Blue Cross Zepbound Coverage · Verified April 16, 2026
Blue Cross Zepbound Prior Authorization: What Actually Gets Approved
Published:
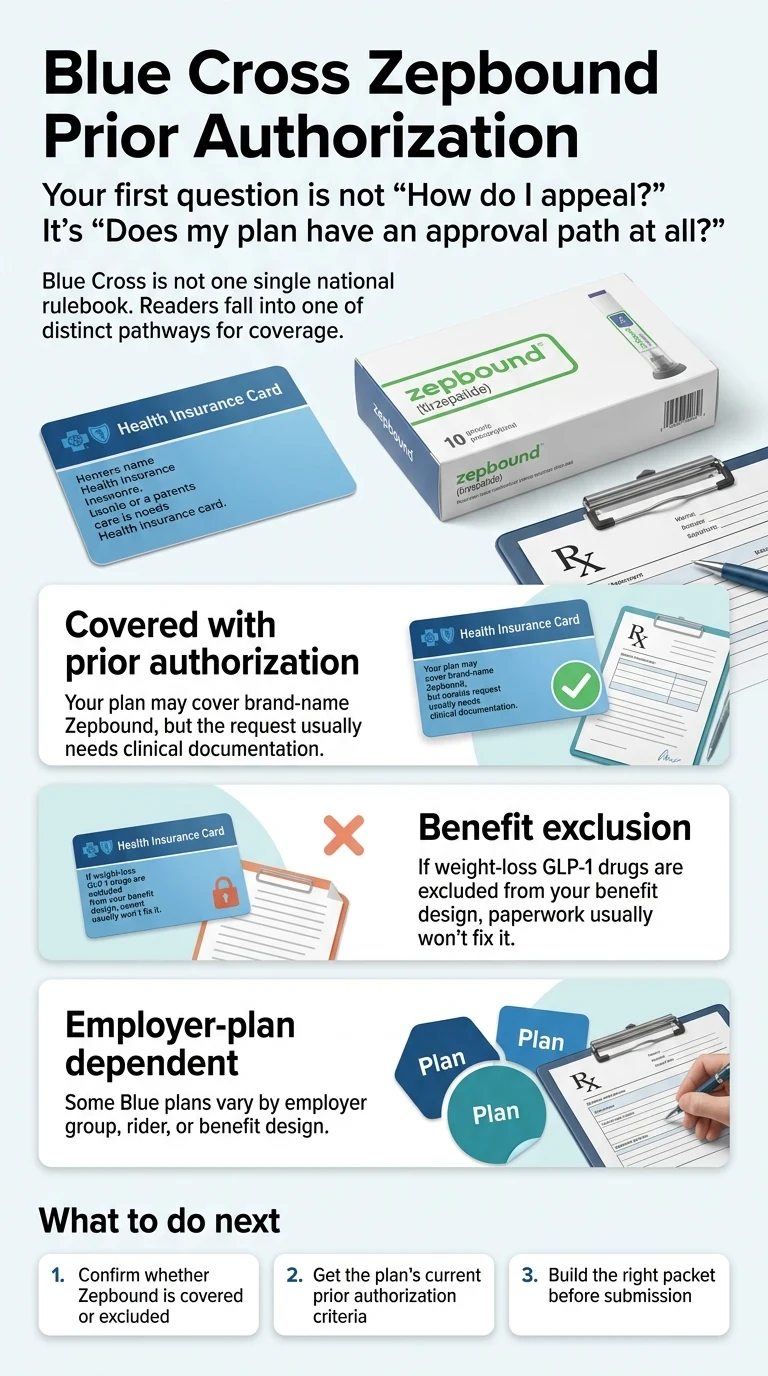
Blue Cross Zepbound prior authorization is not one national rule — it’s a different rule for every plan, and the first thing you need to figure out isn’t your paperwork. It’s whether your plan has an approval path at all.
Some Blue Cross plans still cover Zepbound with a prior authorization. Others removed weight-loss GLP-1s from the benefit entirely in 2025 or 2026, which means there’s nothing to authorize, nothing to appeal, and no amount of doctor letters will change that. Those are two completely different problems with two completely different fixes, and most of the frustration we see online comes from people chasing the wrong one.
Here’s the short version before you scroll. Across the verified Blue plans on this page, common approval requirements include a qualifying BMI (most plans we checked use 30+, or 27+ with a weight-related condition like hypertension, type 2 diabetes, high cholesterol, or sleep apnea), documented lifestyle-program participation, and on some plans (including FEP Blue), a prior trial of preferred products such as Wegovy or Saxenda. Review timelines vary by plan — Blue Shield California publishes a 24–72 hour standard drug PA review window, while end-to-end coverage flows through telehealth providers like Ro typically take two to three weeks.
Your fastest next step by situation
| Your situation | Fastest next step |
|---|---|
| I don't know if my plan even covers Zepbound | Check your coverage path first — Denial or Exclusion? |
| Doctor hasn't submitted the PA yet | Build the packet before submission — The Document Checklist |
| Denial letter says "benefit exclusion" or "not a covered benefit" | Stop fighting the appeal — Fallback options |
| I have FEP Blue | Read the FEP-specific row — strict but real — Friction Matrix |
| I have moderate-to-severe sleep apnea | May open a route your weight-loss rule wouldn't — OSA pathway |
| Renewal was approved last year but denied this year | Read the renewal trap — you're not alone — Renewal denials |
One 10-second question saves most people three weeks.
Denial or Exclusion? (Why Everyone Gets This Backwards)
Answer capsule
A Zepbound denial and a Zepbound benefit exclusion look similar on paper, but they’re not the same problem. A denial typically means your plan covers Zepbound in some form and rejected your specific request — usually for missing documentation, BMI criteria, or step therapy rules. A benefit exclusion means your plan’s design doesn’t include weight-loss GLP-1s at all. Certain Blue plans — BCBS Massachusetts and Health New England among them — explicitly state their 2026 weight-loss GLP-1 exclusions cannot be appealed.
Here’s the truth most articles won’t say out loud. Blue Cross Blue Shield isn’t one company — it’s a brand license shared by more than 30 independent local companies, each setting its own formulary, its own PA criteria, and its own benefit designs (source: BCBS Association, About the Blue Cross Blue Shield System). Anthem, Highmark, CareFirst, BCBS Michigan, BCBS Massachusetts, Blue Shield California, Independence Blue Cross, HCSC (which runs BCBS in Illinois, Texas, Oklahoma, New Mexico, and Montana), and Health New England can all give you completely different Zepbound answers.
That’s why “does Blue Cross cover Zepbound” is the wrong question. The right question is: does your specific plan list Zepbound as a covered benefit — or does it exclude weight-loss GLP-1s entirely?
Three buckets. You’re in one of them.
Bucket 1
Covered with prior authorization
Your plan’s formulary lists Zepbound as covered, typically with a PA requirement. This is the group the checklist and PA-mechanics sections below are written for.
Bucket 2
Excluded entirely, with variants
Growing fast. BCBS Michigan stopped covering GLP-1s for weight loss for fully-insured large-group commercial members as of January 1, 2025 (source: BCBSM Provider Alert, June 2024). BCBS Massachusetts standard commercial plans excluded Wegovy, Saxenda, and Zepbound for weight management starting with 2026 plan renewals, and their own account/broker materials state the exclusion cannot be appealed (source: BCBS Massachusetts GLP-1 FAQ). Health New England, Independence Blue Cross, and other affiliates have similar exclusions on specific group types.
Bucket 3
Benefit-design dependent
Blue Shield California’s 2026 provider notice confirms coverage varies by benefit plan — some groups cover Class III obesity only (BMI ≥40) with program participation, some cover the standard BMI ≥30 or ≥27 with a weight-related condition, some employer groups offer no weight-loss coverage. HCSC (BCBS Illinois, Texas, Oklahoma, New Mexico, Montana) publicly states that GLP-1 weight-management coverage is not a standard benefit and may be available only as a custom benefit on self-funded employer plans.
How to tell which bucket you’re in before you waste a month
One phone call. The number is on the back of your member ID card (the pharmacy benefits number, not the general member services line). Tell them exactly this:
“I’d like to know if tirzepatide, brand name Zepbound, is covered under my pharmacy benefit for weight management. If it is, can you tell me the prior authorization criteria? If it’s not covered, can you confirm whether it’s a benefit exclusion or a formulary non-coverage I could request an exception for?”
That script works because it forces the rep to answer the exclusion question directly, not deflect into generic “talk to your doctor” advice. Write down the rep’s name, the reference number, and the exact words they use. If they say “excluded” or “not a covered benefit,” you’re in Bucket 2 — head to the fallback section. If they say “requires prior authorization” or “formulary exception available,” you’re in Bucket 1 — keep reading.
What Blue Cross Plans Actually Require for Zepbound Prior Authorization
Answer capsule
Across the Blue Cross plans we verified for April 2026, common PA requirements include a qualifying BMI or diagnosis, documented prior weight-loss attempts, proof of participation in a structured lifestyle program, no concurrent use of another GLP-1, and on some plans (notably FEP Blue), step therapy requiring a prior trial of preferred products such as Wegovy or Saxenda. Each Blue plan states these requirements differently — which is why we built the Friction Score below.
We read the 2026 policy documents, provider forms, and member bulletins for the biggest Blue plans to build a single-page comparison nobody else has assembled in this form.
The RX Index Blue Cross Zepbound PA Friction Matrix (April 2026)
The Friction Score is our editorial rating — not an insurer-produced number. We score each plan 1–5 based on how many major approval hurdles appear in the current public policy: BMI threshold, documentation or program proof, step therapy or preferred-product rules, renewal hurdles, and plan-level admin complexity. Higher score means harder to get approved on a first submission.
| Blue Plan | What the Current Policy Shows | RXI Friction Score | Plain-English Takeaway |
|---|---|---|---|
| Blue Cross umbrella | Federation of 30+ independent local companies, each with its own formulary and PA criteria. No single national Zepbound rule exists. | — | First question: which Blue company and which benefit design? |
| FEP Blue (Federal Employee Program) | 2026 pharmacy policy requires qualifying BMI and comorbidity, documented inadequate response, intolerance, or contraindication to two oral weight-loss medications, participation in a comprehensive weight-management program, no concurrent GLP-1 therapy, and trial of preferred products (Saxenda and Wegovy are listed as preferred products for Zepbound in the 2026 FEP preferred-products document). Initial approval is 6 months; renewal requires 5% baseline weight loss maintenance. Zepbound is Tier 3 non-preferred on FEP Blue Basic and Standard, Tier 2 preferred on FEP Blue Focus. | 4/5 | Strict but real. If you can document a Wegovy or Saxenda trial, the path is open. |
| Highmark BCBS (PA, WV, DE, NY) | Current provider PA form requires lifestyle program proof with unusually specific acceptable evidence: provider chart notes, recurring receipts for Noom, Weight Watchers, or Omada, dietary logs, nutrition counseling receipts, gym receipts, summary reports from a wearable device (showing elevated heart rate for 20+ minutes, 3+ times weekly for a month), and personal trainer receipts. Also requires comorbidity documentation, previous medication trials with dates and outcomes, and prescriber rationale. | 4/5 | Documentation-heavy but transparent — if you can show the program proof, you can win. |
| BCBS Michigan / Blue Care Network | GLP-1 weight-loss coverage ended for fully-insured large-group commercial members on January 1, 2025 (self-funded employer groups may retain coverage at employer option). Where coverage remains, the current BCBSM/BCN April 2026 criteria show Zepbound coverage is group-benefit dependent and define two public routes: (1) BMI ≥30 or ≥27 with comorbidity or moderate-to-severe OSA in adults with obesity; and (2) a separate stricter route requiring BMI ≥35 with 6 months of documented lifestyle program participation. Renewal requires 5% baseline weight loss. | 5/5 | Most members lost weight-loss coverage in 2025. If you're self-funded, ask HR before assuming. |
| BCBS Massachusetts commercial | Starting with 2026 plan renewals, most commercial plans exclude Wegovy, Saxenda, and Zepbound for weight management unless the employer buys the optional GLP-1 rider. BCBSMA account/broker materials state the exclusion is a benefit-design decision and coverage cannot be appealed. Mounjaro coverage for type 2 diabetes is unaffected. | 5/5 | Don't appeal a benefit exclusion. Ask HR whether your employer bought the GLP-1 rider. |
| Blue Shield California large-group commercial | 2026 provider notice confirms coverage varies by benefit plan: some groups cover Class III obesity only (BMI ≥40) with comprehensive weight-loss program participation, some cover the standard BMI ≥30 or ≥27 with condition, some employer groups offer no weight-loss coverage. Drug prior authorizations submitted through the standard channel typically review within 24–72 hours per Blue Shield CA's member PA page. | 3/5 | Fastest published review window in the matrix — but coverage depends entirely on your employer's plan. |
| Independence Blue Cross (PA) | Ended standard-benefit weight-loss GLP-1 coverage (including Zepbound) for fully-insured group and individual commercial members effective January 1, 2025. Coverage continues for type 2 diabetes and cardiovascular indications. | 5/5 | Appeals won't work for weight-loss indication. Ask HR about riders; self-pay is the realistic route. |
| HCSC (BCBS IL, TX, OK, NM, MT) | BCBSIL pharmacy materials explicitly state coverage for GLP-1 weight-management drugs like Zepbound is not a standard benefit and may be available only as a custom benefit on self-funded employer plans. Verify your plan's 2026 formulary directly. | 4/5 | Not a standard benefit. Employer-plan dependent. Check your formulary directly before assuming. |
| Anthem BCBS (multi-state) | Coverage and PA criteria vary significantly by state affiliate and employer plan. Verify your specific plan's 2026 formulary and PA form before relying on any general rule. | 3/5 | Varies widely. Pull your plan-specific formulary. |
| CareFirst BCBS (MD, DC, VA) | Coverage and PA criteria vary by specific plan and employer group. Verify your plan's 2026 formulary directly. | 3/5 | Varies widely. Pull your plan-specific formulary. |
| Health New England | Weight-loss GLP-1 coverage (including Zepbound) ends for Individual and Small Group members on January 1, 2026; large groups under 100 lose coverage on renewal; groups of 100+ can purchase a rider to retain coverage; ASO/self-funded groups choose. No grandfathering of existing approvals. | 5/5 | Group-size specific. Ask HR where your group falls. |
Sources: FEP Blue 2026 Pharmacy Policy · CVS Caremark FEP Preferred Products · Highmark BCBS Zepbound PA Form · BCBSM/BCN PA Guidelines (April 2026) · BCBSM Provider Alert (June 2024) · BCBS Massachusetts Account/Broker GLP-1 FAQ · Blue Shield California 2026 provider news + member Drug PA page · Independence Blue Cross provider communications · Health New England GLP-1 Coverage notice · BCBSIL pharmacy communications.
A few notes on how to read this. The Friction Score isn’t a coverage score — it’s a “how much work is this going to be” score. A plan can be high-friction and still approve you. A plan can be low-friction and still deny you if your documentation is thin. And a plan with a 5/5 because of a benefit exclusion isn’t asking for more work — it’s telling you the work won’t matter. Don’t confuse those.
One more thing the matrix won’t show: self-funded employer plans can override the affiliate default in either direction. If your company self-insures, your HR or benefits portal is the real source of truth, not the state Blue plan’s public policy. Ask HR whether your plan includes a GLP-1 exclusion or rider.
If your plan is in Bucket 1 (covered with PA): the document checklist below is what your doctor needs.
If you’re not sure your plan has a real path: Check your coverage free through Ro’s Insurance Coverage Checker → (sponsored affiliate link, opens in a new tab) Ro’s insurance specialists pull the specifics from your actual plan, not the generic state-level policy, and email you the answer.
The Document Checklist That Gives a Blue Cross Zepbound PA the Best Chance
Answer capsule
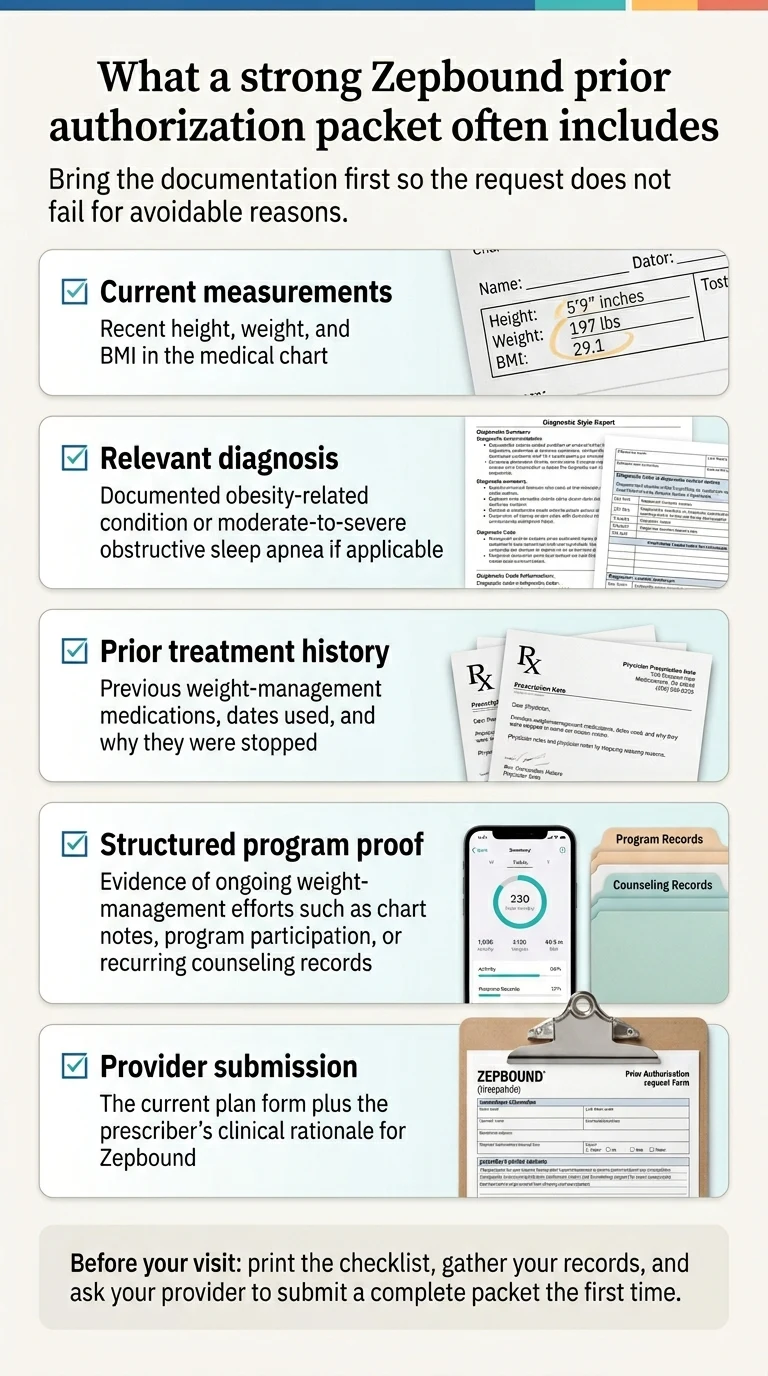
Blue Cross Zepbound PA forms repeatedly ask for the same evidence categories: diagnosis documentation with ICD-10 codes, baseline weight and BMI measured recently, prior medication trials with dates and outcomes, structured weight-management program participation, and a clinical rationale from the prescriber. Submitting all of it on the first try reduces the odds of a documentation-based denial.
We built this checklist by combining the acceptable proof examples from the Highmark PA form, the FEP Blue 2026 policy requirements, and BCBSM’s April 2026 documentation criteria into a single list that satisfies the strictest common denominator. If your packet clears this bar, you’ll clear most Blue plans’ PA requirements.
The base packet
Clinical measurements, dated within the last 3 months:
- ✓Current height, weight, and calculated BMI, documented in the chart
- ✓Baseline weight from 12 months ago if available (strengthens weight-history claims)
- ✓Blood pressure, A1C, lipid panel — any metric that supports a qualifying comorbidity
Qualifying comorbidity (required if BMI is 27–29.9; strengthens any submission):
| Condition | Common ICD-10 | Notes |
|---|---|---|
| Hypertension | I10 | One of the most common qualifying conditions |
| Type 2 diabetes / prediabetes | E11.x / R73.03 | Coded diagnosis required, not a verbal mention |
| Dyslipidemia / hyperlipidemia | E78.x | Includes high LDL, high triglycerides |
| Obstructive sleep apnea | G47.33 | Sleep study with AHI ≥15 required for the OSA indication |
| Cardiovascular disease | I25.x | May open separate cardiovascular pathways on some plans |
Casually mentioning “high blood pressure runs in my family” won’t work. The comorbidity needs a diagnosis code in your chart your doctor can cite.
Prior medication trials (dates, doses, outcomes):
List every weight-loss medication you’ve tried — Wegovy, Saxenda, phentermine, Contrave, Qsymia, Xenical — with start date, end date, dose escalation, and reason stopped (side effects, lack of efficacy, insurance issue, or contraindication). If you’ve tried Wegovy or Saxenda specifically, document that thoroughly — FEP Blue’s 2026 preferred-products document lists both as the preferred products for Zepbound, and a documented trial and response is what the step therapy exception relies on.
Structured lifestyle program participation (this is where most first submissions stumble):
The bar isn’t “I eat better and walk more.” It’s documented, ongoing, program-based participation. Acceptable evidence examples from the current Highmark PA form (one of the most detailed we’ve seen):
- ✓Chart notes from your provider documenting ongoing weight-management counseling
- ✓Recurring receipts from Noom, Weight Watchers, Omada, or a similar structured program
- ✓Dietary logs kept consistently
- ✓Nutrition counseling receipts from a registered dietitian
- ✓Gym membership receipts (recurring, not a one-time trial)
- ✓Wearable device reports showing elevated heart rate for 20+ minutes at least 3 times per week for a month
- ✓Personal trainer receipts (recurring)
BCBSM’s documentation-heavy route requires six months of this evidence before initial approval. FEP Blue requires participation in a comprehensive weight-management program per its 2026 Zepbound policy; check your plan’s exact duration requirement on the PA form, not on this page.
Prescriber-submitted items:
- ✓Letter of medical necessity from your provider (request this specifically — many offices don't include one by default)
- ✓Clinical rationale for Zepbound specifically versus a preferred product (required if your plan has step therapy)
- ✓Attestation that you're not on another GLP-1 concurrently
- ✓Plan-specific PA form, current version (download fresh — forms change quarterly)
What to add if you’re using the OSA pathway
- ✓Sleep study results confirming AHI (apnea-hypopnea index) ≥15 events per hour
- ✓CPAP/BiPAP use records if you've trialed positive airway pressure, plus documentation of inadequate response, intolerance, or contraindication
- ✓BMI ≥30 documentation
What to add if this is a renewal
- ✓Weight history showing at least 5% loss from baseline (required for renewal approval on plans including FEP Blue and BCBSM's documented route)
- ✓Side effect log if applicable
- ✓Documentation of continued lifestyle program participation through the initial approval period
- ✓If your plan changed PA criteria at renewal (FEP and others have tightened in 2026 without grandfathering), a new submission may need to meet the new criteria, not the ones you met originally
How Long Does Blue Cross Prior Authorization Take for Zepbound?
Answer capsule
Review timelines vary by plan. Blue Shield California’s member prior authorization page states drug PAs typically review within 24–72 hours once submitted. Ro’s published insurance workflow says the full end-to-end GLP-1 insurance process — benefits verification, PA submission, any back-and-forth, and pharmacy fulfillment — typically takes two to three weeks.
Here’s what the clock actually looks like:
| Stage | What Happens | Typical Time |
|---|---|---|
| Benefits verification | Call your plan to confirm coverage, pull the PA form, identify the PBM | 1–5 days |
| PA submission | Provider submits via ePA, CoverMyMeds, fax, or direct portal | Same day once docs are gathered |
| Plan review | Most Blue plans review within 1–7 business days; Blue Shield CA states 24–72 hours standard | 24 hours – 14 business days |
| Pharmacy fulfillment | Prescription sent, filled, or picked up (longer if dose is on shortage) | 1–7 days |
The two numbers that matter: 24–72 hours is what Blue Shield of California says about review once a complete PA is submitted (source: Blue Shield CA Drug Prior Authorizations page). Two to three weeks is what Ro publishes for its full end-to-end GLP-1 insurance process (source: Ro Weight Loss Program and Insurance page). The difference between those numbers is where most people lose patience — it’s almost entirely the stuff that happens before and after plan review, not plan review itself.
When to follow up and when to stop waiting
- →Day 7 after submission with no response: call the pharmacy benefits number, confirm receipt, ask for a status update, and write down the reference number.
- →Day 14 with no response: your PA is either stuck in a queue or was rejected without notice. Call again and ask for the decision in writing.
- →Day 21 with no response: something is wrong with the submission itself. Your doctor’s office probably needs to resubmit.
Why Blue Cross Denies Zepbound — and Which Denials Are Fixable
Answer capsule
Blue Cross Zepbound denials fall into a few recurring categories: incomplete documentation, step therapy or preferred-product rules, renewal criteria, wrong diagnosis track, and benefit exclusions. The most important move after any denial is to get the specific denial reason in writing before doing anything else — because the right fix depends entirely on the reason.
Insurance appeals can work. KFF’s analysis of Medicare Advantage data found that a substantial majority of appealed prior authorization denials were overturned (source: KFF Medicare Advantage prior authorization analysis, 2024). But the same data shows very few patients appeal in the first place. The gap between “appeals work” and “appeals get filed” is largely a knowledge gap. Here’s what you actually do.
Denial Type 1: Benefit exclusion
What the letter says: "This drug is not a covered benefit under your plan" or "weight-loss medications are excluded from this plan's pharmacy benefit" or similar language with no mention of missing documentation.
What it means: Your employer or plan design doesn't include weight-loss GLP-1s. This is a contract, not a clinical denial. BCBS Massachusetts's account/broker FAQ states explicitly that their 2026 GLP-1 exclusion cannot be appealed. Health New England's notice similarly describes the exclusion as a benefit-design decision.
What to do instead: Head to the fallback section. Consider asking HR whether your employer offers an optional GLP-1 rider that can be added at open enrollment. If you have moderate-to-severe OSA, check whether your plan covers Zepbound under the OSA indication — some plans that exclude weight-loss GLP-1s still cover the OSA route.
Denial Type 2: Incomplete or insufficient documentation
What the letter says: "Clinical criteria not met" or specific gaps like "BMI not documented" or "lifestyle program participation not documented."
What it means: Most likely fixable. Gather what was missing, resubmit with a complete packet.
What to do: Read the denial letter carefully — it will usually specify what was missing. Use the checklist above to gather the gaps, have your provider resubmit a complete PA with a letter of medical necessity, and include the original denial reference number.
Denial Type 3: Step therapy or preferred-product failure
What the letter says: "Must try preferred product first" or "step therapy criteria not met" or specifically names Wegovy or Saxenda.
What it means: Your plan wants you to try a preferred product before it covers Zepbound. FEP Blue's 2026 preferred-products document lists Saxenda and Wegovy as the preferred products for Zepbound.
What to do: Two paths. Either trial the preferred product for your plan's required period (check your plan's exact rule on the PA form) and document response or intolerance, then resubmit. Or, if you have a medical contraindication to Wegovy or Saxenda, a documented prior failure, or a clinical reason Zepbound is specifically indicated, your provider can request a step therapy exception with clinical justification. The exception path is faster when you have genuine documentation supporting it.
Denial Type 4: Renewal denial after successful initial year
What the letter says: "Renewal criteria not met," "insufficient weight loss," or cites new 2026 criteria your original approval didn't have to meet.
What it means: Your plan changed the rules at renewal. Several Blue affiliates tightened criteria for 2026 without grandfathering existing approvals, so a PA approved under 2025 criteria may need to meet stricter 2026 criteria when it renews.
What to do: Read the current renewal criteria carefully. FEP Blue's 2026 policy and BCBSM's documented route both require 5% baseline weight loss maintenance. Document your weight loss, your continued program participation, and resubmit under the new criteria. If you haven't maintained 5%, talk to your provider about dose adjustments or combined support.
Denial Type 5: Wrong diagnosis track
What the letter says: "Not medically necessary for stated indication."
What it means: The PA was submitted under a diagnosis your plan doesn't cover Zepbound for, even though another covered path might exist — most commonly when a plan excludes weight-loss coverage but would cover OSA.
What to do: If you have sleep apnea symptoms, pursue a sleep study. If AHI comes back ≥15, resubmit under the OSA indication. See the next section.
Appeal basics
Federal consumer guidance generally gives you up to 180 days to file an internal appeal after a denial (source: HealthCare.gov internal appeals guidance). Your specific plan’s appeal process and any external-review path are described in the denial letter itself — follow those instructions and deadlines. Eli Lilly publishes a free Prior Authorization Resource Guide and an Appeals Guide on the Zepbound access site, including template letter-of-medical-necessity language your provider can adapt.
The Preferred-Product Trap: What to Do If Your Denial Mentions Wegovy or Saxenda
Answer capsule
If your Blue Cross Zepbound denial specifically mentions Wegovy, Saxenda, or “preferred products,” your plan has a step therapy rule requiring a trial of a preferred weight-loss GLP-1 before Zepbound. FEP Blue’s 2026 preferred-products document lists Saxenda and Wegovy. Step therapy can often be bypassed with a documented exception if you have a contraindication, a prior failure, or a clinical reason Zepbound is specifically indicated.
Step therapy exists because plans want you to try the cheaper or contractually preferred option first. It’s annoying if you already know which medication your provider is recommending — but it’s not unbeatable, and many people don’t realize the exception path exists.
When to just try the preferred product first
If you haven’t tried Wegovy or Saxenda and you don’t have a contraindication, the fastest path to Zepbound coverage can be to trial the preferred product for the period your plan requires, then switch based on documented response. You’ll lose some weeks to the process, but you’ll be on active treatment during that time rather than fighting paperwork. Your plan’s PA form specifies the exact trial duration it requires.
When to push for the step therapy exception instead
Request the exception if any of these apply — and document each one carefully in your chart:
- ✓You've previously tried Wegovy or Saxenda and had inadequate response, significant side effects, or discontinued for any clinical reason
- ✓You have a contraindication to semaglutide or liraglutide (Wegovy's and Saxenda's active ingredients)
- ✓You have a specific clinical reason Zepbound is indicated over a preferred product — tirzepatide's dual GIP/GLP-1 mechanism may matter clinically for some patients who haven't responded to pure GLP-1 agonists, but this is a provider judgment
- ✓Your provider's clinical judgment is that step therapy delay risks patient harm
Your provider submits the step therapy exception request with clinical justification. If your plan has a true clinical denial pathway — not a benefit exclusion — the exception is usually processed within the normal PA timeline.
Does Sleep Apnea Change Your Blue Cross Zepbound Approval Path?
Answer capsule
Sometimes, yes. Zepbound received FDA approval for moderate-to-severe obstructive sleep apnea in adults with obesity in December 2024, and some Blue Cross plans recognize the OSA indication as a separate approval route with different criteria than the weight-loss route. BCBSM’s April 2026 criteria explicitly mention moderate-to-severe OSA in adults with obesity as one of the qualifying conditions in its baseline route. Not every Blue plan offers this pathway — confirm with your specific plan.
The OSA pathway is the single most underused approval route on Blue Cross. People hear “my plan excluded weight-loss GLP-1s” and give up, when they may still have a viable covered indication. If you have any of the symptoms below and haven’t had a sleep study, this is worth pursuing.
Common signs of sleep apnea (discuss with your provider)
- ✓Loud snoring, especially with partner-witnessed breathing pauses
- ✓Waking up gasping or choking
- ✓Daytime sleepiness despite apparently sufficient sleep
- ✓Morning headaches
- ✓Unrefreshing sleep
- ✓Difficulty concentrating
If you have BMI ≥30 plus any of these, ask your doctor about a sleep study.
What counts as moderate-to-severe OSA for the indication
FDA approval and most insurer criteria require an apnea-hypopnea index (AHI) of 15 or higher — 15 or more breathing events per hour during sleep. Severe OSA is AHI ≥30. Mild OSA (below AHI 15) typically doesn’t qualify for Zepbound under the OSA indication.
What to document for the OSA PA
- ✓Sleep study results with AHI ≥15
- ✓BMI ≥30 documentation
- ✓Symptom history
- ✓If you've tried CPAP or BiPAP: use records (the Highmark form asks specifically about 70% of nights for 4+ hours per night, over 2+ months) and documentation of inadequate response, intolerance, or contraindication
- ✓Prescriber rationale for Zepbound over continued CPAP alone
Important caution
Don’t assume every Blue plan covers Zepbound for OSA just because the FDA approved the indication. Plan policies differ, and some plans that excluded weight-loss GLP-1s may or may not recognize the OSA pathway. Call your plan before banking on this route, and get the answer in writing.
If Your Blue Plan Excludes Weight-Loss GLP-1s Entirely: Your Real Options
Answer capsule
If your Blue Cross plan has a benefit exclusion for weight-loss GLP-1s, appeals generally won’t work on the exclusion itself — certain plans (including BCBS Massachusetts and Health New England) explicitly state their exclusion cannot be appealed. The practical paths are direct-to-consumer self-pay through LillyDirect, or a telehealth provider who can prescribe Zepbound and handle any remaining coverage paths you might have. For many readers, a telehealth provider is the right first step because it runs the coverage check and provides either path in one place.
Most articles skip this section or treat it as a footnote. We’re putting it front and center because for a growing share of Blue Cross members, this is the actual answer.
Path 1: LillyDirect Self-Pay
Eli Lilly announced lower Zepbound single-dose vial pricing on December 1, 2025, with Self Pay Journey Program terms updated effective February 23, 2026. Per Lilly’s official current self-pay terms:
| Dose | Regular Self-Pay Price | Self Pay Journey Program Price |
|---|---|---|
| 2.5 mg vial (starter; not approved maintenance) | $299/month | — |
| 5 mg vial | $399/month | — |
| 7.5 mg vial or KwikPen | $499/month | $449/month |
| 10 mg vial or KwikPen | $699/month | $449/month |
| 12.5 mg vial or KwikPen | $699/month | $449/month |
| 15 mg vial or KwikPen | $699/month | $449/month |
Self Pay Journey Program pricing on 7.5 mg and higher requires you to refill within 45 days of your previous delivery. Miss the 45-day window and you pay the regular self-pay price for that refill; you can re-enroll on your next order. (Source: Lilly Zepbound Self Pay Journey Program Purchase Offer terms, effective February 23, 2026; Lilly investor release, December 1, 2025.)
LillyDirect ships directly to your home, or you can pick up at participating Walmart Pharmacy locations. No insurance is billed, no prior authorization is needed, and any valid prescription from a licensed provider works.
The tradeoff: vials require drawing medication with a syringe rather than using an autoinjector pen. The KwikPen option is available under the same Self Pay Journey Program pricing with the same 45-day refill rule.
Path 2: A telehealth provider who handles both insurance and cash pay
For most Blue Cross members who want FDA-approved brand-name Zepbound and some help figuring out whether insurance can cover any of it, a telehealth provider is the cleaner first step. Going straight to LillyDirect without a coverage check means you might pay cash for medication your plan would have covered under a different diagnosis (like OSA). Fighting your insurance for months and eventually losing wastes months. A provider who runs the coverage check first and then handles either path avoids both traps.
Of the providers we track at The RX Index — a pricing intelligence and comparison resource for GLP-1 telehealth providers — the one we recommend most often for Blue Cross members specifically is Ro, because their service is built around exactly this problem. More on that next.
Is Ro the Best Next Step for Blue Cross Zepbound Prior Authorization?
Answer capsule
For most commercial Blue Cross members who want brand-name Zepbound and help navigating prior authorization or self-pay, Ro is the cleanest telehealth fit we’ve verified. Ro publicly offers a free GLP-1 Insurance Coverage Checker that returns a personalized report showing whether your plan covers Zepbound and whether prior authorization is required. Ro members get access to an insurance concierge that, per Ro’s public materials, verifies benefits, submits prior authorization paperwork on the patient’s behalf, and fights for coverage. Get started for $39 the first month, then as low as $74/month with the annual plan paid upfront (ongoing monthly option is $149/month). Medication cost is separate.
Ro’s product is specifically built around the insurance-paperwork side of GLP-1 access, which matters on this page because you landed here searching for Blue Cross Zepbound prior authorization — meaning you’re trying to use your insurance.
Ro: Provider-stated vs what we verified
| Claim | What Ro publicly states | What we verified | Last checked |
|---|---|---|---|
| Free coverage check | Free GLP-1 Insurance Coverage Checker returns a personalized report indicating coverage and whether prior authorization is required | Confirmed on Ro's public GLP-1 Insurance Coverage Checker page | April 16, 2026 |
| Insurance concierge | Ro members are supported by an insurance concierge that verifies benefits, submits prior authorization paperwork, and fights for coverage | Confirmed on Ro's public Weight Loss Program and Insurance page and Ro's 2025 GLP-1 Insurance Coverage Checker Report | April 16, 2026 |
| FDA-approved medications | Ro prescribes FDA-approved Zepbound (tirzepatide) and other FDA-approved GLP-1s | Confirmed on Ro's public Weight Loss pages | April 16, 2026 |
| End-to-end timeline | Insurance process typically takes 2–3 weeks | Confirmed on Ro's public How It Works and Insurance pages | April 16, 2026 |
| Cash-pay fallback | Ro offers FDA-approved Zepbound vials at cash-pay pricing if insurance doesn't cover | Confirmed on Ro's public coverage and pricing pages | April 16, 2026 |
| FEHB coverage | FEHB members can join Ro Body membership and use the insurance concierge; Ro does not coordinate coverage for most other government insurance plans | Confirmed on Ro's public How It Works page | April 16, 2026 |
| Pricing | First month $39; ongoing $149/month; as low as $74/month with annual plan paid upfront | Verify on Ro's public pricing page before each publish — pricing can change | April 16, 2026 |
The honest tradeoff
Ro does not bill its membership to Blue Cross. If your Blue plan excludes weight-loss Zepbound entirely, Ro becomes a cash-pay path instead of an insurance win, and the ongoing membership fee is on top of the medication cost. If your priority is the absolute lowest possible price and you’d rather buy directly from Lilly without a provider relationship, LillyDirect self-pay is cheaper on paper.
Here’s why that tradeoff usually works in Ro’s favor when you’re coming from a Blue Cross PA search specifically: Ro doesn’t just prescribe — they verify coverage and submit the paperwork for you. The insurance concierge work — verifying benefits, submitting the PA with supporting documentation, following up with the plan — is what kills most first PAs when the patient or an unfamiliar doctor’s office tries to do it alone. A dedicated team running that process at scale is the difference between a three-week approval and a three-month loop.
- →If your plan is in Bucket 1 (covered with PA) and you want help not screwing up the paperwork: Ro.
- →If your plan is in Bucket 2 (excluded entirely) and you’d rather not pay a membership on top of self-pay: LillyDirect direct, or take our quiz and we’ll match you to the cheapest FDA-approved cash-pay route that fits your situation.
Real Ro member language (with disclosure)
Ro’s 2025 GLP-1 Insurance Coverage Checker Report includes a published member account describing how Ro handled prior authorizations through insurance when the member switched from Wegovy to Zepbound during a Wegovy shortage — with pharmacy coordination happening within about a week of contacting Ro. (Source: Ro’s 2025 GLP-1 Insurance Coverage Checker Report. Ro’s pricing page states that members were compensated for testimonials, so this is a paid testimonial published on Ro’s own platform. Use only to illustrate the insurance-handling experience, not medical efficacy or typical weight-loss results.)
Wrong fit? Here’s where to go instead
- →Plan fully excludes weight-loss GLP-1s and you don’t want a membership: LillyDirect self-pay, Zepbound vials starting at $299/month.
- →Not sure which path is right yet: Take our 60-second matching quiz →
- →Looking for other GLP-1 providers that work with Blue Cross: See our Aetna Wegovy PA guide →
What We Actually Verified for This Page
Answer capsule
This page was built by reading the primary Blue Cross plan documents directly and combining them with FDA labeling, manufacturer pricing releases, and verified telehealth provider pages. Every plan-specific claim in the matrix is tied to a public document. Where we couldn’t verify a specific plan’s 2026 rules, we’ve flagged the row as varies-by-plan rather than guessing.
Sources we verified directly
- ✓FEP Blue 2026 Zepbound Pharmacy Policy — BMI thresholds, two-oral-medication requirement, preferred-products rule, 6-month approval, 5% renewal maintenance, tier placement
- ✓CVS Caremark FEP Preferred Products document — Saxenda and Wegovy as preferred products for Zepbound
- ✓Highmark BCBS Zepbound Prior Authorization Form — acceptable evidence examples for lifestyle program documentation
- ✓BCBSM / Blue Care Network Prior Authorization and Step Therapy Guidelines, April 2026 — group-benefit dependency, two public approval routes, 5% renewal maintenance
- ✓BCBSM Provider Alert (June 2024) — end of GLP-1 weight-loss coverage for fully-insured large-group commercial members January 1, 2025
- ✓BCBS Massachusetts Account/Broker GLP-1 FAQ — 2026 benefit exclusion; exclusion cannot be appealed
- ✓Blue Shield California provider news + member Drug Prior Authorizations page — 2026 large-group coverage variation; 24–72 hour drug PA review window
- ✓Independence Blue Cross provider communications — weight-loss GLP-1 exclusion effective January 1, 2025
- ✓Health New England GLP-1 Coverage notice — 2026 exclusion schedule by group size; no grandfathering
- ✓BCBSIL pharmacy communications — GLP-1 weight-management as non-standard benefit
- ✓Eli Lilly Zepbound Self Pay Journey Program Purchase Offer terms (effective February 23, 2026) — current pricing and 45-day refill rule
- ✓Eli Lilly investor release, December 1, 2025 — vial pricing reductions
- ✓Ro's GLP-1 Insurance Coverage Checker page, Weight Loss Program and Insurance page, How It Works page, 2025 GLP-1 Insurance Coverage Checker Report, pricing page
- ✓FDA approval of Zepbound for moderate-to-severe obstructive sleep apnea in adults with obesity (December 2024)
- ✓KFF analysis of appeal overturn rates for Medicare Advantage prior authorization (2024)
- ✓HealthCare.gov internal appeals guidance
What we could not fully verify
- !Exhaustive state-by-state rules for every Anthem, CareFirst, Regence, Premera, and Horizon plan (these vary significantly by employer group; check your plan's 2026 formulary directly)
- !Whether specific self-funded employer plans at your workplace override their affiliate's default — this is HR's domain
- !Provider testimonial statements (paid and published on Ro's platform; sourced but not independently verified)
How we update this page
This page is reviewed quarterly and more frequently during open enrollment (October through December). LillyDirect pricing, Ro pricing, and FDA approvals are checked monthly. When a material change happens, we update the page and bump the “Last verified” date.
Last verified: April 16, 2026.
Affiliate disclosure
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We earn a commission when readers use certain provider links on this page, including the Ro links. This does not affect our coverage of pricing, plan policies, or coverage changes — those are sourced from primary documents independent of any commercial relationship.
Frequently Asked Questions: Blue Cross Zepbound Prior Authorization
Does Blue Cross Blue Shield cover Zepbound?
Some Blue Cross plans cover Zepbound with prior authorization; others exclude weight-loss GLP-1s for affected groups as of 2025 or 2026. Because BCBS is a federation of more than 30 independent local companies, coverage depends on your specific plan. Call the pharmacy benefits number on your member ID card and ask whether Zepbound is a covered benefit or excluded.
Does FEP Blue cover Zepbound?
FEP Blue has a real prior authorization path for eligible members under its 2026 pharmacy policy. It requires qualifying BMI and comorbidity, documented inadequate response, intolerance, or contraindication to two oral weight-management medications, participation in a comprehensive weight-management program, and trial of preferred products (Saxenda and Wegovy are preferred products for Zepbound).
What BMI do you need for Blue Cross Zepbound prior authorization?
On most Blue plans we verified, the BMI threshold is 30 or higher, or 27 or higher with a qualifying condition like hypertension, type 2 diabetes, high cholesterol, or sleep apnea. Some Blue plan routes use higher thresholds — BCBSM's documentation-heavy route requires BMI 35 or higher with six months of lifestyle proof, and Blue Shield California's large-group commercial plans include variants that cover only Class III obesity at BMI 40 or higher.
Can you appeal a Blue Cross benefit exclusion?
It depends on which Blue plan you have. BCBS Massachusetts's 2026 GLP-1 exclusion FAQ and Health New England's GLP-1 coverage notice both state those specific exclusions cannot be appealed because they are benefit-design decisions. If your denial letter uses language like not a covered benefit rather than criteria not met, the exclusion itself typically isn't reversible through appeal, but your denial letter describes the specific appeal rights available under your plan.
Does Blue Cross cover Zepbound for sleep apnea?
Some Blue plans recognize the OSA indication as a separate approval route with different criteria than weight-loss coverage. BCBSM's April 2026 criteria, for example, include moderate-to-severe OSA in adults with obesity in the qualifying-condition list. Not every Blue plan accepts the OSA pathway — confirm with your specific plan.
How long does Blue Cross prior authorization take for Zepbound?
Review timelines vary by plan. Blue Shield California publishes a 24–72 hour typical drug PA review window. Ro's published insurance workflow says the full end-to-end GLP-1 insurance process typically takes two to three weeks.
Do you have to try Wegovy or Saxenda before Zepbound on Blue Cross?
On some Blue plans, yes. FEP Blue's 2026 preferred-products document specifically lists Saxenda and Wegovy as preferred products for Zepbound. If you have already tried and had inadequate response to either medication, document the trial thoroughly and your provider can request a step therapy exception.
Can Blue Cross deny a Zepbound renewal even if the medication is working?
Yes. Several Blue plan approvals — including FEP Blue and BCBSM's documented route — require 5% baseline weight loss maintenance for renewal. Several Blue affiliates tightened criteria for 2026 without grandfathering existing approvals.
Still Not Sure Which Path Is Right for You?
If you’re stuck between “my insurance might cover this” and “I should just pay cash” — or you’re worried you’ll start a PA, wait three weeks, get denied, and be back at square one — take our free 60-second matching quiz. We’ll ask about your insurance situation, your goals, and your comfort level with the insurance process, then match you to the fastest realistic path to your first dose.
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. Policies, pricing, and provider offerings change often in GLP-1 — bookmark this page and come back when your plan year rolls over.
By The RX Index Editorial Team · Last verified: April 16, 2026. Created from primary Blue Cross plan documents, FDA labeling, manufacturer pricing releases, and verified telehealth provider pages. We do not add a “medically reviewed by” claim because no physician reviewed this editorial content.
Related guides and resources
- Aetna Wegovy Prior Authorization: Approval Checklist & What If Denied →
- How to Appeal a Zepbound Denial →
- Zepbound Savings Card: Eligibility & HSA/FSA Conflict →
- Letter of Medical Necessity for GLP-1 →
- GLP-1 Superbill Guide: Insurance Reimbursement Playbook →
- Zepbound vs Wegovy: Which Wins on Coverage and Cost →
- Zepbound for Sleep Apnea: FDA Indication & Coverage →
- Find My GLP-1 Path: 60-second matching quiz →
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup