Denied Wegovy, Zepbound, Ozempic, or Mounjaro? Start here.
How to Appeal a GLP-1 Denial (and Know When an Appeal Won't Work)
Your GLP-1 got denied. Here’s what matters right now: how to appeal a GLP-1 denial depends entirely on why you were denied. Some denials flip with a single phone call. Others require a formal appeal with clinical evidence. And some — the true plan exclusions — are genuinely hard to overturn.
Disclosure: Some links on this page are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you.
Here’s what this guide will help you do:
- Decode your denial in 60 seconds so you know which type you're dealing with
- Follow the exact appeal steps for your specific denial reason
- Know when an appeal isn't your best move — and what to do instead
- Start treatment without insurance if you can't afford to wait 4–12 weeks
Most people who get denied never appeal. KFF found that consumers appealed roughly 1% of denied in-network claims in HealthCare.gov marketplace plans in 2023. In Medicare Advantage, only 11.5% of denied prior authorization requests were appealed in 2024 — but 80.7% of those appeals were wholly or partially decided in the patient’s favor.
Insurance companies are counting on you giving up. Don’t.
What Does Your GLP-1 Denial Actually Mean?
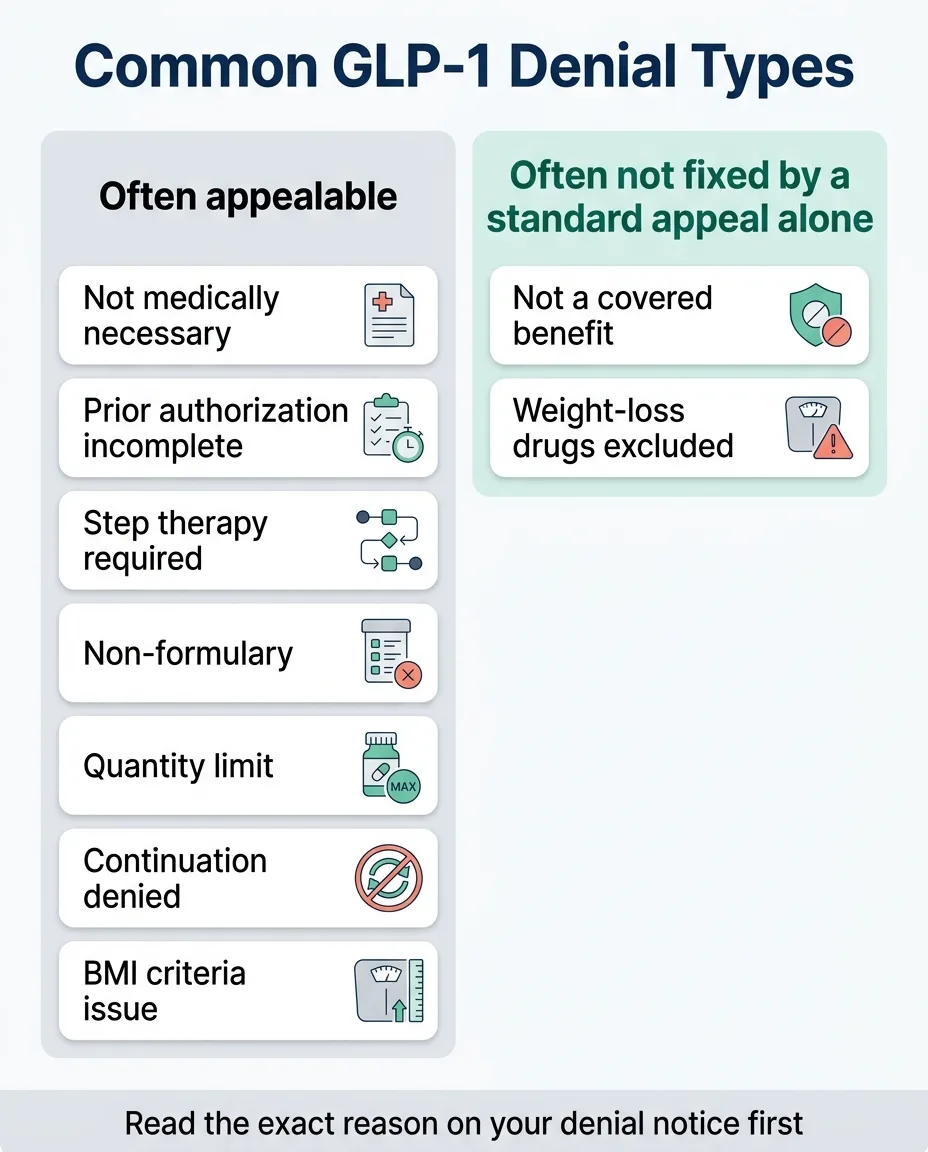
Before you write a single word of an appeal letter, you need to know what you’re fighting. Pull out your denial notice and find the specific reason. The language they use tells you everything about your chances and strategy.
| What Your Denial Says | What It Really Means | Can You Win? | Best Move |
|---|---|---|---|
| Not medically necessary | Insurer says submitted evidence doesn't prove you need this drug | High odds | Get a Letter of Medical Necessity |
| Prior authorization incomplete | Your doctor's office didn't submit the right paperwork | Very high odds — often a paperwork fix | Ask your doctor to resubmit with complete documentation |
| Step therapy required | Insurer wants you to try cheaper drugs first | Moderate odds | Document prior medications tried or get a step therapy exception |
| Non-formulary | This specific medication isn't on your plan's approved list | Moderate odds | Request a formulary exception or ask about covered GLP-1 alternatives |
| Quantity limit exceeded | The dose or quantity isn't covered | Moderate odds | Have your doctor justify the specific dose in writing |
| Continuation/reauthorization denied | You were on it; now they want to stop coverage | Good odds — you have documented results | Show your progress: weight loss, labs, reduced comorbidities |
| BMI does not meet criteria | Your BMI is too low because the medication worked | Good odds — but you need your initial BMI | Submit pre-treatment BMI; argue that stopping reverses progress |
| Off-label use | Drug prescribed for an FDA-unapproved use | Low-moderate odds | Ask your doctor about switching to the correctly-indicated drug |
| Not a covered benefit / Weight-loss drugs excluded | Your plan categorically excludes weight-loss medications | Low odds for standard appeal | Verify exclusion, check alternate indications, escalate to HR, or explore non-insurance options |
The critical distinction most guides miss
The first seven rows are utilization management denials — the insurer is gatekeeping, but there’s a door. The last row is a benefit exclusion — there may not be a door at all. Knowing which bucket you’re in changes everything about your next move.
Your Legal Rights (What Insurance Companies Hope You Don’t Know)
Most non-grandfathered private health plans must give you internal appeal and external review rights. (Grandfathered plans — some older plans unchanged since March 2010 — may follow different rules.) If you’re unsure, check your plan documents or call the number on your insurance card.
What the law guarantees for most non-grandfathered plans
- Written explanation. Your insurer must tell you in writing exactly why they denied your claim and what criteria they used.
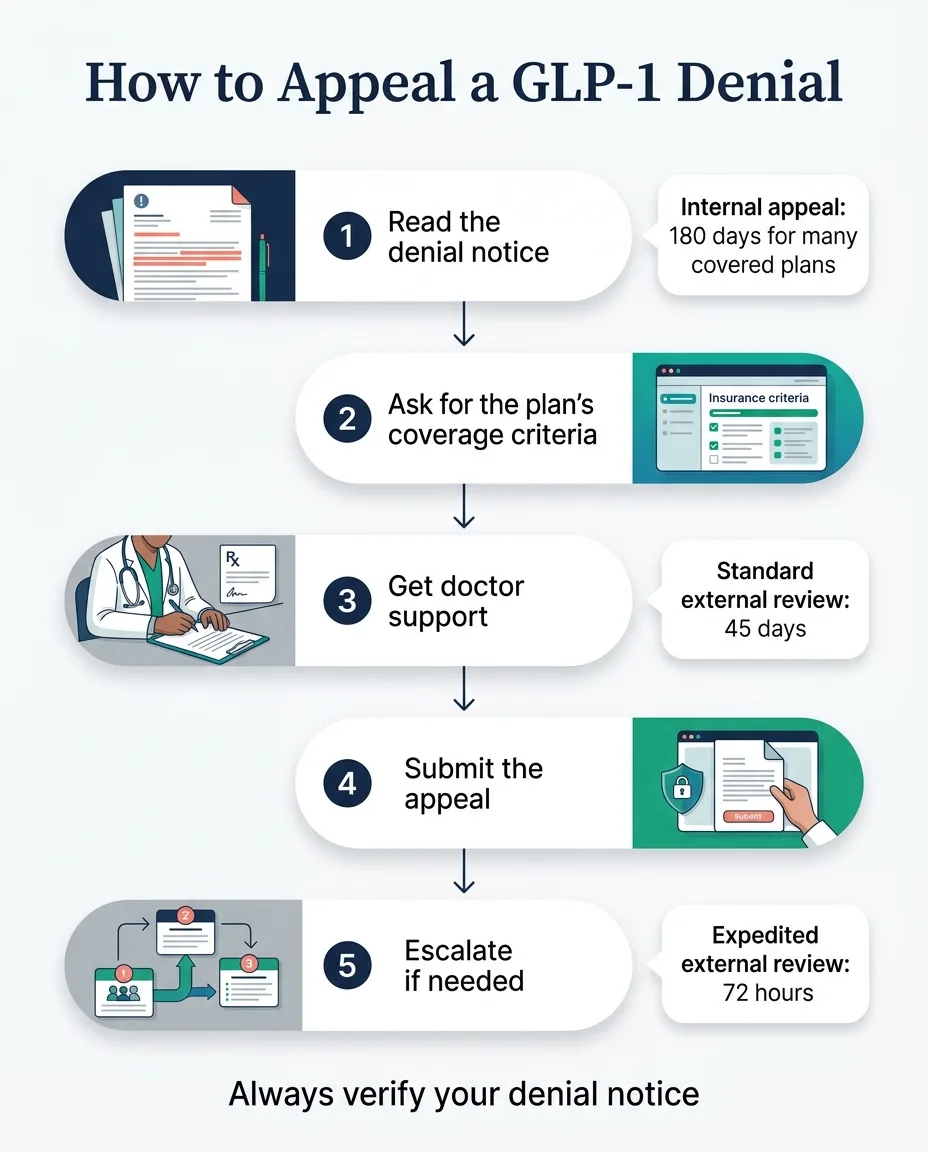
- Internal appeal. You can file at least one formal appeal. HealthCare.gov gives a standard 180-day filing window for covered plans.
- External review. If your internal appeal fails, an independent third-party medical professional reviews your case with no financial ties to your insurer. Standard external reviews take up to 45 days; expedited reviews (when delay creates medical risk) must happen within 72 hours.
- Binding decision. For non-grandfathered plans, the insurer must honor the external reviewer's decision. If the independent reviewer says you should be covered, your insurance company must comply.
Medicare Part D
Start with an exception request or redetermination, then reconsideration (65 days). Standard: 7 days. Expedited: 72 hours.
Medicaid
Your state has its own fair hearing process. Timelines vary, but every state must offer a way to challenge a denial.
Self-Funded Plans
DOL rules apply. The employer — not the insurer — makes coverage decisions. HR escalation can sometimes override denials.
The system is built around the assumption that you’ll give up after the first “no.” The data proves that fighting back works — but only if you actually file.
How to Appeal Your GLP-1 Denial: 7 Steps
These steps work for Wegovy, Zepbound, Ozempic, and Mounjaro denials across commercial insurance, ACA marketplace plans, and (with modifications) Medicare Part D.
Save the Denial Notice and Identify the Exact Reason
This sounds basic, but it’s where most people go wrong. They read the denial, feel defeated, and toss it. Don’t. That notice is your battle plan.
Find and write down:
- The specific denial reason (use the table above to classify it)
- Your appeal deadline — commonly 60–180 days for commercial plans; check the notice itself
- Submission instructions — some require fax, some accept online portal, some want certified mail
- Your claim or prior authorization reference number
- The clinical criteria they used — you may need to call and request it
If the notice is missing the denial reason, appeal instructions, deadline, or the standard used, call the plan and request a complete adverse determination before submitting anything.
Call Your Insurance and Ask for the Specific Coverage Criteria
Before you write anything, call the number on the back of your insurance card and ask:
“Can you tell me the exact clinical criteria your plan uses to approve [your medication name] for [your diagnosis]? I’d like to see the prior authorization criteria document.”
Write down the name of every person you speak with, the date, and the time. This documentation can support your appeal later.
Pro tip that works more often than you’d think
Sometimes the person on the phone will tell you exactly what’s missing. “We needed documentation of a BMI over 30 with a comorbidity, and your doctor only submitted the BMI.” That’s gold. Now you know exactly what to fix.
Get a Letter of Medical Necessity from Your Doctor
This is the single most important document in your appeal. A strong Letter of Medical Necessity (LMN) from your prescribing physician can make or break the outcome.
Your doctor’s letter must include:
- Your diagnosis with specific ICD-10 codes (E66.01, E11, I10, G47.33, E28.2 — all relevant diagnoses)
- Your initial/pre-treatment BMI — not just your current BMI. If the medication worked and your BMI dropped, the initial BMI is what qualifies you.
- Comorbidities with documentation: hypertension, type 2 diabetes, prediabetes, cardiovascular disease, sleep apnea, PCOS, dyslipidemia, NASH/MASH
- Previous weight-loss attempts that failed: diets, exercise programs, behavioral therapy, other medications tried (with dates, duration, and outcomes)
- Why this specific GLP-1 is medically necessary for your specific situation — not generic language
- Relevant clinical guidelines: ADA Standards of Care, AACE Obesity Guidelines, AHA/ACC recommendations
- A direct response to the denial reason — if they said 'not medically necessary,' the letter explains precisely why it is
Ask about a peer-to-peer review
This is a phone call between your prescribing doctor and the insurance company’s medical director. Your doctor can directly explain your clinical situation in real time. Ask your doctor’s office to request one — many patients don’t know this tool exists.
Both Novo Nordisk and Eli Lilly publish sample appeal letter templates on their medical professional sites. Share these with your doctor’s office as a starting framework.
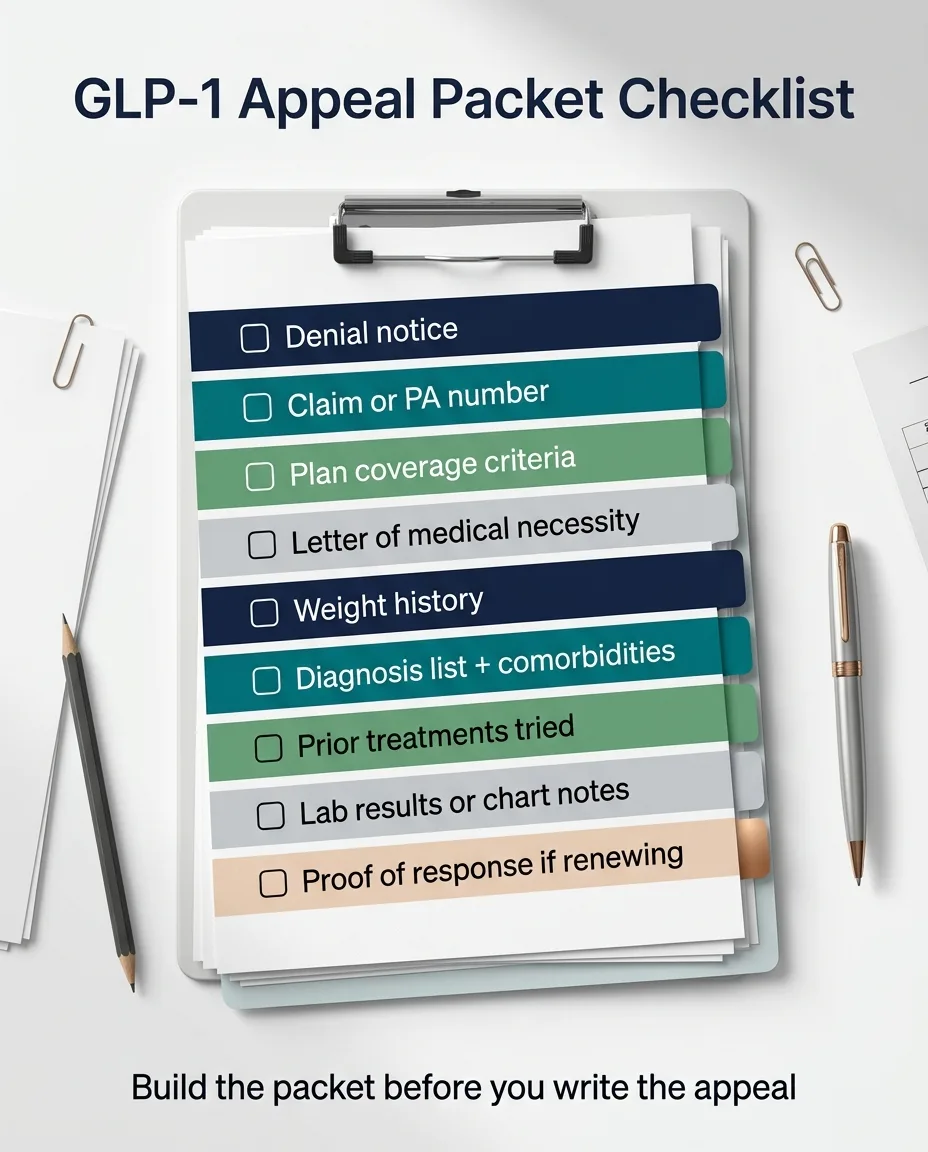
Gather Your Clinical Evidence Package
Your appeal should be an evidence package, not just a letter. Here’s what to include:
For every denial type:
- Copy of the denial notice
- Prior authorization reference number
- Your doctor's Letter of Medical Necessity
- Medical records showing relevant diagnoses
- Lab results (A1C, lipid panel, fasting glucose, liver function)
- BMI documentation — both initial and current
- List of all weight-loss methods previously tried with dates and outcomes
For “step therapy” denials, also include:
- Documentation of every medication previously tried — even under a different insurance plan
- Side effects experienced with chart notes to prove it
- Clinical reasons why the required alternatives are inappropriate for you
- Your state may have step therapy exception laws — check with your state insurance department
For “not medically necessary” denials, also include:
- Clinical guidelines recommending GLP-1s for your conditions (ADA Standards of Care 2025, SELECT trial, AACE guidelines)
- Documentation of obesity-related health complications
- If applicable, evidence of cardiovascular risk that aligns with Wegovy's FDA-approved indication for reducing major adverse cardiovascular events
For continuation/reauthorization denials, also include:
- Progress documentation: pounds lost, BMI reduction, improved labs, reduced medications
- Evidence that stopping treatment poses clinical risk — published data shows patients regain roughly two-thirds of prior weight loss within a year after stopping semaglutide
Write Your Appeal Letter
Keep it professional. Keep it focused. Keep it tied to their specific denial reason.
Structure that works:
- 1Header: Your name, insurance ID, policy number, claim/PA reference number, date
- 2Opening: "I am writing to formally appeal the denial of coverage for [medication], reference number [X], denied on [date] for the stated reason of [quote their exact denial reason]."
- 3Your medical case: Connect your specific health conditions to the medical necessity. Use clinical language. Reference diagnoses by ICD-10 code.
- 4Counter their denial reason directly: Don't write around it — address it head-on. If they said "step therapy," explain why the required alternatives are inappropriate.
- 5Cite clinical guidelines: Reference the ADA Standards of Care, the AACE Guidelines, and relevant clinical trials by name.
- 6List attached evidence: Enumerate every document you're including.
- 7Closing: Professional, firm, requesting reconsideration. Note your right to external review if the internal appeal is denied.
What NOT to put in your letter
- Emotional pleas without clinical backing ("I really need this medication")
- Vague statements ("it's not fair")
- Threats or hostility
Phrases that work with medical reviewers
“medically necessary,” “standard of care,” “clinically indicated,” “consistent with ADA/AACE guidelines,” “documented failure of alternative treatments.”
GLP-1 Appeal Letter Template
Use this fill-in-the-blank framework. The more specific you are, the stronger your case.
[Your Name]
[Your Address]
[Date]
[Insurance Company] Appeals Department
[Address from denial notice]
Re: Appeal of Denial — [Medication Name]
Member ID: [Your ID]
Claim/PA Reference: [Number from denial notice]
Date of Denial: [Date]
Dear Appeals Review Committee,
I am writing to formally appeal the denial of coverage for [medication name and dose], prescribed by [doctor name, credentials] for the treatment of [your diagnosis/diagnoses with ICD-10 codes]. The stated reason for denial was [copy the exact denial reason from your notice].
Medical History and Necessity: I am a [age]-year-old [male/female] patient. My initial BMI was [initial BMI] as of [date], with the following documented comorbidities: [list: e.g., type 2 diabetes (E11.9), hypertension (I10), obstructive sleep apnea (G47.33)]. [If continuation denial: My current BMI is [current BMI], reduced from [initial BMI] while on this medication, demonstrating clinical response.]
Prior Treatment History: I have previously attempted the following treatments without adequate response: [list each medication or program with dates, duration, and outcome/side effects].
Clinical Guidelines Supporting This Treatment: The ADA Standards of Care (2025) recommend GLP-1 receptor agonists for patients with my clinical profile. The AACE Comprehensive Clinical Practice Guidelines recognize GLP-1 medications as first-line pharmacotherapy for obesity. [If applicable: The SELECT trial (New England Journal of Medicine, 2023) demonstrated that semaglutide reduced major adverse cardiovascular events by 20% in patients with established CVD and obesity/overweight.]
Response to Denial Reason: [Address the specific denial reason directly. For “not medically necessary”: explain why it IS necessary. For “step therapy”: document why required alternatives are inappropriate. For “BMI too low”: submit initial BMI and explain that discontinuation will reverse clinical benefit.]
Enclosed Documentation:
1. Copy of denial notice
2. Letter of Medical Necessity from [doctor name]
3. Medical records including BMI history, diagnoses, and lab results
4. [List all additional supporting documents]
I respectfully request that you reconsider this denial based on the medical evidence provided. If this appeal is denied, I will exercise my right to external review.
Sincerely,
[Your Name]
[Phone Number]
[Email]
Want insurance support built into your GLP-1 evaluation?
Ro handles the insurance check, prior authorization support, and prescribing in one workflow — so you’re not navigating this alone.
Check eligibility on RoSubmit and Document Everything
Follow your insurer’s submission instructions exactly.
- If they want a fax, fax it — and keep the transmission confirmation
- If they accept online portal submissions, screenshot every step
- If mailing, use certified mail with return receipt so you have proof of delivery
- Keep copies of everything you send
- Note the date submitted and calculate when the response is due based on your plan's timeline
If the deadline passes with no response, that’s a compliance issue. Contact your state insurance department.
If Denied Again — Don’t Stop
Your first appeal was denied? You still have options.
Level 2: Second internal appeal
Many plans allow a second round. Strengthen your evidence. Address any new reasons they cited.
Level 3: External review
An independent medical professional reviews your case with no financial ties to your insurer. Standard: 45 days. Expedited: 72 hours. For non-grandfathered plans, the insurer must honor the decision.
Level 4: State insurance commissioner
File a complaint with your state's Department of Insurance. They can investigate whether your insurer followed proper procedures.
Level 5: Employer benefits escalation (self-funded plans)
If your plan is self-funded, the employer — not the insurance company — actually makes coverage decisions. Talk to your HR department or benefits administrator.
For Medicare Part D
After an unfavorable redetermination, file for reconsideration within 65 days. If that fails, you can escalate to an Administrative Law Judge hearing for claims over a minimum dollar threshold.
How Long Does a GLP-1 Appeal Actually Take?
Let’s set real expectations:
| Stage | Timeline |
|---|---|
| Read denial + call insurance + gather records | Week 1 |
| Get Letter of Medical Necessity from doctor | Weeks 1–2 |
| Write and submit appeal | Week 2–3 |
| Internal appeal decision | 30 days (72 hours if expedited) |
| Second internal appeal (if needed) | Additional 30 days |
| External review (if needed) | 45 days (72 hours if expedited) |
| Total realistic timeline | 4–12 weeks |
That’s 4–12 weeks of waiting — and if you were already on a GLP-1, that’s 4–12 weeks without your medication. Which brings us to something most guides won’t tell you.
The Hard Truth About Plan Exclusions
If your insurance plan categorically excludes weight-loss medications, a standard appeal is unlikely to succeed.
You’re not fighting a documentation problem or a medical-necessity argument. You’re fighting the plan design itself.
That doesn’t mean you have zero options:
- 1Verify it's really a blanket exclusion. Call and ask: 'Does my plan exclude all anti-obesity medications, or just specific ones? Are GLP-1s covered for any indication?' Sometimes a plan excludes Wegovy for weight loss but covers Ozempic for diabetes.
- 2Check for alternate FDA-approved indications. Wegovy was FDA-approved in March 2024 to reduce major adverse cardiovascular events in adults with established cardiovascular disease and obesity or overweight. A prescription framed around cardiovascular risk reduction may qualify for different coverage.
- 3Zepbound has an OSA indication. Zepbound (tirzepatide) was approved for moderate-to-severe obstructive sleep apnea in adults with obesity. If you have a documented sleep apnea diagnosis, this changes the appeal calculus entirely.
- 4Escalate to HR if your plan is self-funded. Many large employer plans are self-funded, meaning your employer decides what's covered — not the insurance company. HR or benefits teams can sometimes add GLP-1 coverage or make exceptions.
- 5Plan for open enrollment. If the exclusion is ironclad, switching to a plan that does cover GLP-1s during open enrollment (typically November–January) may be your best medium-term strategy.
What If You Don’t Want to Wait?
Many patients do both: file the appeal AND start treatment through a cash-pay provider. If the appeal succeeds, they switch to insurance coverage. If it doesn’t, they’re already in treatment and haven’t lost months of progress.
This path makes sense if any of these fit your situation:
- Your plan excludes weight-loss medications entirely — appeal odds are low
- You were already on a GLP-1 and lost coverage — every week risks losing your progress
- You've been denied two or more times — the appeal process has exhausted your time
- You have a high-deductible plan — even if approved, cash-pay may actually cost less
Provider We Recommend: Ro
Ro offers a free insurance checker and an insurance concierge that handles coverage checks and prior authorization paperwork. If your insurance covers GLP-1s, they’ll work with your plan. If it doesn’t, you have a clear cash-pay path with FDA-approved options — same evaluation, same clinicians, no additional hoops.
Ro’s cash-pay options start at $149/month for certain medications, with a separate Ro Body membership fee. Verify the total monthly cost and specific medication during your intake evaluation.
Check your insurance coverage and GLP-1 eligibility
Free insurance check, FDA-approved medications, clinical evaluation within 48 hours.
Check eligibility on RoBudget is the priority? MEDVi offers compounded semaglutide starting at $179/month, no insurance needed. Note: compounded GLP-1 medications are not FDA-approved. Go in with your eyes open.
See pricing on MEDViHow to Write the Appeal for Each Denial Type
Each denial reason requires a different strategy, different evidence, and different framing. Find yours.
How to Appeal a “Not Medically Necessary” Denial
Your argument
“This medication IS medically necessary based on my documented conditions, and current clinical guidelines from the ADA and AACE recommend it as standard-of-care treatment.”
Your strongest evidence:
- BMI ≥30 (or ≥27 with comorbidity) with supporting documentation
- List of comorbidities: type 2 diabetes, cardiovascular disease, hypertension, sleep apnea, dyslipidemia, PCOS, NASH/MASH
- Failed prior weight-loss attempts with dates and details
- ADA Standards of Care (updated annually) and AACE Comprehensive Clinical Practice Guidelines
- The SELECT Trial (NEJM) — semaglutide reduced major adverse cardiovascular events by 20% in patients with overweight/obesity and established CVD
- If applicable: your doctor's direct rebuttal of the insurer's criteria
Key move: Have your doctor request a peer-to-peer review — a direct phone call with the insurer’s medical director.
How to Appeal a Step Therapy (“Fail First”) Denial
Your argument
“I have already tried the required alternative medications and they were either ineffective, caused adverse effects, or are medically inappropriate for my condition.”
- Documentation of every prior medication tried — including under previous insurance plans
- Chart notes documenting side effects, allergic reactions, or lack of efficacy
- If required alternatives are contraindicated for you, document that clearly
- Check if your state has step therapy exception laws at your state insurance department's website
Key move: If you genuinely haven’t tried the required alternatives, ask your doctor whether a documented short trial showing inadequate response might satisfy the requirement. Medicare Part D also allows exception requests to step therapy with a prescriber supporting statement.
How to Appeal a Non-Formulary Denial
Your argument
“I’m requesting a formulary exception because the formulary alternatives are not appropriate for my medical situation.”
- Clinical rationale for why THIS specific medication (vs. a covered GLP-1) is necessary
- If already on the medication and responding well, document that switching creates clinical risk
- Your doctor's letter explaining why the formulary alternatives won't work
Alternative: Ask your doctor and pharmacist which GLP-1 IS on your plan’s formulary. Sometimes switching to a covered GLP-1 is the path of least resistance.
How to Appeal a Continuation or Reauthorization Denial
Your argument
“Discontinuing this medication will reverse my documented medical progress and create clinical risk.”
- Weight loss achieved (pounds and percentage)
- Improved lab results (A1C reduction, lipid improvement, liver function)
- Comorbidities that improved or resolved while on treatment
- Your initial BMI — not your current BMI. This is critical. If the medication worked and your BMI dropped, the insurer may argue you no longer qualify. Your counter: you only meet that lower threshold because the medication is working.
- Published STEP 1 extension trial data — patients regained roughly two-thirds of prior weight loss within a year after stopping semaglutide
How to Appeal When Your BMI Is “Too Low” Because the Medication Worked
One of the most frustrating and most common reauthorization scenarios: You started at BMI 34. The medication worked. Now your BMI is 29. Your insurer says you no longer meet the criteria.
The counter-argument:
- 1Submit your initial/pre-treatment BMI, not your current BMI — this is the qualifying metric
- 2Cite the STEP 1 extension data — patients regain the majority of lost weight within a year of stopping
- 3Argue that ongoing treatment is necessary to maintain medical benefit — continuation of a working therapy, not a new request
- 4Have your doctor frame the letter around preventing clinical deterioration, not weight loss
As one patient put it on r/WegovyWeightLoss: “It needs your INITIAL BMI not your CURRENT BMI.” This single piece of advice has saved countless reauthorization appeals.
How to Handle Off-Label Use Denials (Ozempic or Mounjaro for Weight Loss)
Ozempic is FDA-approved for type 2 diabetes. Mounjaro is FDA-approved for type 2 diabetes. If your doctor prescribed either for weight loss in someone without T2D, the insurer’s denial may be technically valid.
If you have type 2 diabetes
Make sure the prescription reflects the diabetes indication. Sometimes the denial is a coding issue — submitted with a weight-loss diagnosis when a diabetes diagnosis would have been approved.
If you don’t have type 2 diabetes
Ask your doctor about Wegovy (semaglutide, FDA-approved for weight loss) or Zepbound (tirzepatide, FDA-approved for weight loss). Same active ingredients, correct FDA-approved indication for your use case.
How Are Wegovy, Zepbound, Ozempic, and Mounjaro Denials Different?
The appeal landscape varies by medication because each has different FDA-approved uses — and insurers care deeply about this distinction.
Wegovy (semaglutide) Denial Appeal
FDA-approved indications:
- Chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related comorbidity
- Reducing risk of major adverse cardiovascular events in adults with established cardiovascular disease and obesity/overweight (approved March 2024)
- Pediatric use (ages 12+) for obesity
Appeal leverage
The cardiovascular indication is powerful. If you have documented heart disease, peripheral artery disease, or prior stroke — reframing the prescription around cardiovascular risk reduction can change the outcome entirely. This is using the drug for an FDA-approved purpose.
Zepbound (tirzepatide) Denial Appeal
FDA-approved indications:
- Chronic weight management in adults with obesity or overweight + comorbidity
- Moderate-to-severe obstructive sleep apnea (OSA) in adults with obesity
Appeal leverage
The OSA indication is a significant differentiator. If you have documented sleep apnea (typically confirmed by a sleep study), some insurers who exclude weight-loss drugs still cover Zepbound for OSA. Note: CVS Caremark excluded Zepbound from its formulary as of mid-2025 — ask about Wegovy as an alternative if your PBM is CVS Caremark.
Ozempic (semaglutide) Denial Appeal
FDA-approved indications:
- Type 2 diabetes (glycemic control)
- Reducing risk of major adverse cardiovascular events in T2D patients with established CVD
Appeal leverage
If denied for weight-loss use, your strongest move may be switching to Wegovy (same active ingredient, FDA-approved for weight management). If denied for diabetes: appeal with your A1C levels, diabetes management history, and documentation that alternatives were tried or are inappropriate.
Mounjaro (tirzepatide) Denial Appeal
FDA-approved indications:
- Type 2 diabetes (glycemic control)
Appeal leverage
If denied for weight-loss use, ask your doctor about Zepbound (same active ingredient, approved for weight management). If denied for diabetes: appeal with diabetes documentation, prior medication history, and A1C levels.
Why diagnosis framing matters more than drug popularity
The drug/diagnosis pairing is often more important than the quality of your appeal letter. A perfectly written appeal for Ozempic for weight loss will likely fail because the FDA indication doesn’t match. Work with your doctor to match the right medication to your documented, FDA-approved indication.
The Clinical Evidence That Wins GLP-1 Appeals
When your appeal letter says “clinical guidelines recommend this treatment,” the medical reviewer needs to see which guidelines and which evidence. Here’s the ammunition that carries the most weight — organized so you can hand this list directly to your doctor.
ADA Standards of Care (2025)
The American Diabetes Association recommends GLP-1 receptor agonists as preferred options for patients with type 2 diabetes who have established cardiovascular disease, and as effective options for weight management in patients with obesity. Gold standard for diabetes-related denials.
AACE Comprehensive Clinical Practice Guidelines for Obesity
The American Association of Clinical Endocrinology recognizes GLP-1 medications as first-line pharmacotherapy for obesity. Particularly powerful for 'not medically necessary' denials related to weight management.
The SELECT Trial (NEJM, 2023)
This landmark trial demonstrated that semaglutide reduced major adverse cardiovascular events by 20% in patients with overweight or obesity and established cardiovascular disease — without requiring diabetes. If you have cardiovascular disease, the SELECT trial reframes a weight-loss denial as cardiovascular prevention.
STEP Trials (Wegovy/semaglutide)
Demonstrated 15–17% mean body weight loss. The STEP 1 extension showed that patients regained approximately two-thirds of prior weight loss within a year of stopping — powerful evidence for continuation-of-therapy appeals.
SURMOUNT Trials (Zepbound/tirzepatide)
Demonstrated over 20% mean body weight loss. The SURMOUNT-OSA trial specifically showed significant improvement in obstructive sleep apnea severity — powerful evidence for Zepbound OSA-related appeals.
AHA/ACC Guidelines
The American Heart Association and American College of Cardiology include GLP-1 medications in their guidelines for managing patients with cardiovascular disease, recognizing their ability to reduce major adverse cardiovascular events.
How to cite these in your letter
Don’t just name-drop. Write: “The ADA Standards of Care 2025 recommend GLP-1 receptor agonists as preferred treatment for patients with my clinical profile (type 2 diabetes with established cardiovascular disease). The SELECT trial, published in the New England Journal of Medicine, demonstrated a 20% reduction in major adverse cardiovascular events with semaglutide in this population.” Specific, cited, and directly tied to your situation — that’s what moves a medical reviewer.
Not sure which medication path fits your situation?
Ro evaluates your complete medical picture — conditions, medications, and insurance — to recommend the right GLP-1 for you.
See which GLP-1 you qualify for on RoWhat If Your Doctor Won’t Help With the Appeal?
It happens more than it should. Some doctors are too busy, unfamiliar with the appeal process, or simply don’t prioritize insurance fights.
What you can do yourself:
- You have the right to file an appeal yourself — HealthCare.gov confirms the patient or authorized representative can file
- Request copies of your medical records, BMI history, lab results, and chart notes (they're legally required to provide them)
- Write and submit the patient portion of the appeal yourself using the template above
Minimum to ask your doctor’s office for:
- A brief statement confirming why they prescribed the medication
- Your complete diagnosis list
- Lab results
- The prior authorization documentation they originally submitted
When to find a new prescriber: If your doctor won’t support the appeal at all, it may be time to find a provider who will advocate for you. Telehealth GLP-1 providers like Ro include clinical support and insurance navigation as part of their service — you get a prescriber who actually handles the insurance paperwork.
Need a provider who handles insurance support and prescribing together?
Ro’s clinical team manages evaluation, prescribing, and insurance coordination in one place.
Start your GLP-1 evaluation on RoThe 7 Mistakes That Kill GLP-1 Appeals
These are the most common reasons appeals fail — avoid every one of them.
Appealing before you understand the denial reason
A generic 'please reconsider' letter doesn't work. You need to counter the specific reason they said no.
Submitting your current BMI instead of your initial BMI
If you were on a GLP-1 and it was working, your current BMI may be below the threshold. Always include your pre-treatment BMI. This is the single most missed document in reauthorization appeals.
Writing with emotion instead of evidence
'I need this medication' doesn't move a medical reviewer. 'My BMI was 36.2 at treatment initiation, I have documented type 2 diabetes (E11.9), hypertension (I10), and obstructive sleep apnea (G47.33), and ADA Standards of Care recommend GLP-1 therapy as a first-line option for my clinical profile' — that moves them.
Treating a plan exclusion like a documentation problem
If your plan doesn't cover weight-loss drugs as a benefit category, a stronger appeal letter won't fix that. You need a different strategy: alternate indication, HR escalation, or a non-insurance path.
Using the wrong drug/diagnosis pairing
Appealing an Ozempic-for-weight-loss denial with weight-loss evidence is fighting uphill. The FDA indication doesn't match. Switch to the correctly-indicated drug.
Missing the deadline
Appeal windows are real. Missing yours can permanently forfeit your rights. Mark it on your calendar the day you get the denial notice.
Not requesting expedited review when it matters
If delay creates medical risk — you're running out of medication, your blood sugar is uncontrolled, you have an upcoming surgery — you can request expedited review. Standard expedited: 72 hours.
Your Plan Type Changes Everything
Your appeal rights, deadlines, and escalation options differ depending on what kind of insurance you have.
Employer Plan — Self-Funded
Most large employers (500+ employees) self-fund their health plans, meaning the employer — not the insurance company — decides what's covered. The insurer just administers claims. If your denial is a plan exclusion, escalating to HR or your benefits administrator can sometimes result in exceptions.
Appeal path
Internal appeal → External review → Department of Labor complaint → Employer benefits escalation
Ask HR or check your Summary Plan Description (SPD). Self-funded plans say something like 'benefits are paid from the general assets of the employer.'
Employer Plan — Fully Insured
If your employer buys insurance from a carrier (Aetna, BCBS, Cigna, UnitedHealthcare), the carrier's rules apply. Your employer has less flexibility to override denials.
Appeal path
Internal appeal (180-day window) → External review (45 days standard, 72 hours expedited) → State insurance commissioner
ACA Marketplace / Individual Plan
Full ACA protections apply. You're guaranteed internal appeal and external review rights.
Appeal path
Internal appeal within 180 days → External review → State insurance department
Medicare Part D
Different process entirely. Start with an exception request or coverage determination, then redetermination, then reconsideration by an Independent Review Entity (IRE) within 65 days. Standard decisions: 7 days. Expedited: 72 hours.
Appeal path
Exception request → Redetermination → IRE Reconsideration (65 days) → Administrative Law Judge (if amount threshold met)
Medicare cannot cover drugs prescribed solely for weight loss, but Wegovy's cardiovascular indication and the Medicare GLP-1 Bridge (July–December 2026) create different pathways.
Medicaid
Rules vary by state. As of January 2026, 13 state Medicaid fee-for-service programs cover GLP-1s for obesity treatment — but the landscape is shifting. Contact your state Medicaid office for your specific fair hearing rights.
Appeal path
State Medicaid fair hearing process
Not sure what kind of plan you have?
Call the number on the back of your insurance card and ask: “Is my plan self-funded or fully insured?” This single question changes your entire strategy.
What to Do While You’re Waiting for a Decision
Your appeal is filed. Don’t just wait. Here’s how to use the time productively:
- Ask your doctor about bridge options. Some doctors can provide samples or authorize a short-term supply during your appeal. Some manufacturer programs offer temporary medication access for patients in appeal.
- Check manufacturer savings programs. Novo Nordisk (NovoCare) and Eli Lilly (LillyDirect) offer savings cards and patient assistance programs. For eligible commercially insured patients, these can reduce out-of-pocket costs substantially — sometimes to as little as $25.
- Look at your HSA/FSA. Health Savings Accounts and Flexible Spending Accounts may cover GLP-1 medications even when your insurance doesn't. This can meaningfully offset out-of-pocket costs.
- Consider starting treatment through a cash-pay provider. If your appeal takes 4–12 weeks and your health is at risk, starting now means you don't lose months of progress. If the appeal succeeds later, you switch back to insurance coverage.
- Document everything while you wait. Keep logging weight, blood pressure, and blood sugar. If your health deteriorates during the gap, that documentation becomes powerful evidence for expedited review or escalation.
Don’t lose momentum while you wait
Check your options on Ro — if your insurance comes through, great. If not, you’re already in treatment.
Check eligibility on RoCompare Your Non-Insurance GLP-1 Options
If insurance isn’t in the cards — either because of a plan exclusion, a failed appeal, or a decision not to wait — here’s what the current landscape looks like.
| Feature | Ro | MEDVi |
|---|---|---|
| Medication type | FDA-approved options available | Compounded semaglutide |
| Starting price | Cash-pay from $149/mo for certain medications + Ro Body membership fee | Starting at $179/mo |
| Insurance accepted? | Yes — free insurance checker + concierge | No — cash-pay only |
| Evaluation speed | 24–48 hours | 24–48 hours |
| Licensed clinician? | Yes | Yes |
| Best for | People who want FDA-approved medications and/or insurance support | People prioritizing the lowest monthly cost |
| Cancel anytime? | Yes | Yes |
Pricing last verified March 2026. Verify current total costs directly with each provider, as prices and included services may vary.
Important distinction
FDA-approved GLP-1 medications (Wegovy, Zepbound) have undergone rigorous clinical trials and are manufactured under strict FDA oversight. Compounded GLP-1 medications are prepared by compounding pharmacies and are not FDA-approved. The FDA has raised concerns about certain unapproved compounded GLP-1 products. We include both because both serve real patient needs, but the distinction matters for your decision.
Ro
Free insurance check, FDA-approved GLP-1 options, evaluation within 48 hours.
Check eligibility on RoReal Patients Who Fought Their Denials
When you’re staring at a denial letter, it helps to know you’re not alone — and that persistence pays off.
One patient shared on Claimable’s GLP-1 appeals page: after experiencing multiple denials, they filed one more appeal with a proper Letter of Medical Necessity — and the denial was overturned in less than 12 hours. Their takeaway: “I wish I hadn’t waited so long.”
A common story on Reddit’s r/WegovyWeightLoss: patients get denied for reauthorization because the insurer looks at their current BMI — which dropped because the medication was working — instead of their initial BMI. The fix that keeps coming up: always submit your starting BMI from before treatment began.
The pattern is always the same: identify the specific denial reason, gather the right evidence, address it directly, and keep going. The ones who ultimately succeed are the ones who don’t stop at the first no.
Frequently Asked Questions About GLP-1 Insurance Denials
How long do I have to appeal a GLP-1 denial?
It depends on your plan. HealthCare.gov gives a standard 180-day filing window for ACA marketplace plans. Medicare Part D reconsideration must be filed within 65 days of the denial. Your denial notice will state your specific deadline — do not let it pass.
Can I appeal if my plan excludes weight-loss drugs?
You can try, but standard appeals for benefit exclusions have low success rates. Better strategies include checking for alternate FDA-approved indications (cardiovascular, diabetes, sleep apnea), escalating to your employer's HR team if the plan is self-funded, or planning to switch plans during open enrollment.
Do I need a lawyer to appeal a GLP-1 denial?
No. The vast majority of successful GLP-1 appeals are filed by patients or their doctors without legal representation. Legal help is typically only needed after exhausting all appeal levels if you suspect bad faith or a complex ERISA issue.
What is a Letter of Medical Necessity?
A letter from your prescribing doctor explaining why a GLP-1 medication is medically necessary for your specific health conditions. It should include your diagnoses with ICD-10 codes, BMI (initial and current), comorbidities, prior treatments tried, and clinical guidelines supporting the prescription. It is the single most important document in your appeal.
What is the difference between an appeal and a formulary exception?
An appeal challenges a denial after your claim was processed. A formulary exception requests that your plan cover a drug that is not on its approved list. If your drug is non-formulary, you typically need to file an exception request rather than a standard appeal.
Can I file an appeal myself, or does my doctor have to do it?
Either. HealthCare.gov confirms that the patient or an authorized representative can file appeals. Your doctor can also file on your behalf or submit a supporting statement alongside your patient appeal.
What is a peer-to-peer review?
A phone call between your prescribing doctor and the insurance company's medical director. Your doctor can directly explain your clinical situation and advocate for the prescription in real time. Ask your doctor's office to request one — it is a tool many patients do not know exists.
Does Medicare cover GLP-1s for weight loss?
As of 2026, Medicare Part D generally cannot cover drugs prescribed solely for weight loss. However, Wegovy's cardiovascular indication (approved March 2024) creates a coverage pathway for Medicare beneficiaries with established cardiovascular disease plus obesity or overweight. CMS has also announced the BALANCE Model and the Medicare GLP-1 Bridge (July–December 2026) as separate programs that may expand access.
What if my insurance dropped my GLP-1 coverage mid-treatment?
If your plan changed its formulary or coverage mid-year, you may have transition protections depending on your plan type. Contact your insurer and your state insurance department. Document your treatment history and the clinical risk of abrupt discontinuation, then file an appeal emphasizing continuation of effective therapy.
Can I start a cash-pay GLP-1 while appealing my insurance denial?
Yes — and many patients do. There is no rule preventing you from pursuing both simultaneously. You can start cash-pay treatment to avoid a gap in care, then switch to insurance coverage if the appeal succeeds.
What ICD-10 codes should be on my GLP-1 appeal?
Common codes: E66.01 (morbid obesity), E66.09 (other obesity), E66.9 (obesity unspecified), E11 (type 2 diabetes), I10 (hypertension), E78 (dyslipidemia), G47.33 (obstructive sleep apnea), E28.2 (PCOS), K76.0 (fatty liver disease), I25.10 (atherosclerotic heart disease). Your doctor should include all relevant diagnoses.
How do I find my state's insurance commissioner?
Visit the National Association of Insurance Commissioners (NAIC) website at naic.org for a directory of every state's insurance department and contact information.
How We Verified This Guide
We take accuracy seriously — especially on a topic where wrong information costs people money, time, and health.
Affiliate disclosure: We earn commissions from some providers recommended on this page. This does not influence our appeal guidance — the majority of this guide is about winning your appeal, not buying anything. Our provider recommendations are based on medication type, pricing, insurance coordination, and patient experience. Last verified: March 2026.