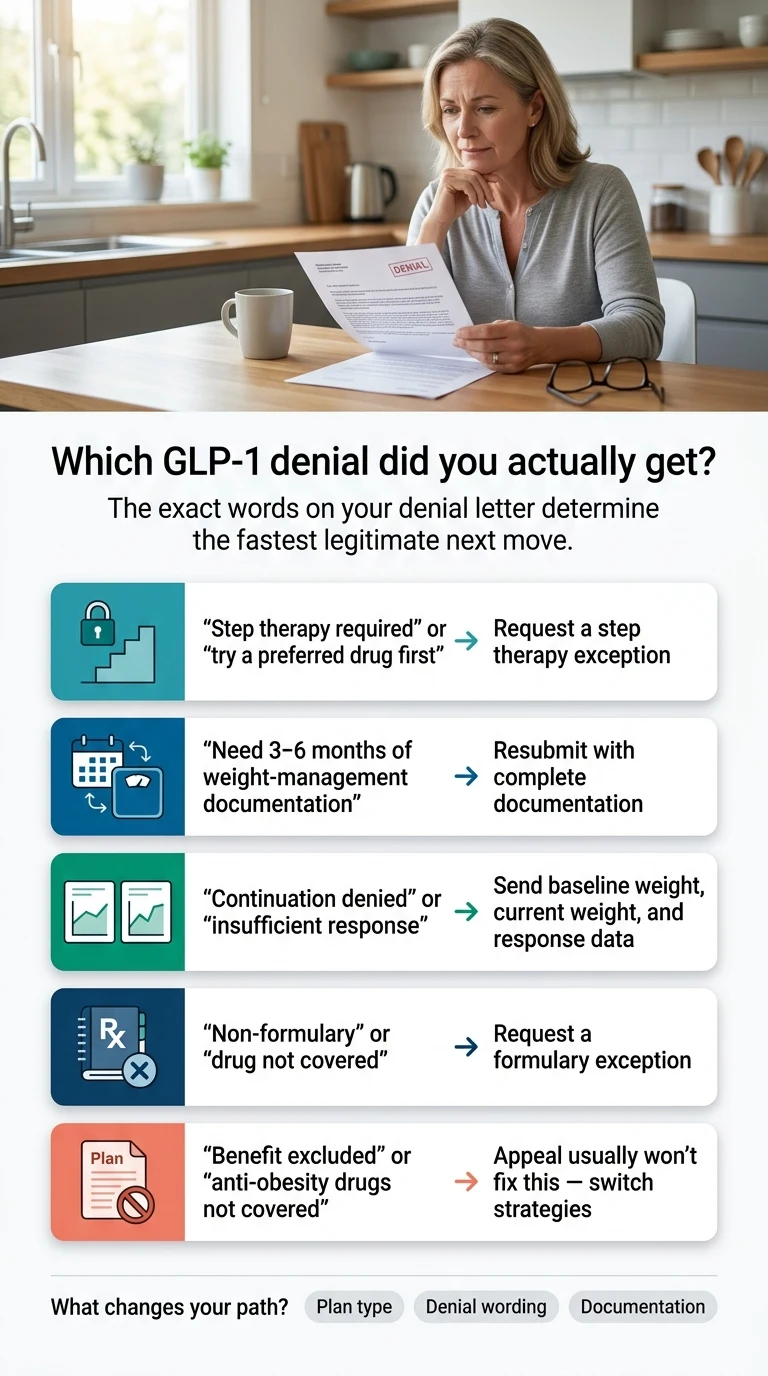
2. Which Denial Did You Actually Get? The Triage Table
Your denial letter is the starting line. Match the exact wording to the row below before you do anything else. “Step therapy required,” “benefit excluded,” and “continuation denied” all feel the same at the pharmacy counter. Each needs a different response.
| What your denial says | What it means | Fastest legitimate move | Winnability |
|---|---|---|---|
| “Step therapy required” or “you must try a preferred drug first” | Plan wants evidence you tried (or can’t safely try) a cheaper drug | Step therapy exception request citing prior failure, contraindication, or expected ineffectiveness | ✅ Often winnable if one of the six grounds fits |
| “You haven’t tried [phentermine / metformin / Contrave]” | Insurer needs documented prior trial or a reason you can’t use that drug | Document prior fill history, dates, dose, outcome, side effects — or cite contraindication | ✅ Often the most straightforward to overturn |
| “Needs 3–6 months of documented weight-management participation” | Some plans require documented program participation before approving initial coverage. CVS Caremark requires at least 6 months. | Gather dated records of participation and resubmit PA with documentation. Appealing won’t help — meeting the requirement will. | ⚠️ Not a step-therapy appeal — requires documentation, not exception request |
| “Continuation denied — insufficient response” | Insurer wants proof the current GLP-1 is working. CVS Caremark requires at least 3 months at stable maintenance dose plus 5% baseline weight loss. | Submit baseline weight, current weight, dosing history, and response documentation | ✅ Generally winnable when response data exists |
| “Not medically necessary” | Clinical-criteria gap (BMI, comorbidities, indication) or thin letter of medical necessity | Supplemental letter of medical necessity with BMI, comorbidities, ICD-10 codes; request peer-to-peer review | ✅ Often winnable with peer-to-peer |
| “Non-formulary” or “drug not covered” | Drug itself isn’t on the plan’s list | Formulary exception request (different form than step therapy exception, same spirit) | ⚠️ Depends on whether a covered alternative exists |
| “Benefit excluded” or “plan does not cover anti-obesity medications” | Plan doesn’t cover weight-loss drugs as a category | Stop. An appeal won’t fix this. Route to HR for plan modification, or switch to self-pay. | ❌ Rarely winnable through appeals |
| “Off-label use” | Prescribed for an indication not FDA-approved for that drug | Switch to an FDA-approved option for your indication, or appeal with strong clinical rationale | ⚠️ Sometimes winnable; documentation burden is high |
3. Does Your GLP-1 and Indication Change the Strategy?
Yes — significantly. Coverage and step therapy rules differ based on what the drug is approved for and what you’re seeking it for. A lot of first-round denials are really indication-coding errors, not clinical disputes.
1. You were prescribed Ozempic or Mounjaro for weight loss (off-label)
Coverage denials for off-label use are harder to appeal. If your clinical situation supports a weight-management diagnosis (BMI ≥30, or BMI ≥27 with a comorbidity), the cleanest path is often to switch to Wegovy or Zepbound, which are on-label for weight management. Step therapy rules for Wegovy/Zepbound generally focus on prior weight-loss drug trials (phentermine, Contrave, orlistat, Qsymia) and documented weight-management program participation.
2. You were prescribed Wegovy or Zepbound for cardiovascular risk or sleep apnea
Wegovy has an FDA indication for cardiovascular risk reduction in adults with established cardiovascular disease plus obesity or overweight. Zepbound has an FDA indication for moderate-to-severe obstructive sleep apnea in adults with obesity. Denials under these indications should cite the specific FDA-approved indication — and many initial PAs miss the right ICD-10 codes. This is often a documentation fix, not a true step-therapy problem.
3. You were prescribed Ozempic or Mounjaro for type 2 diabetes
Coverage for T2D-indicated GLP-1s is typically broader than for weight-management GLP-1s. The ADA Standards of Care (2026) recommend GLP-1 receptor agonists with demonstrated cardiovascular benefit as a first- or second-line agent for patients with T2D and established ASCVD, heart failure, or chronic kidney disease — not a last resort. This directly contradicts step therapy protocols that force older, less-effective oral agents first.
4. The Six Exception Grounds
These six grounds appear consistently across Medicare Part D exception rules, state step-therapy reform laws (~30 states), and typical plan documents. You only need one. If two or more fit, file citing all of them — requests are granted faster when the case is overdetermined.
You already tried the required drug — and it didn’t work
The insurer wants pharmacy records, not stories. Pull your pharmacy fill history from your pharmacy’s patient portal. CVS, Walgreens, and most big chains let you download 2+ years of fills in under five minutes.
- Pharmacy fill records
- Prior provider notes mentioning the drug
- Lab results during that period
- Records from a previous insurance plan count — you don’t have to repeat a trial because you switched jobs
The required drug is contraindicated for you
Contraindication means a real clinical reason you shouldn’t take it — allergy, documented intolerance, dangerous drug interaction, or a condition that makes the drug unsafe.
- Phentermine: cardiovascular disease, uncontrolled hypertension, tachycardia, hyperthyroidism, MAOI use
- Contrave: seizure history, uncontrolled hypertension, chronic opioid use, MAOI use
- Qsymia: glaucoma, hyperthyroidism, pregnancy
- Orlistat: chronic malabsorption syndrome, cholestasis
- Metformin: severe kidney disease (eGFR < 30), metabolic acidosis history
- Any GLP-1: personal or family history of medullary thyroid carcinoma or MEN2
What counts: chart documentation of the condition, recent labs, specialist notes.
The required drug is expected to be ineffective
This is where clinical guidelines do the heavy lifting. The ADA Standards of Care (2026) position GLP-1 RAs with demonstrated CV benefit as first- or second-line for T2D patients with established ASCVD — independent of A1C. That directly contradicts step therapy protocols that force older oral agents first.
- ADA Standards of Care 2026, Section 9
- SELECT trial for CV risk population
- STEP-1 (semaglutide) or SURMOUNT-1 (tirzepatide) for weight-management indications
- Documentation of your clinical profile showing the step-one drug is unlikely to produce a meaningful response
You’re already stable on the prescribed GLP-1
The continuity-of-care argument is one of the strongest when documented cleanly. If you’ve been on an FDA-approved GLP-1 and responding, forcing you off it isn’t cost-effective — it’s clinically disruptive.
- Dosing history
- Baseline weight and current weight
- Lab trends (A1c, lipids, blood pressure)
- Side-effect profile showing tolerance
- Prior plan’s coverage records if applicable
If your prior therapy was compounded rather than FDA-approved: the continuity-of-care argument is weaker. Insurers treat a compounded-to-brand transition as a new therapy decision. Your prescriber can still cite Ground 4 but should frame it as “patient has demonstrated tolerance of the mechanism” rather than formal continuation.
Delay or forced switch risks serious or irreversible harm
If making you fail first will cause measurable worsening of your condition, you get the exception. Request expedited review — most plans have a 24-hour urgent timeline for this ground.
- Uncontrolled type 2 diabetes
- Progressive diabetic complications
- Active ASCVD
- Worsening kidney function
- Severe obstructive sleep apnea
- Severe obesity-related comorbidities where delay has clear clinical consequences
What counts: current labs showing worsening trend, specialist notes documenting urgency, imaging or diagnostic results if applicable.
Not in best medical interest (clinical judgment)
Your prescriber — in their documented professional opinion — believes the prescribed GLP-1 is the right medication and the step-one drug is not. This is the catch-all ground.
Ground 6 is rarely the primary basis. Pair it with at least one other ground when filing.
5. Copy-Paste Scripts to Send Your Prescriber Today
Under most commercial/ACA-regulated plans, your prescriber’s office files the exception. Under Medicare Part D, you, your prescriber, or your representative can file — though the prescriber’s supporting statement is still required. The language below gives your doctor exactly what they need to file fast. These are patient-to-prescriber requests, not medical-necessity letters.
Script 1 — Prior trial and failure (Ground 1)
Hi Dr. [Name], my insurance denied coverage of [Wegovy / Zepbound / etc.] due to step therapy — they’re asking me to try [required drug] first. I tried [required drug] from [approximate dates] under my prior plan, at [dose if known]. It did not produce clinically meaningful weight loss [and/or] I experienced [side effect]. Would you file a step therapy exception request on the ground of prior trial and failure? I can pull my pharmacy fill history from [pharmacy name] — just let me know where to upload. Thank you.
Note for prescriber: cite pharmacy fill records. If the trial was older than 24 months, still reference it — most plans don’t require recent failure.
Script 2 — Contraindication (Ground 2)
Hi Dr. [Name], my insurance denied [GLP-1] due to step therapy — they want me to try [required drug] first. I have [condition: cardiovascular disease / uncontrolled hypertension / seizure history / glaucoma / etc.], which I understand makes [required drug] clinically inappropriate for me. Would you file a step therapy exception request citing contraindication? My [specialist notes / recent labs / chart documentation] should support this.
Note for prescriber: cite the specific contraindication from the drug’s prescribing information and attach supporting chart documentation.
Script 3 — Expected ineffectiveness (Ground 3)
Hi Dr. [Name], my insurance denied [GLP-1] and is requiring me to try [required drug] first. Given my [clinical profile — ASCVD / BMI / prior weight-loss history / T2D with CV risk], [required drug] is unlikely to produce adequate response. The ADA Standards of Care (2026) support GLP-1 RAs as first- or second-line for my profile. Could you file a step therapy exception request on the ground of expected ineffectiveness, citing the ADA guidelines?
Note for prescriber: cite ADA Standards of Care, Section 9 (2026). For readers with documented ASCVD, also cite SELECT trial outcomes.
Script 4 — Already stable on FDA-approved GLP-1 (Ground 4)
Hi Dr. [Name], my insurance is requiring step therapy before covering [GLP-1], but I’ve been stable on [FDA-approved GLP-1 under prior plan / samples] since [date]. I’ve lost [X lbs] and my [A1c / BP / etc.] has improved. Forcing a switch to [required drug] would interrupt a regimen that’s working. Could you file a step therapy exception request on the ground of continuity of care, with my current response data as supporting documentation?
Note for prescriber: attach baseline and current weight, dosing history, and any improved lab values. If prior therapy was compounded rather than FDA-approved, adjust framing to “patient has demonstrated tolerance of the semaglutide/tirzepatide mechanism” rather than as formal continuation of an equivalent approved therapy.
Script 5 — Risk of harm from delay (Ground 5)
Hi Dr. [Name], my insurance denied [GLP-1] with a step therapy requirement. Given my [progressing condition: uncontrolled T2D / worsening kidney function / active ASCVD / severe OSA / rapid weight gain], delaying effective treatment while I fail-first on [required drug] risks serious harm. Could you file an expedited step therapy exception request on the ground of risk of irreversible harm from delay, with my current clinical trajectory as documentation?
Note for prescriber: cite current labs showing worsening trend and any specialist recommendations. Request expedited review — most plans have a 24-hour urgent timeline for this ground.
Script 6 — Clinical judgment (Ground 6)
Hi Dr. [Name], my insurance denied [GLP-1] with a step therapy requirement. Based on your clinical assessment of my case, is the prescribed [GLP-1] the appropriate choice over [required drug]? If so, could you file a step therapy exception request on the ground that the step-one drug is not in my best medical interest, along with any additional supporting grounds that apply?
Note for prescriber: Ground 6 is rarely the primary basis — pair with at least one other ground when filing.
6. How to File the Exception — The 5-Step Process
Under most commercial plans, your prescriber’s office files the exception — but you drive the process. Under Medicare Part D, you or your prescriber can file.
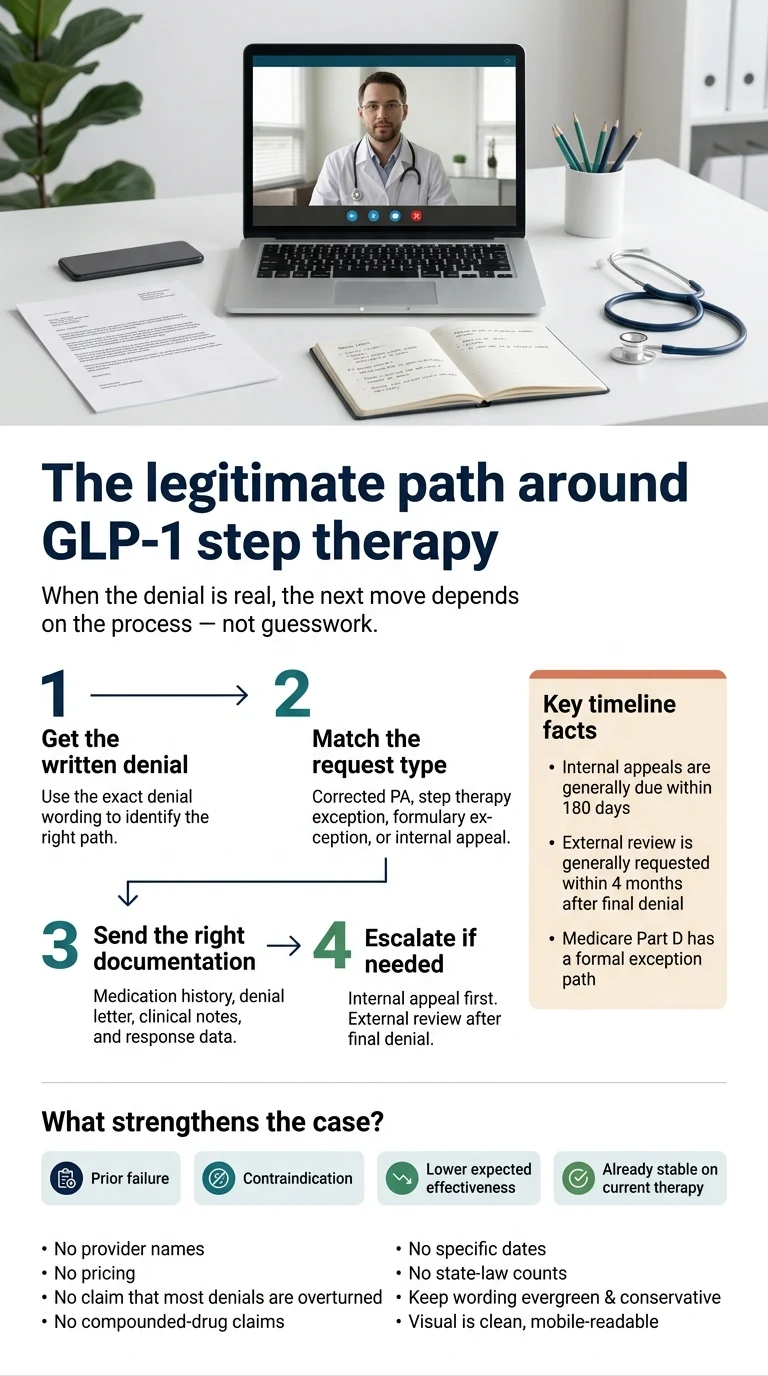
Get the written denial
Call the number on your insurance card. Ask for the written denial letter with the specific reason code. The verbal denial from the pharmacy isn’t enough — the written version contains the exact criteria citation, the appeal deadline, and the specific step-one drug(s) required.
Pull the plan’s actual step therapy criteria
Every plan publishes its own pharmacy-benefit criteria. Search for `[PBM name] [drug name] criteria PDF` and you’ll usually find the exact document. For Wegovy and Zepbound on CVS Caremark, the public criteria require BMI ≥30 (or ≥27 with weight-related comorbidities) and at least six months of documented participation in a comprehensive weight-management program before initial approval.
Identify your ground
Match your situation to one of the six grounds in Section 4. If two fit, file citing both.
Send your prescriber the script (or file yourself on Medicare Part D)
Patient portals process messages faster than phone tag. Paste the right script, fill in the bracketed pieces, and add any supporting documentation. On Medicare Part D, you can file the exception request yourself using your plan’s coverage determination form.
Track the response clock
Under most state step-therapy reform laws, standard exception requests get a response within 72 hours. Urgent requests (where delay risks harm) get a response within 24 hours. Medicare Part D uses the same 72-hour / 24-hour timeline. Self-funded ERISA employer plans don’t follow state-law timelines.
7. Timelines: Exception, Internal Appeal, External Review (By Plan Type)
The timeline depends entirely on your plan type. Mark these on your calendar the day the denial arrives. The most common reason appeals fail isn’t weak evidence — it’s missed deadlines.
| Stage | ACA-regulated / Marketplace / fully-insured employer | Medicare Part D | Self-funded ERISA employer |
|---|---|---|---|
| Step therapy exception — standard | 72 hours (most state-regulated plans) | 72 hours (Medicare.gov) | Plan-defined; varies |
| Step therapy exception — urgent | 24 hours (most state-regulated plans) | 24 hours | Plan-defined; commonly 72 hours |
| Internal appeal — filing window | Up to 180 days from denial (HealthCare.gov) | 60 days to request a redetermination after denial | 180 days from denial |
| Internal appeal — decision window | 30 days for pre-service; 60 days for services received | 7 days standard, 72 hours expedited | Single-level: up to 30 days pre-service. Two-level: up to 15 days per level per 29 CFR 2560.503-1 |
| Internal appeal — urgent | 72 hours | 72 hours | 72 hours |
| External review — filing window | Generally 4 months after final internal denial (HealthCare.gov) | 60 days for Medicare Part D | Varies by plan document |
8. Self-Funded ERISA Employer Plans: The Problem Nobody Explains Clearly
Self-funded employer plans cover roughly 65% of U.S. covered workers. Under federal ERISA preemption, these plans are not subject to state step-therapy reform laws — meaning your state’s 72-hour response rule, your state’s exception grounds list, and most state-level patient protections do not apply. You still have appeal rights under federal rules, but the playbook is different.
How to tell if your plan is self-funded (2-minute test)
- Check your Summary Plan Description or Benefits Handbook. Look for “self-funded,” “self-insured,” “ASO” (Administrative Services Only), or “funded by [Employer Name].”
- Check your insurance card. If it says “Administered by [Aetna/BCBS/UHC] for [Your Employer],” that’s usually self-funded.
- Ask HR directly: “Is our medical plan self-funded or fully-insured?”
What you DO have on a self-funded plan
- Federal ERISA appeal rights with written claims and appeals procedure
- A plan-defined exception process (the six grounds show up in most plan documents)
- HR / benefits team leverage — employers choose their formulary and can grant exceptions
What you DON’T have on a self-funded plan
- State-law 72/24-hour response windows (unless your plan voluntarily follows them)
- State-law exception grounds list
- State-level external review (though ERISA plans must still offer external review under ACA rules)
What to do instead
- Request the plan’s written step-therapy exception procedure and timelines.
- File the exception using whichever of the six grounds fits. The legal framework is different; the clinical argument is the same.
- Track federal appeal timelines strictly (see Section 7).
- Add HR as a parallel lever. HR doesn’t process appeals directly, but can raise formulary issues with the plan administrator.
- The Safe Step Act (S. 2903, introduced September 18, 2025) would apply step-therapy reform to ERISA plans if it passes — but don’t wait on it.
9. What Wegovy and Zepbound Insurers Actually Require (CVS Caremark Example)
We’re citing CVS Caremark specifically because its criteria are publicly posted and representative of documentation-heavy PBMs. Other major PBMs (Express Scripts, OptumRx, Prime Therapeutics) have similar structures but meaningfully different specifics. For the most accurate view of your plan’s requirements, search for your specific PBM’s published criteria.
Sources: CVS Caremark Zepbound criteria PDF; CVS Caremark Wegovy criteria PDF (both publicly posted at info.caremark.com). Verified April 17, 2026.
Initial Zepbound / Wegovy criteria (CVS Caremark)
- BMI ≥30, or BMI ≥27 with at least one weight-related comorbidity (T2D, hypertension, dyslipidemia, OSA, cardiovascular disease)
- Documented participation in a comprehensive weight-management program including dietary counseling, increased physical activity, and behavior modification — typically at least six months before initial therapy
- Follow-up documentation during the six-month period
- Prescriber attestation regarding ongoing behavioral components
Continuation criteria (CVS Caremark)
- At least three months at a stable maintenance dose
- At least 5% weight loss from baseline, or maintained weight loss on continuation
- Prescriber documentation of ongoing behavioral support
| If your denial says | Don’t do this | Do this instead |
|---|---|---|
| Need documentation of weight-management participation | File an appeal arguing medical necessity | Gather dated records of participation and resubmit the PA with documentation |
| Not meeting continuation criteria | Start over from scratch | Submit current weight data, dosing history, and response metrics as a supplement |
| Step therapy required with no documentation ask | Don’t worry about the program | File the exception citing one of the six grounds |
10. If Your Exception Is Denied: Appeals, Peer-to-Peer, External Review
A denied exception is not the end. After a denial, your escalation path is: (1) peer-to-peer review if available, (2) internal appeal with expanded documentation, (3) external review.
Level 1 — Peer-to-peer review (when available)
Peer-to-peer review is underused and high-leverage: your prescriber speaks directly to the insurer’s medical director. Approval can be immediate. Not universal — availability varies by plan and PBM.
Patient’s job before a peer-to-peer:
- The specific denial reason
- Which of the six grounds you’re claiming
- The clinical evidence (ADA Standards of Care citation, lab trends, response data)
- A one-line “ask” — what decision you want
Level 2 — Internal appeal
Under ACA rules, you have up to 180 days from the original denial date to file. The appeal should include:
- A copy of the denial letter
- A letter of medical necessity from your prescriber (a full clinical narrative, not just the exception request)
- All supporting documentation (labs, chart notes, pharmacy history, guideline citations)
- A specific ask: approve the prescribed drug, citing which ground applies
Level 3 — External review
After a final internal denial, you can request an external review by an independent reviewer. Under federal rules, you generally have four months from the final internal denial on ACA-regulated plans. The insurer must accept the external reviewer’s decision.
External review is particularly effective when the insurer’s criteria seem inconsistent with clinical guidelines, documentation is strong but the insurer repeatedly denies, or your case involves risk-of-harm arguments.
| Action | Deadline |
|---|---|
| Request peer-to-peer (if available) | As soon as exception is denied |
| File internal appeal | Within 180 days of denial |
| Request external review | Within 4 months of final internal denial |
| Expedited review (urgent) | Available at any stage if delay risks harm |
11. When to Stop Fighting Insurance and Switch Strategies
Not every denial is winnable. Spotting that fast is the most valuable thing we can give you, because the alternative is 60 days on a fight that was always going to lose.
Stop signal 1: Blanket exclusion
If your denial letter says “plan does not cover anti-obesity medications” or “weight-loss drugs excluded from formulary,” you’re in a benefit-design fight, not a step therapy fight. The only way to win is to change the benefit design — which means HR advocacy or switching plans during open enrollment.
Stop signal 2: Self-funded plan that declined the exception
If you’re on a self-funded ERISA plan and the plan administrator has already denied an exception for this drug class, your employer made a deliberate coverage choice. HR is your best remaining lever, and it’s slow.
Stop signal 3: No supporting documentation
If you’ve never tried a step-one drug, nothing is contraindicated, your clinical profile doesn’t support “expected ineffectiveness,” you’re not currently on a GLP-1, and nothing is urgently progressing — you may not have a case that fits the six grounds. Completing the six-month program documentation may be faster than fighting an appeal you’re likely to lose.
Stop signal 4: Timeline mismatch
If your motivation window is this month and your appeal cycle will run 60–90 days, you have a real choice: start self-pay now and run the appeal in parallel (many readers do this), or accept that insurance won’t be your path this cycle.
12. The Parallel Self-Pay Path — If You Need to Start This Week
For readers whose insurance path is blocked or whose timeline is too tight, self-pay through a licensed telehealth provider is often more accessible than expected. One compliance note: in March 2026, the FDA issued warning letters to 30 telehealth companies over misleading marketing of compounded GLP-1s. The providers below focus on FDA-approved options.
| Provider | Membership / program fee | Medications carried | Insurance help | HSA/FSA |
|---|---|---|---|---|
| Embody | No membership fee; cash-pay, low first month | Compounded semaglutide/tirzepatide injections + needle-free GLP-1 gum | Self-pay focused | ✅ Eligible |
| Ro | $39 first month, then $149/month — or as low as $74/month with annual plan prepaid. Medication priced separately. | Zepbound, Foundayo, Wegovy pen, Wegovy pill | Insurance concierge verifies benefits, handles PA paperwork, assists with appeals | Some medications eligible with prescription |
| Sesame Care | $59/month annual membership. Medication priced separately. | FDA-approved GLP-1 access | Self-pay focused | ✅ Eligible |
Embody
Best for: low-cost cash-pay, needle-free gum, HSA/FSAWhen the step-therapy fight isn’t worth it, Embody is the low-friction cash-pay route — no insurance required and no separate membership fee, so your dollars go to medication. Fast online intake (~5 min); if a provider approves you, Embody ships compounded semaglutide or tirzepatide as a weekly injection or a needle-free GLP-1 gum. Pricing starts low (from $99 first month for semaglutide injection, then $299–$449/month by medication and form) and it’s advertised as HSA/FSA eligible (confirm with your plan).
Check Embody Eligibility → (sponsored affiliate link, opens in a new tab)From $99 first month (sema injection) · No separate membership fee · HSA/FSA eligible (confirm with plan) · Check availability in your state during intake
Embody’s shipped compounded GLP-1 options are not FDA-approved finished drugs. A licensed provider determines whether treatment is medically appropriate. Prices, pharmacy availability, shipping timelines, and state eligibility can change and should be confirmed during intake. Last verified June 11, 2026.
Ro
Best for: PA concierge + cash-pay fallbackRo’s insurance concierge handles the prior authorization fight with you. They verify benefits, handle PA paperwork, and assist with appeals — literally what this page is about. For readers who want someone to handle the insurer call and have a cash-pay fallback ready, Ro is the fit.
Honest disclosure: Ro’s monthly membership ($149/month, or $74/month annual) sits on top of separately-priced medication, whereas Embody bundles its cash-pay program with no separate membership fee. Ro cannot coordinate GLP-1 coverage for government insurance plans (Medicare, Medicaid, VA/TRICARE). If you’re on a government plan, a cash-pay route like Embody or Sesame Care is the better fit. Ro pays The RX Index a smaller referral than several other providers on our full list — we’re featuring them because the concierge layer is genuinely relevant here.
Current Ro pricing: $39 first month, then as low as $74/month with annual plan paid upfront or $149/month. Medication priced separately. Wegovy pill from $149, Foundayo from $149, Zepbound KwikPen from $299, Wegovy pen from $199 (first month). Verify current pricing at checkout.
See if Ro’s concierge path fits you → (sponsored affiliate link, opens in a new tab)$39 to start · Commercial insurance only for concierge · Verified April 17, 2026
Sesame Care
Best for: FDA-approved only, oral FoundayoThe cleanest FDA-approved-only lane, including oral Wegovy and Foundayo. $59/month annual membership, medication priced separately. Strong for readers who specifically want branded-only care.
Compare FDA-approved options on Sesame Care → (sponsored affiliate link, opens in a new tab)13. Frequently Asked Questions
Can you legally bypass step therapy for GLP-1?
Yes — through the step therapy exception process your plan offers. You cannot bypass it by falsifying a failed trial or misrepresenting contraindications. The exception process uses the six grounds covered on this page. Exact rules vary by plan type — Medicare Part D, ACA/commercial, state-regulated, and self-funded ERISA plans each operate differently.
Who can file the step therapy exception request?
Under most commercial/ACA-regulated plans, the prescriber’s office files the exception. Under Medicare Part D, you, your prescriber, or your representative can request an exception — though the prescriber’s supporting statement is still required.
What’s the difference between step therapy, prior authorization, and a formulary exception?
Step therapy requires trying a cheaper drug first. Prior authorization requires clinical documentation before approval. Formulary exception requests a drug that isn’t on the plan’s list at all. Each uses a different form and different arguments. Read your denial letter for the exact category.
What if my insurer says I need 3 or 6 months of weight-loss proof?
That’s a documentation requirement, not step therapy. Appealing won’t help — meeting the requirement will. Gather dated records of dietician visits, program participation, follow-up visits, and resubmit the PA with complete documentation. CVS Caremark’s public criteria require at least six months for initial Wegovy/Zepbound approval.
Does being already stable on Wegovy or Zepbound help my exception request?
Yes — significantly. This is Ground 4 (continuity of care). Attach your dosing history, baseline weight, current weight, and any improved lab values. Insurers routinely grant exceptions when forcing a drug switch would interrupt a working regimen.
Do state laws let you skip step therapy?
Roughly 30 states have step therapy reform laws that require insurers to offer an exception process with defined grounds and timelines. State laws apply to state-regulated plans — individual, small-group, and fully-insured employer plans. They generally do not apply to self-funded ERISA employer plans.
What if my employer plan is self-funded?
State step-therapy reform laws don’t apply to self-funded ERISA plans. You still have federal ERISA appeal rights, and most plans have an internal exception process — but the timeline and grounds may be plan-defined. The six exception grounds still apply clinically; the legal framework is different.
How long do GLP-1 appeals take?
Step therapy exception: typically 72 hours (24 hours urgent) under state-regulated and Medicare Part D plans. Internal appeal: up to 30 days for pre-service under ACA rules; varies under ERISA. External review: generally decided within 45 days, 72 hours for urgent. Full cycle worst case on ACA-regulated plans: 60–90 days.
What if my internal appeal is denied?
Request an external review by an independent reviewer. Under ACA rules, you generally have four months from the final internal denial to request external review. External reviewers’ decisions are binding on insurers.
Should I pay cash while I appeal?
Many readers do. The appeal cycle can run 60–90 days, and motivation windows close. If you start self-pay now, keep your pharmacy records — they become Ground 4 evidence (stability on current therapy) if your appeal eventually succeeds.
When is a denial really a plan exclusion instead of step therapy?
Read the denial language. “Plan does not cover anti-obesity medications” or “weight-loss drugs excluded from plan” = exclusion. “Step therapy required” or “must try [specific drug] first” = step therapy. Exclusions require changing the benefit design; step therapy can be appealed.
Can I get Wegovy without trying metformin first?
Usually — if you have a qualifying weight-management indication and metformin is either inappropriate for you or already tried. Metformin is more commonly required as a step-one for diabetes-indicated GLP-1s (Ozempic, Mounjaro) than for weight-management ones (Wegovy, Zepbound). If your denial names metformin and you’re seeking Wegovy for weight loss specifically, the insurer may have mis-applied a diabetes step-therapy rule. That’s fixable.
Does step therapy apply to compounded GLP-1s?
Compounded GLP-1s are not FDA-approved and are typically not covered by commercial insurance, which means step therapy rules usually don’t apply to them specifically. But if you’re switching from compounded to an FDA-approved product and your insurer requires step therapy for the branded drug, the six-ground framework in this guide applies.
Can I use HSA or FSA funds while I’m fighting the exception?
Usually yes — HSA and FSA funds can cover FDA-approved GLP-1s when you have a prescription. IRS Publication 502 treats prescribed drugs as qualified medical expenses, and weight-loss programs can qualify when treating a specific disease diagnosed by a physician. Some administrators may require a Letter of Medical Necessity for weight-loss-indicated use.
How much does a GLP-1 cost without insurance if the exception fails?
Self-pay cost depends on the drug and provider. Ro’s current cash-pay options include Wegovy pill from $149 first month, Foundayo from $149, Zepbound KwikPen from $299, and Wegovy pen from $199 (medication priced separately from membership). Manufacturer direct-pay programs (LillyDirect, NovoCare Pharmacy) and direct-to-consumer programs like TrumpRx are additional options. Verify all pricing directly at checkout.
What if I’m prescribed a GLP-1 for a non-weight-loss indication?
Coverage is generally easier for FDA-approved indications other than weight loss — type 2 diabetes (Ozempic, Mounjaro), cardiovascular risk reduction (Wegovy’s CV indication), obstructive sleep apnea (Zepbound’s OSA indication), or chronic kidney disease. Make sure the PA submission uses the correct diagnosis code for your indication.
14. What We Actually Verified
Every commercial and regulatory claim on this page was checked against a primary source on April 17, 2026.
| Claim | Verified | Source |
|---|---|---|
| Internal appeals generally must be filed within 180 days (ACA plans) | April 17, 2026 | HealthCare.gov — Internal appeals |
| External review generally due within 4 months of final denial (ACA plans) | April 17, 2026 | HealthCare.gov — External review |
| Medicare Part D step therapy exception: 72h standard / 24h urgent | April 17, 2026 | Medicare.gov — Plan rules |
| Medicare Part D: patient, prescriber, or representative can file an exception | April 17, 2026 | Medicare.gov — Plan rules |
| CVS Caremark public Wegovy/Zepbound criteria: ~6 months weight-management participation for initial approval | April 17, 2026 | CVS Caremark Zepbound PDF; CVS Caremark Wegovy PDF (info.caremark.com) |
| CVS Caremark continuation criteria: 3 months + 5% baseline weight loss or maintained response | April 17, 2026 | CVS Caremark public criteria (above) |
| Roughly 65% of covered workers on self-funded employer plans | April 17, 2026 | DOL EBSA guidance; NCSL referenced data |
| State step therapy reform laws generally don’t apply to self-funded ERISA plans | April 17, 2026 | ERISA preemption framework; Triage Cancer state law chart |
| ADA Standards of Care (2026): GLP-1 RAs recommended as first- or second-line for T2D with ASCVD | April 17, 2026 | Diabetes Care 49 Supplement_1, S183 (2026) |
| FDA warning letters to 30 telehealth companies (March 2026) over compounded GLP-1 marketing | April 17, 2026 | FDA press announcement |
| Safe Step Act: S. 2903, 119th Congress, introduced September 18, 2025 | April 17, 2026 | GovInfo S. 2903 |
| ERISA claims rules: single-level appeal up to 30 days pre-service | April 17, 2026 | 29 CFR 2560.503-1 |
| Ro pricing: $39 first month, then $149/month or as low as $74/month annual prepay | April 17, 2026 | Ro.co/weight-loss; Ro pricing page — re-verified monthly |
| Embody: compounded semaglutide/tirzepatide injections + needle-free GLP-1 gum, cash-pay, HSA/FSA eligible (confirm with plan) | June 11, 2026 | Embody provider site — re-verified monthly |
| Sesame Care: $59/month annual membership, medication separate | April 17, 2026 | Sesame Care provider site — re-verified monthly |
Your action plan (four steps)
- Pull your denial letter. Match the exact language to the triage table in Section 2.
- Identify your ground. One of the six in Section 4 likely fits.
- Send your prescriber the matching script (Section 5). Ask specifically for a step therapy exception request — use those exact words. On Medicare Part D, you can also file yourself using your plan’s coverage determination form.
- Track the response clock. 72 hours standard in state-regulated and Medicare Part D plans; 24 hours urgent. Self-funded ERISA plan: check your Summary Plan Description.
If the exception is denied: up to 180 days to file an internal appeal on ACA-regulated plans. After that fails: four months for external review. If your plan excludes weight-loss drugs entirely: move to self-pay or work with HR.
Not sure which GLP-1 path is right for you?
We’ll map your insurance situation, your state, your denial language, and your timeline to the right next move in 60 seconds.
Start the GLP-1 Path Matcher →Related guides on The RX Index
Written by: The RX Index Editorial Team • Last verified: April 17, 2026 • Next scheduled recheck: July 2026
To produce this guide, we reviewed federal appeal rules (HealthCare.gov, CMS, 29 CFR 2560.503-1), Medicare Part D exception rules, state step-therapy reform laws (Triage Cancer state-law chart), publicly-posted PBM criteria (CVS Caremark Wegovy and Zepbound documents), the American Diabetes Association Standards of Care 2026, and provider-site pricing pages.
When readers click affiliate links to Embody, Ro, Sesame Care, or other providers from this page, The RX Index may receive a referral at no additional cost to you. We disclose material conflicts in the content itself. We do not accept payment to change editorial rankings or suppress negative information about any provider.
This page provides general information about insurance step therapy exceptions. It is not medical advice, legal advice, or insurance advice. For medical decisions, consult your healthcare provider. For plan-specific coverage questions, contact your insurer directly.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup