Long Term GLP-1 Treatment: 5 Paths, Cost & Safety (2026)
By The RX Index Editorial Team
Published: · Last updated: · Last reviewed:
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. This guide is educational and is not a substitute for medical advice from your prescribing clinician. We earn affiliate compensation from some providers we mention. Our analysis is based on verified clinical, regulatory, and pricing sources.
The bottom line, before you scroll
Long term GLP-1 treatment usually means treating your weight or metabolic health as a chronic-care plan — not running a 90-day diet sprint. The American Association of Clinical Endocrinology's 2025 algorithm classifies obesity as a chronic condition that needs long-term care. The World Health Organization's December 2025 guideline conditionally recommends GLP-1 therapies as long-term treatment for obesity in adults.
In SELECT — the largest long-term GLP-1 trial we have — semaglutide produced sustained weight loss of -10.2% at week 208 versus -1.5% on placebo, plus a 20% reduction in major adverse cardiovascular events. The catch: when people stop, regain is common. STEP-1 extension showed about two-thirds of lost weight came back within a year. A 2026 eClinicalMedicine meta-regression estimated about 60% of treatment-phase weight loss is regained within 12 months.
This page walks you through all five paths, the real safety data, and the math — so you can decide with eyes open. Get your personalized GLP-1 path →
Choose your path
| If this is your situation | Start with this section |
|---|---|
| "I'm afraid I'll be stuck on this forever" | Do you have to take a GLP-1 forever? |
| "I just hit goal weight — now what?" | What's a maintenance dose? |
| "Insurance just changed or denied me" | Insurance & coverage in 2026 |
| "Cost might break this for me" | What it really costs over 5 years |
| "I'm using compounded — is that OK long-term?" | Compounded vs. FDA-approved |
| "I'm worried about side effects in 5+ years" | Is it safe long-term? |
| "Who shouldn't be on a GLP-1 at all?" | Who should not use or continue |
| "I want to stop — how do I do it safely?" | What happens when you stop |
Not sure where you fit? Get your personalized GLP-1 path in 60 seconds → Maintenance, stopping, coverage, or provider match — answer 6 questions, get a personalized plan.
✓ What we actually verified this quarter
Last verified: May 5, 2026
This quarter we re-checked: LillyDirect Foundayo dose-by-dose pricing and Zepbound KwikPen pricing; NovoCare Wegovy and Wegovy pill pricing; Ro Body membership pricing and Ro's GLP-1 Insurance Coverage Checker; the Medicare GLP-1 Bridge launch date and full clinical eligibility criteria; the FDA's April 30, 2026 proposed exclusion of semaglutide, tirzepatide, and liraglutide from the 503B bulks list (public comment period closes June 29, 2026); SURMOUNT-4 post hoc analysis; the December 2025 WHO global GLP-1 guideline; the 2025 AACE ABCD algorithm; the ATTAIN-MAINTAIN 52-week data for orforglipron; CMS Medicare GLP-1 Bridge eligibility criteria and drug list; and Mass General Brigham Health Plan coverage policy changes.
What we did not re-verify this quarter: state-by-state Medicaid copay specifics, individual employer plan formularies.
Next scheduled verification: August 5, 2026.
What “long term GLP-1 treatment” actually means
Long-term GLP-1 treatment is the use of a GLP-1 receptor agonist (like semaglutide or liraglutide) or a dual GIP/GLP-1 agonist (tirzepatide) under clinical care for months or years to manage a chronic condition — most often obesity, type 2 diabetes, or established cardiovascular disease in eligible patients. It's not a quick weight-loss reset. The goal is to maintain health gains while managing side effects, cost, and access over time.
A GLP-1 (glucagon-like peptide-1) receptor agonist mimics a hormone your gut already makes after meals. It tells your brain you're full. It slows how fast your stomach empties. In some drugs, it also taps into a second hormone called GIP (glucose-dependent insulinotropic polypeptide) to amplify the effect. Tirzepatide — the active ingredient in Zepbound and Mounjaro — works on both pathways.
Long-term means different things in this conversation:
- Years on the same dose. Often the default if the medication is working.
- Years on a lower maintenance dose. A practical step-down once you've reached your goal, used in clinical practice though not always label-supported.
- A switch. From injection to pill. From one drug to another. From cash-pay to insurance-covered.
- A planned taper or stop. With structured lifestyle support to limit regain.
- Cycling. Periods on, periods off. The most controversial path.
We'll cover all five. But first, let's answer the question almost everyone is really asking.
Do you have to take a GLP-1 forever?
No, you don't have to. But many people benefit from staying on a GLP-1 long-term because trial data show weight maintenance while treatment continues and meaningful regain after stopping. “Forever” is one legitimate path among five. The right answer depends on your medication, your health, your insurance, your cost ceiling, and your goals — not a default rule.
Here's the honest truth most articles dance around. Obesity behaves like high blood pressure. If you stop the medication that controls it, the underlying biology comes back. That's not a moral failing. That's pharmacology. The American Association of Clinical Endocrinology made this official in its 2025 algorithm by classifying obesity as adiposity-based chronic disease (ABCD) — a chronic condition requiring long-term care, like hypertension or diabetes.
The World Health Organization went further in December 2025. Its first global guideline on GLP-1 medicines for obesity conditionally recommends them as long-term treatment in adults (excluding pregnant women). Separately, in 2025 WHO added GLP-1 therapies to its Essential Medicines List for type 2 diabetes in high-risk groups.
“It might take a year to lose the weight, but only four months to gain it back. It's like a rubber band — you pull it hard and it snaps back quickly.”
— Dr. John Morton, Yale Medicine
That's the rubber band. But here's what those headlines miss: continuing the medication isn't the only honest answer. There are five paths. Each has evidence. Each fits a different person.
One damaging admission, said clearly
A GLP-1 is not the right call if your only plan is to take it for 12 weeks, stop, and never think about it again. The data is unkind to that strategy. If you're open to treating your weight or metabolic health like a chronic condition the way millions of people treat blood pressure or thyroid issues — long-term GLP-1 treatment is a legitimate, evidence-supported path that the major medical bodies of 2025 and 2026 explicitly endorse.
Not sure if you're a maintenance, stopping, or coverage case? Get your personalized 5-year GLP-1 plan in 60 seconds →
What the evidence actually shows about staying on a GLP-1
Continued GLP-1 treatment shows sustained benefit for several years across multiple major trials. Semaglutide kept 15.2% weight loss going at 2 years in STEP 5 and -10.2% at 4 years in SELECT. Tirzepatide users who stayed on the drug kept 89.5% of their weight loss compared to 16.6% of those who switched to placebo (SURMOUNT-4).
Semaglutide at 2 years
The STEP 5 trial followed adults with overweight or obesity (without diabetes) on semaglutide 2.4 mg weekly for 104 weeks. Average weight loss: 15.2%. Weight stayed off as long as treatment continued. Published in Nature Medicine, 2022.
Semaglutide at 4 years (SELECT)
SELECT is the biggest long-term GLP-1 trial we have — 17,604 adults with established cardiovascular disease and overweight or obesity, without diabetes, followed for a median of about 40 months. The findings:
- Weight loss kept going: -10.2% at week 208 vs. -1.5% on placebo. Waist circumference dropped 7.7 cm. Both held steady for years.
- Major adverse cardiovascular events dropped 20% in this specific high-cardiovascular-risk population — for the right population, GLP-1s aren't just weight drugs, they're cardiovascular drugs.
- A SELECT subanalysis published in Nature Medicine in 2024 also found kidney protection over a median 182 weeks of follow-up.
Tirzepatide: continue vs. stop (SURMOUNT-4)
This is the trial that made “stay on it” the default clinical recommendation for many doctors.
- 670 adults with obesity completed a 36-week tirzepatide lead-in. Average weight loss: 20.9%.
- They were then randomly assigned: keep taking tirzepatide for another 52 weeks, or switch to placebo.
- The continued-tirzepatide group lost an additional 5.5%.
- The placebo group regained 14.0% in just 52 weeks.
- 89.5% of those who stayed on tirzepatide kept at least 80% of their weight loss. Only 16.6% of those who switched to placebo did.
A November 2025 post hoc analysis in JAMA Internal Medicine found that people who regained 25% or more of their weight loss after stopping also lost most of the cardiometabolic benefits — blood pressure, non-HDL cholesterol, fasting insulin, and waist circumference all reverted.
What the evidence does NOT prove
- It does not prove every adult on a GLP-1 should stay on it for life.
- It does not eliminate the need for safety monitoring.
- It does not make compounded GLP-1 products equivalent to FDA-approved medications.
- It does not replace nutrition, resistance training, and sleep.
- The longest randomized obesity trial we have is roughly 4 years (SELECT). Beyond that, data is observational.
What happens when you stop a GLP-1: the regain data
Most people regain a substantial portion of lost weight within a year of stopping a GLP-1. STEP-1 extension showed about two-thirds regain in 52 weeks. SURMOUNT-4 showed 14.0% regain on placebo over 52 weeks. A 2026 eClinicalMedicine meta-regression estimated about 60% of treatment-phase weight loss is regained within 12 months. Stopping isn't failure — but stopping without a plan increases risk.
| Trial / Source | Drug | Off-drug period | Regain |
|---|---|---|---|
| STEP-1 Extension (Wilding et al., DOM, 2022) | Semaglutide 2.4 mg | 52 weeks off | ~2/3 regained; +11.6 pp back |
| STEP 4 (Rubino et al., JAMA, 2021) | Semaglutide 2.4 mg | 48 weeks | Placebo arm regained 6.9% |
| SURMOUNT-4 (Aronne et al., JAMA, 2024) | Tirzepatide 10/15 mg | 52 weeks placebo | Placebo arm regained 14.0% |
| 2026 eClinicalMedicine meta-regression | Class-wide | Up to 1+ year | ~60% of treatment-phase loss at 12 months |
| Cleveland Clinic real-world (Gasoyan et al., AJMC, May 2025) | Semaglutide / Tirzepatide | 3+ months | Slower regain than trials in some patients |
The harder truth about adherence
Here's the part the rubber-band analogy misses: most people don't even make it to the regain question because they stop early. Blue Cross Blue Shield Association research released in 2025 found that nearly two-thirds of patients discontinue GLP-1 treatment before the 12-week mark needed for meaningful weight loss. More than 40% stop after just 4 weeks. Long-term success is mostly an adherence problem, not a pharmacology problem.
If you're going to stop anyway — plan it
| Why you might stop | Risk without a plan |
|---|---|
| You hit goal weight | Regain, returning hunger, loss of routine |
| Cost or insurance loss | Abrupt stop, emotional rebound, inconsistent dosing |
| Bad side effects | Dehydration, poor intake, dose anxiety |
| Pregnancy planning | Medication exposure concern |
| Surgery or anesthesia | Delayed gastric emptying matters perioperatively |
| Compounded access changed | Regulatory or supply disruption |
If your specific question is what happens when you stop Wegovy, our Wegovy stopping guide goes deeper on that single drug.
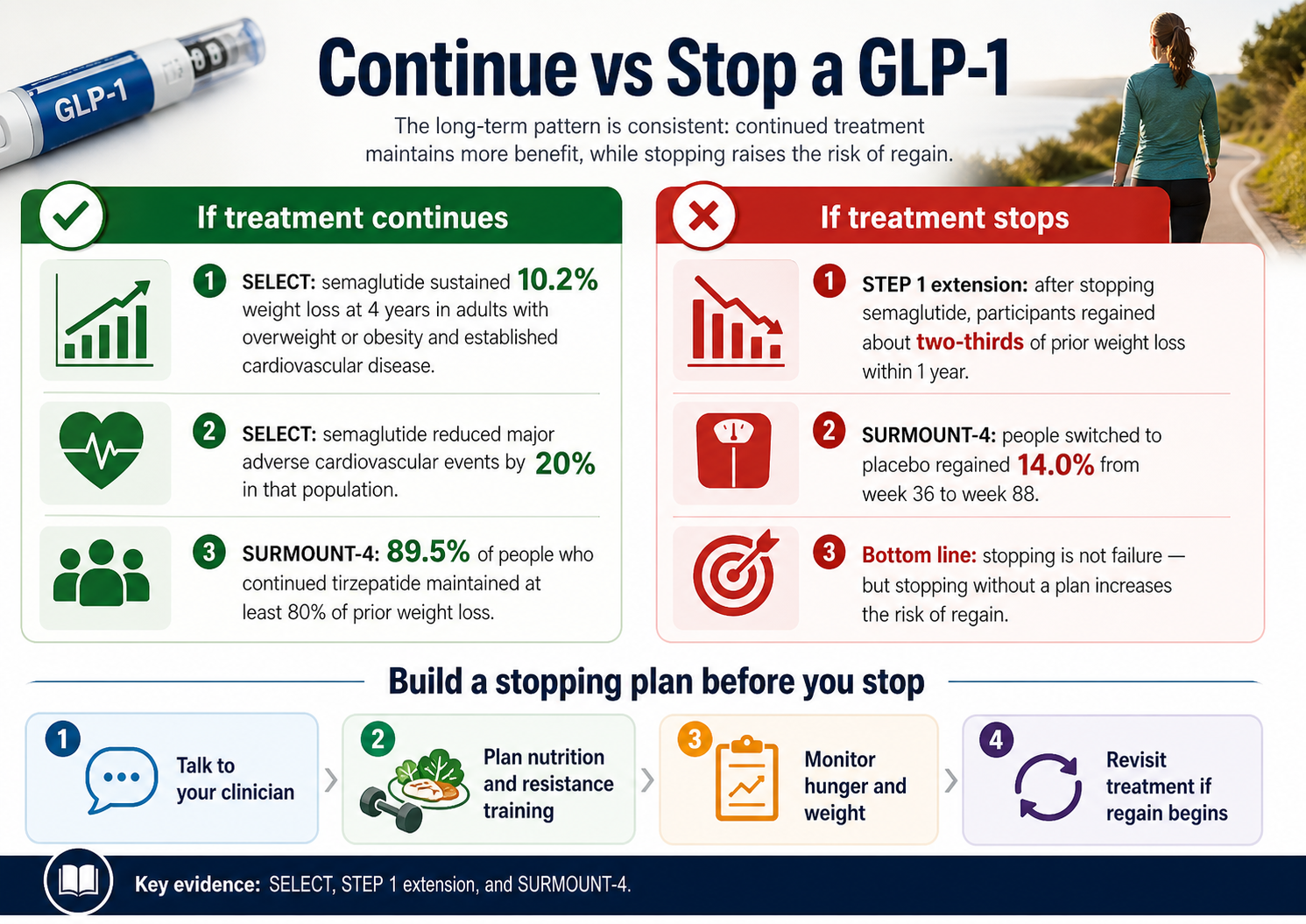
Key evidence: SELECT, STEP-1 extension, and SURMOUNT-4. The pattern is consistent — continued treatment maintains more benefit while stopping raises regain risk.
The 5-Path Long-Term GLP-1 Decision Matrix
There are five long-term paths for GLP-1 treatment: stay on the full dose, step down to a maintenance dose, switch to an oral GLP-1, taper off with structured lifestyle support, or cycle on and off in defined periods. Paths 1, 2, and 3 have the strongest evidence base. Paths 4 and 5 are real-world strategies some clinicians and patients consider, but they carry more regain or efficacy uncertainty.
| Path | What it means | Best fit |
|---|---|---|
| 1. Stay the Course | Continue full therapeutic dose indefinitely | Tolerating the drug, financially sustainable, no contraindications |
| 2. Maintenance Dose | Step down to a lower dose after reaching goal | Reached goal, want lower side-effect burden and cost |
| 3. Switch to Oral | Move from injection to Wegovy pill or Foundayo | People dreading lifelong injections; better long-term adherence |
| 4. Bridge & Taper | Use to goal, then taper off with structured lifestyle support | Cannot afford or tolerate indefinite use, willing to invest in supports |
| 5. Pause & Restart | Cycle on/off in defined periods | Using GLP-1 as a tool, not a destination; long-term safety concerns |
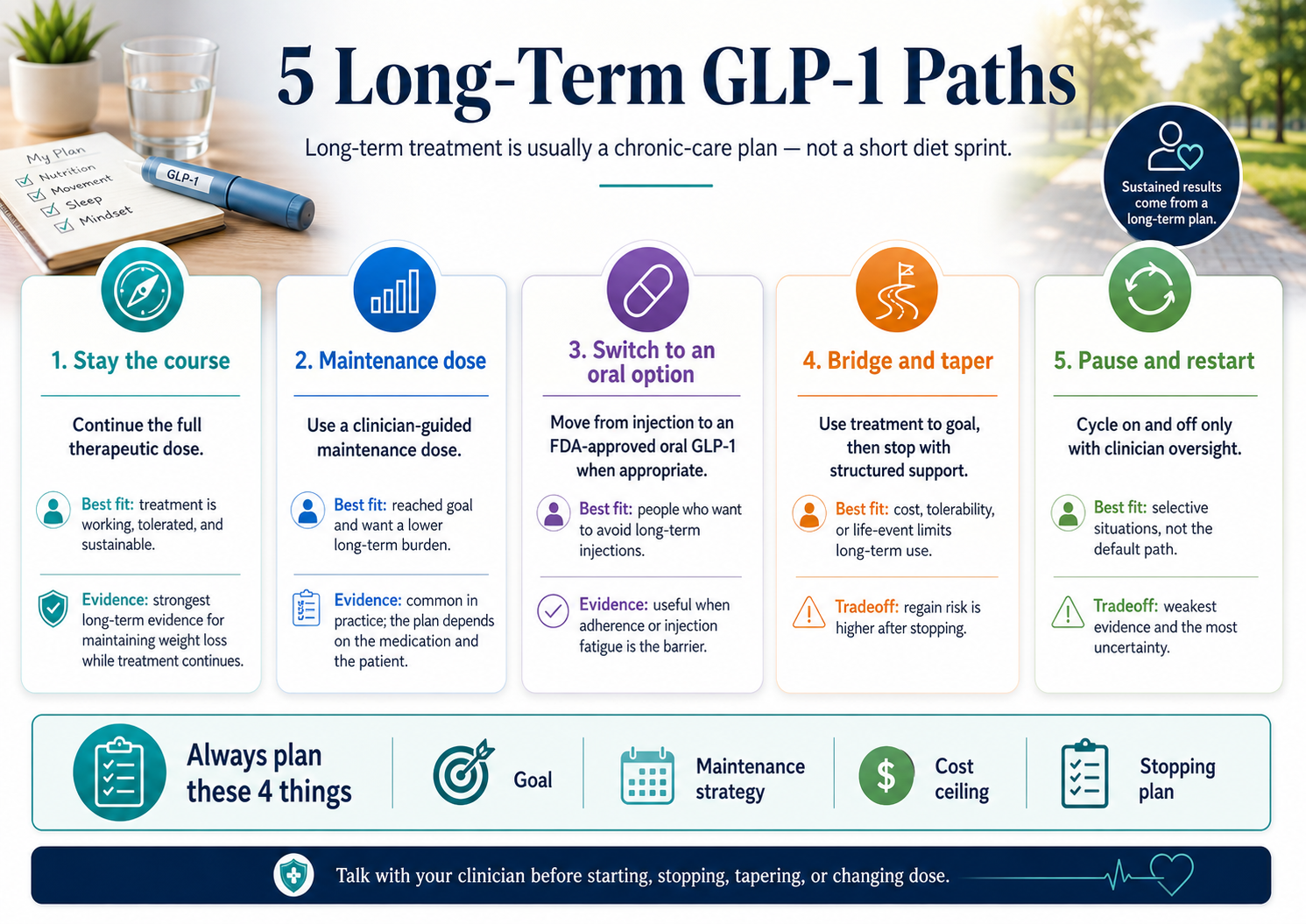
Always plan these 4 things: goal, maintenance strategy, cost ceiling, and stopping plan. Talk to your clinician before starting, stopping, tapering, or changing dose.
Path 1: Stay the Course
This is the path the major guidelines lean toward for most adults with obesity who tolerate the medication. The tradeoff is cost and the unknown of 10+ year safety. The benefit is the strongest evidence base for sustained weight maintenance and — in the right population — sustained cardiovascular protection.
Path 2: Maintenance Dose
Common in clinical practice, validating data still emerging. The SURMOUNT-MAINTAIN trial reads out in 2026 and will tell us whether dropping from full therapeutic tirzepatide to a 5 mg maintenance dose holds up against placebo and continued max dose. Important: dose stretching beyond the labeled schedule is off-label. Talk to your clinician — don't self-manage.
Path 3: Switch to Oral GLP-1
The 2026 game-changer for long-term adherence. Two oral GLP-1s are now FDA-approved for weight management:
- Wegovy pill (oral semaglutide 25 mg) — approved January 2026. Same active ingredient as injectable Wegovy, with cardiovascular indication retained.
- Foundayo (orforglipron) — approved April 1, 2026. First non-peptide GLP-1 that can be taken any time of day, with or without food.
In Eli Lilly's Phase 3 ATTAIN-MAINTAIN trial, orforglipron met the primary and key secondary endpoints for weight maintenance versus placebo at 52 weeks. The FDA has asked Eli Lilly for additional post-marketing studies on Foundayo for heart, liver, and other long-term risks — this isn't a red flag, it's the FDA being cautious with a brand-new molecule.
If switching to an FDA-approved oral or insurance-covered path fits your situation:
Check GLP-1 coverage with Ro → (sponsored affiliate link, opens in a new tab)Ro carries Zepbound® and Foundayo™, matches LillyDirect / NovoCare pricing on cash-pay medication, and includes a free GLP-1 Insurance Coverage Checker. Get started for $39, then as low as $74/month with annual plan paid upfront (Ro Body membership; medication billed separately).
Path 4: Bridge & Taper
Honestly, this has the weakest evidence base of the first four paths. But it's a real-world option for people who genuinely cannot afford or tolerate indefinite use and are willing to invest heavily in structured supports — protein, resistance training, behavioral coaching, ongoing follow-up. About 33–50% of people retain ≥5% net weight loss off-treatment in trial extensions. Your support infrastructure matters more than your medication choice.
Path 5: Pause & Restart
The most uncertain path. Preclinical data raise concerns that cycling on and off may reduce long-term effectiveness — a concept called tachyphylaxis (drug tolerance from repeated exposure). Gaps in treatment also reduce the sustained MACE benefit shown in SELECT. The evidence base is the thinnest of the five paths, and this should be a path you and your physician design together.
Want this matched to your specific situation? Get your personalized 5-year plan in 60 seconds →
What is a GLP-1 maintenance dose?
A GLP-1 maintenance dose is the dose your clinician keeps you on after the initial weight-loss phase to maintain your results. It's not one universal number — it's individualized based on tolerance, response, cost, and medical history. Don't lower, skip, or stretch doses on your own.
Different drugs have different built-in maintenance doses, based on current FDA labeling:
| Medication | FDA-labeled maintenance dose |
|---|---|
| Wegovy & Wegovy HD (semaglutide injection) | 1.7 mg or 2.4 mg once weekly for weight reduction (2.4 mg recommended). After 4+ weeks at 2.4 mg, label allows escalation to maximum 7.2 mg weekly (Wegovy HD). |
| Wegovy pill (oral semaglutide) | 25 mg daily. |
| Zepbound (tirzepatide) | 5 mg, 10 mg, or 15 mg once weekly for weight reduction. 10 mg or 15 mg once weekly for obstructive sleep apnea in adults with obesity. |
| Foundayo (orforglipron) | Starts at 0.8 mg once daily, increasing to 2.5 mg, then 5.5 mg, then up to 9 mg, 14.5 mg, or 17.2 mg (maximum) once daily after at least 30 days at each level, based on response and tolerability. |
Can you stay on a lower dose long-term?
Some patients do under clinician guidance. We're not aware of strong RCT data proving lower-dose maintenance prevents regain to the same degree as full-dose continuation. SURMOUNT-MAINTAIN will tell us more in 2026.
Can you space out doses to every 10–14 days?
Spacing injections beyond the labeled weekly schedule is off-label. Don't change dose timing without your clinician — and don't trust internet protocols that promise the same results at half the dose. The data isn't there yet.
What if you miss a dose?
Wegovy labeling says if you miss a dose and your next scheduled dose is more than 2 days away, take the missed dose. If less than 2 days, skip it. After missing 2 or more consecutive doses, your clinician may restart escalation to reduce GI side effects.
Is long-term GLP-1 treatment safe?
Across 4+ years of randomized trial data, FDA-approved GLP-1 medications have a well-characterized safety profile. Pancreatitis and pancreatic cancer concerns from early signals have been largely dispelled by long-term cardiovascular outcome trials. The medullary thyroid cancer signal from rodent studies remains an FDA boxed warning. Lean body mass loss accounts for roughly 20–30% of total weight lost in most studies and is mitigable with resistance training and adequate protein.
Confirmed & usually fade
- Nausea
- Vomiting
- Diarrhea or constipation
- Bloating
- Heartburn
- Fatigue
- Injection site reactions
Slow dose escalation reduces all of these.
Largely dispelled
- Pancreatitis (causal link not confirmed in long-term CV trials)
- Pancreatic cancer (JCI 2026 review: 'largely dispelled')
Acute pancreatitis remains a rare side effect to watch for.
Requires monitoring
- Medullary thyroid carcinoma (FDA boxed warning)
- Gallbladder disease
- Acute kidney injury (dehydration-linked)
- Diabetic retinopathy progression
- Aspiration risk during anesthesia
Tell your surgical team you're on a GLP-1 before any procedure.
The lean body mass question
Headlines claim GLP-1 users lose 40% of their weight as muscle. The truth is more nuanced. Across studies, lean body mass loss ranges from 15% to 40% of total weight lost. Most cluster around 20–30% — which UC Davis exercise physiologist Keith Baar pointed out in 2025 is no different from any calorie-restricted weight loss.
The 2025 SEMALEAN study tracked 12 months of semaglutide use. Lean mass dropped initially, then stabilized. Handgrip strength actually improved. Sarcopenic obesity prevalence dropped from 49% at baseline to 33% at month 12. The mitigation strategy: adequate protein (~1.0–1.2 g/kg ideal body weight), resistance training 2–3 times per week, enough sleep, and don't drop calories too low.
What we don't know about 10+ years
We don't have controlled data past about 4 years for obesity. SELECT-LIFE will provide up to 10 years of post-trial follow-up. Until then, anyone who tells you long-term GLP-1 use is “definitely safe” or “definitely dangerous” past a decade is guessing. The major guidelines (AACE 2025, WHO Dec 2025, ACC 2025) treat current safety data as sufficient to recommend long-term use while acknowledging the data gaps.
Who should not use or continue a GLP-1 long-term?
You shouldn't start or continue a GLP-1 long-term if you have a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2) — that's the FDA boxed warning. Other situations include pregnancy or active pregnancy planning, acute pancreatitis history, severe gastrointestinal disease, and intolerable side effects despite dose adjustment. Upcoming surgery requires telling your anesthesia team.
Hard contraindications — don't start, don't continue:
| Contraindication | Details |
|---|---|
| Personal or family history of MTC or MEN2 | FDA boxed warning across the GLP-1 class. Do not use. |
| Severe hypersensitivity reaction | History of severe hypersensitivity to the specific GLP-1 you're considering. |
| Pregnancy or active pregnancy planning | Semaglutide labeling says discontinue at least 2 months before a planned pregnancy. GLP-1 weight-loss treatment is not a pregnancy plan. |
Reasons to pause or stop with clinician guidance:
- Acute pancreatitis (current or recent history)
- Severe gastrointestinal disease that gastric emptying delays could worsen
- Intolerable side effects that don't improve with dose adjustment or drug switch
- Upcoming surgery — tell your anesthesia team. Slowed gastric emptying matters perioperatively.
- Severe diabetic retinopathy in patients with diabetes — rapid glucose improvement can temporarily worsen it
- Loss of insurance coverage with no realistic cash-pay or alternative path. Build a planned taper rather than abrupt stopping if you can.
For people on tirzepatide specifically: Zepbound labeling notes that delayed gastric emptying may affect absorption of orally taken medications, including oral contraceptives. A backup contraceptive method is recommended for 4 weeks after starting and after each dose escalation.
Build your long-term plan before you start
The best time to build a long-term GLP-1 plan is before your first prescription — not after side effects, a plateau, or an insurance denial. A complete plan covers seven things: your medical goal, your medication path, your response checkpoint, your side-effect strategy, your maintenance plan, your cost ceiling, and your stopping strategy.
This is the original RX Index 7-Part Long-Term GLP-1 Plan. Run through it before you commit:
Your medical goal
Weight loss alone? A1C control? Cardiovascular risk reduction? Sleep apnea? Mobility? Goals drive medication choice and duration.
Your medication path
FDA-approved with insurance? FDA-approved cash-pay direct? Compounded? “Not sure yet”? Each path has different long-term cost, regulatory stability, and clinical support.
Your response checkpoint
Most clinicians evaluate at 12–16 weeks. If you’re not seeing meaningful response by then, the question becomes dose, drug, or different approach — not “give it another year.”
Your side-effect strategy
What symptoms trigger dose adjustment? Which trigger urgent contact? Hydration plan? Antiemetic plan if GI symptoms get bad?
Your maintenance plan
What happens after goal weight? Stay on full dose? Step down? Switch to oral? You should know this before you reach goal, not figure it out on the fly.
Your cost ceiling
Maximum sustainable monthly cost. 12-, 24-, and 36-month total. What’s your “stop” trigger if cost rises beyond that?
Your stopping strategy
If you have to stop (insurance, side effects, life event) — what's your plan to limit regain? Lifestyle infrastructure, behavioral coaching, follow-up plan, possible bridge medication.
If you can't answer at least 5 of these 7 right now, you're not ready to commit to long-term treatment — and that's fine.
Get your personalized GLP-1 path →Six questions. A personalized 5-year plan.
What long-term GLP-1 treatment really costs over 5 years
Five-year out-of-pocket costs vary widely based on payment path. Medicaid copays in covering states can be very low. The Medicare GLP-1 Bridge offers $50/month copays for eligible Part D enrollees from July 1, 2026 through December 31, 2027 — up to $900 across the 18-month program. FDA-approved manufacturer-direct cash pay can run from $149/month at the lowest doses to $699/month at the highest tirzepatide doses without an active offer.
The single biggest mistake people make planning for long-term GLP-1 treatment? They look at first-month price. A “$39 first month” offer means nothing if month 13 is $400. The number that matters is your 12-month, 24-month, and 36-month total. All figures verified May 5, 2026 — pricing changes frequently.
| Payment Path | FDA Status | Monthly Cost Range |
|---|---|---|
| Compounded GLP-1 (cash, telehealth) | Not FDA-approved | $150–$300 typical |
| FDA-approved manufacturer direct (LillyDirect, NovoCare, TrumpRx) | FDA-approved | Foundayo $149–$349. Wegovy pill $149 first month, $199–$299 thereafter. Zepbound KwikPen $299–$699. |
| FDA-approved with commercial insurance (PA approved) | FDA-approved | $25–$300 typical copay |
| Medicare GLP-1 Bridge (July 1, 2026 – Dec 31, 2027) | FDA-approved | $50/month copay |
| Medicaid (state-dependent) | FDA-approved | Varies by state |
What changed in 2026
- November 2025 manufacturer deals — The Trump administration negotiated lower prices with Eli Lilly and Novo Nordisk, leading to $149 starting prices for the Wegovy pill and Foundayo at the lowest doses through manufacturer-direct channels.
- Medicare GLP-1 Bridge — Launches July 1, 2026. Eligible Part D enrollees pay $50/month for Foundayo (any FDA-approved formulation), Wegovy (any FDA-approved formulation), or the Zepbound KwikPen specifically through December 31, 2027. The $50 copay does not count toward TrOOP.
- Insurance shifts — Some commercial carriers tightened coverage. Mass General Brigham Health Plan dropped GLP-1 weight-management coverage for fully insured commercial members on January 1, 2026 (large employer groups may add it back at renewal). Coverage for diabetes, established cardiovascular disease, or obstructive sleep apnea remains more reliable.
Have insurance and want an FDA-approved path? Ro offers a free GLP-1 Insurance Coverage Checker — it tells you whether GLP-1 medications it carries may be covered under your plan before you commit. Ro also offers an insurance concierge for prior-authorization paperwork.
Check GLP-1 coverage with Ro → (sponsored affiliate link, opens in a new tab)Get started for $39, then as low as $74/month with annual plan paid upfront (Ro Body membership; medication billed separately).
Paying cash and want to compare options without committing? Find your cash-pay match in 60 seconds →
Compounded vs. FDA-approved GLP-1s for long-term treatment
For long-term planning, FDA-approved medications have clearer labeling, defined dosing, manufacturer quality controls, and regulatory stability. Compounded GLP-1 products are not FDA-approved. The FDA has not verified their safety, efficacy, or quality. As of April 30, 2026, the FDA proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list — narrowing the regulatory pathway for compounded versions.
| Factor | FDA-Approved | Compounded |
|---|---|---|
| FDA safety & efficacy review | Yes — full review | No — not verified |
| Defined dosage form & labeling | Yes | Varies by pharmacy |
| Manufacturer quality systems | Yes — GMP required | Varies (503A vs. 503B) |
| Regulatory stability (3-5 yr horizon) | High | Uncertain — proposed 503B exclusion pending |
| Cash-pay monthly cost (lowest dose) | $149/mo (Foundayo / Wegovy pill) | $150–$300 typical |
| AACE 2025 algorithm recommendation | Recommended | Advises against compounded alternatives |
The verification checklist if you're considering a compounded path
Before committing to compounded for long-term treatment, verify each of these:
If a provider can't or won't tell you the answers above, that's your answer.
Insurance, Medicare, Medicaid, and the 2026 coverage landscape
The Medicare GLP-1 Bridge launched July 1, 2026, providing eligible Part D beneficiaries access to all FDA-approved formulations of Foundayo and Wegovy plus the Zepbound KwikPen specifically for a $50 monthly copay through December 31, 2027. Coverage for GLP-1s prescribed for type 2 diabetes, established cardiovascular disease, or obstructive sleep apnea remains more reliable than weight management alone.
The Medicare GLP-1 Bridge
| Detail | What it means |
|---|---|
| Launch date | July 1, 2026 |
| End date | December 31, 2027 |
| Eligibility | Medicare Part D beneficiaries age 18+ prescribed the drug to reduce excess body weight with ongoing lifestyle modification, AND meeting one CMS clinical criterion (BMI ≥35; BMI ≥30 with HFpEF, uncontrolled hypertension on 2 meds, or CKD stage 3a+; BMI ≥27 with prediabetes, prior MI, prior stroke, or symptomatic PAD). |
| Cost | $50/month copay. Does not count toward TrOOP. Coupons and manufacturer discounts may not be applied. |
| Eligible drugs | All FDA-approved formulations of Foundayo and Wegovy. Zepbound KwikPen specifically. Excludes Zepbound single-dose vial and Zepbound pen. |
| Plan requirement | Standalone Part D plan or Medicare Advantage plan with drug coverage. |
For more detail on the Medicare Bridge and how to access it, see our Medicare GLP-1 Bridge Program guide.
Medicaid
Coverage for GLP-1s prescribed for obesity is optional for state Medicaid programs — 13 fee-for-service state Medicaid programs covered GLP-1s for obesity as of January 2026 (KFF), usually with utilization controls. Coverage for GLP-1s prescribed for type 2 diabetes is required nationwide. Coverage for established cardiovascular disease (Wegovy) and obstructive sleep apnea (Zepbound) is also required nationwide.
Commercial insurance trends
- Coverage for diabetes, CVD, or OSA: relatively stable.
- Coverage for weight management alone: tightening.
- Mass General Brigham Health Plan dropped GLP-1 weight-management coverage for fully insured commercial members on January 1, 2026 (large employer groups may add weight-loss drug coverage at renewal).
- Many other carriers are quietly raising prior authorization bars.
A tactical note on prior authorization
Initial PA denials are often automated. A well-written letter of medical necessity from your prescribing clinician — including diagnosis, BMI, comorbidities, prior weight loss attempts, and clinical rationale — can be the difference between a denial and an approval. Don't accept a first denial as a final answer.
What the 2025–2026 guidelines actually say
The 2025 AACE algorithm classifies obesity as adiposity-based chronic disease (ABCD), a complex chronic disease needing long-term care. The December 2025 WHO global guideline conditionally recommends GLP-1s as long-term obesity treatment in adults (excluding pregnant women). The 2025 ACC expert consensus supports medical weight management for cardiovascular health. None of these guidelines specify a stop date.
AACE 2025
American Association of Clinical Endocrinology
Classifies obesity as adiposity-based chronic disease (ABCD). Recommends GLP-1s as long-term therapy in eligible patients. Advises against compounded alternatives.
WHO Dec 2025
World Health Organization
First global guideline on GLP-1s for obesity. Conditionally recommends them as long-term treatment in adults (excluding pregnant women). Added GLP-1s to Essential Medicines List for T2D in high-risk groups.
ACC 2025
American College of Cardiology
Expert consensus supports medical weight management for cardiovascular health. Notes longest published GLP-1 obesity trial is ~4 years (SELECT).
What they all explicitly recommend: treat as long-term therapy when clinically appropriate, combine with nutrition and lifestyle support, monitor regularly, and don't abandon lifestyle work just because the medication is doing the heavy lifting.
What real long-term users and clinicians say
The quotes below are real, attributable, and included for educational context — not as medical evidence and not as proof that anyone's results will match.
“Even after discontinuation of GLP-1s for 3 months or so, patients' journeys in treating their obesity does not stop, which is an encouraging thing to us, and also gives us a task to produce evidence-based recommendations for them in terms of what's next.”
— Dr. Hamlet Gasoyan, Cleveland Clinic Center for Value-Based Care Research, AJMC 2025 interview
“It might take a year to lose the weight, but only four months to gain it back. It's like a rubber band — you pull it hard and it snaps back quickly. If you stop taking your blood pressure medicine, what do you think happens?”
— Dr. John Morton, Yale Medicine, February 2026 patient-education piece
What patients are searching and saying
Voice-of-customer patterns from public forums — included for searcher-language insight, not as medical proof:
- "I don't think I can afford to be on it forever."
- "I'm really worried this is all for nothing."
- "$1,000 is not sustainable long term."
If those quotes describe how you feel right now, you're not alone — and the answer isn't to power through the anxiety. The answer is to plan for it. That's what the rest of this page exists for.
15 questions to ask your clinician before going long-term
A long-term GLP-1 visit shouldn't just answer “Can I have the prescription?” It should answer how long you may need it, how success is measured, what could make you stop, and what happens if cost, side effects, pregnancy, surgery, or insurance changes.
If your clinician dismisses these or doesn't have answers, that tells you something about the practice — and possibly about whether to find one with more obesity-medicine experience.
Frequently asked questions about long term GLP-1 treatment
How long do most people stay on a GLP-1?
Many people use GLP-1 medications long-term — often years — when treating chronic conditions like obesity or type 2 diabetes. The longest published randomized trial in obesity is the 4-year SELECT trial. Real-world adherence is much lower than guideline recommendations: Blue Cross Blue Shield Association research released in 2025 found nearly two-thirds of patients discontinue before the 12-week mark, and more than 40% stop after just 4 weeks.
Do you have to take GLP-1s forever?
Not always. But many people benefit from staying on a GLP-1 long-term because clinical trials show weight maintenance while treatment continues and meaningful regain after stopping. "Forever" is one of five legitimate paths — others include maintenance dosing, switching to an oral GLP-1, bridge-and-taper with structured lifestyle support, or pause-and-restart cycling.
What happens if you stop GLP-1 treatment?
Across multiple major trials, regain is common. The STEP-1 extension showed about 67% regain in 52 weeks; SURMOUNT-4 showed 14.0% regain on placebo over 52 weeks; a 2026 eClinicalMedicine meta-regression estimated about 60% of treatment-phase weight loss is regained within 12 months. Real-world data from the Cleveland Clinic suggest regain may be slower outside of trial conditions for some patients. Cardiometabolic improvements (blood pressure, lipids, blood sugar) partially reverse with regain.
Can you restart a GLP-1 after stopping?
Yes — many people do. Restart plans depend on the medication, how long you stopped, side effects, and dose history. Wegovy labeling notes that after missing 2 or more consecutive doses, clinicians may resume dosing as scheduled or restart dose escalation to reduce GI side effects.
What is a GLP-1 maintenance dose?
A GLP-1 maintenance dose is the dose your clinician keeps you on after the initial weight-loss phase to maintain your results. Per FDA labeling: Wegovy injection maintenance is 1.7 mg or 2.4 mg weekly (with up to 7.2 mg as a labeled high-dose option), Wegovy pill is 25 mg daily, Zepbound is 5/10/15 mg weekly for weight reduction (10/15 mg for OSA), and Foundayo titrates from 0.8 mg up to 17.2 mg daily. Don't lower, skip, or stretch doses on your own.
Is long-term GLP-1 treatment safe?
Across 4+ years of randomized trial data, FDA-approved GLP-1 medications have a well-characterized safety profile. Concerns about pancreatitis and pancreatic cancer have been largely dispelled by long-term cardiovascular outcome trials. The medullary thyroid cancer signal from rodent studies remains an FDA boxed warning. Long-term data past 10 years is still emerging.
Who should not take a GLP-1?
You shouldn't take a GLP-1 if you have a personal or family history of medullary thyroid carcinoma (MTC) or MEN2 — that's the FDA boxed warning. You also shouldn't take one during pregnancy (semaglutide labeling says stop at least 2 months before planned pregnancy) or with a known severe hypersensitivity reaction to that specific medication. Acute pancreatitis history, severe gastrointestinal disease, and upcoming surgery require clinician guidance.
Can you take GLP-1s during pregnancy?
GLP-1 weight-loss treatment is generally not appropriate during pregnancy. Semaglutide labeling says to stop at least 2 months before planned pregnancy. If you're planning to conceive, talk to your clinician about timing well in advance.
Can you take GLP-1s during long-term diabetes treatment?
Yes — GLP-1 medications have been studied in diabetes for over a decade with observational data extending past 10 years. Insurance and Medicare coverage for diabetes indications is much more reliable than for weight management alone.
Are compounded GLP-1s safe for long-term use?
Compounded GLP-1 products are not FDA-approved. The FDA has not verified their safety, efficacy, or quality and has issued warnings about dosing errors and unlawful online sales. The 2025 AACE algorithm advises against compounded alternatives. As of the FDA's April 2026 update, semaglutide and tirzepatide are not on the FDA shortage list, and on April 30, 2026 the FDA proposed excluding them from the 503B bulks list — meaning the regulatory pathway for compounded versions has narrowed significantly.
Will insurance cover GLP-1 treatment long-term?
It depends on your plan, diagnosis, medication, and prior authorization requirements. Coverage for type 2 diabetes, established cardiovascular disease, or obstructive sleep apnea is generally more reliable than weight management alone. Some commercial carriers tightened weight-management coverage in early 2026. The new Medicare GLP-1 Bridge offers $50/month copays through December 2027 for eligible Part D enrollees.
What if I cannot afford GLP-1 treatment forever?
Calculate 12-, 24-, and 36-month total cost — not just the first month. Then talk to your clinician about insurance coverage, comorbidity-based PA, the Medicare GLP-1 Bridge if eligible, manufacturer-direct cash pricing (Foundayo and Wegovy pill start at $149/month at the lowest doses), or — if needed — a structured bridge-and-taper plan. Cost is a legitimate reason to plan for an exit, not a reason to start without one.
Should I choose Wegovy, Zepbound, Ozempic, Mounjaro, or Foundayo for long-term treatment?
That depends on your indication, FDA approval status for your situation, insurance coverage, medical history, and clinician judgment. We have detailed comparisons for the most common matchups: Wegovy vs. Zepbound for weight loss, and Wegovy pill vs. Foundayo for oral options.
Do GLP-1s lose effectiveness over time?
Current evidence does not show GLP-1 medications losing efficacy with continued use. The plateau most people experience after several months is normal — it's the transition from active weight loss to maintenance, not drug tolerance. Continued tirzepatide treatment in SURMOUNT-4 produced an additional 5.5% weight loss after the initial 36-week loss period.
Still figuring out your long-term path?
You've read the data. You've seen the five paths. You know what 5 years of treatment really costs across every payment route. If you're still not sure which path fits your specific situation — your medication, your insurance, your state, your cost ceiling, your goals — that's exactly what our quiz is built for.
Get your personalized GLP-1 path →Six questions. A personalized 5-year plan. No commitment.
About this page
This page was researched and written by The RX Index editorial team. The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers.
How we produced this guide
We reviewed 12 primary clinical trial publications and 4 medical society guidelines, including SELECT, STEP-1 extension, STEP 4, STEP 5, SURMOUNT-1, SURMOUNT-4, SURMOUNT-MAINTAIN protocol, OASIS-4, ATTAIN-MAINTAIN, plus three meta-analyses including the 2026 eClinicalMedicine meta-regression. We pulled current 2025–2026 guidance from AACE, ACC, the WHO, the FDA, and CMS. We verified pricing on LillyDirect, NovoCare, Ro Body, and GoodRx on May 5, 2026.
Key sources cited
- Wilding et al. — STEP-1 extension, Diabetes, Obesity and Metabolism, 2022
- Aronne et al. — SURMOUNT-4, JAMA, 2024
- Horn et al. — SURMOUNT-4 post hoc, JAMA Internal Medicine, November 2025
- Lincoff et al. — SELECT, NEJM, 2023
- Ryan et al. — SELECT weight outcomes, Nature Medicine, 2024
- Colhoun et al. — SELECT kidney outcomes, Nature Medicine, 2024
- Garvey et al. — STEP 5, Nature Medicine, 2022
- Gasoyan et al. — real-world GLP-1 discontinuation, AJMC, 2025
- 2026 eClinicalMedicine meta-regression on GLP-1 cessation trajectory
- December 2025 WHO Global Guideline on GLP-1 Medicines for Obesity
- 2025 AACE Algorithm for Adiposity-Based Chronic Disease
- 2025 ACC Concise Clinical Guidance on Medical Weight Management
- FDA prescribing information via DailyMed for Wegovy, Zepbound, Mounjaro, Ozempic, Foundayo, and Wegovy HD
- FDA April 2026 updates on compounded GLP-1s, including April 30, 2026 proposed 503B bulks list exclusion
- CMS Medicare GLP-1 Bridge resource; KFF Medicaid GLP-1 Coverage Tracker (January 2026)
Medical disclaimer: This guide is informational and is not a substitute for individualized medical advice. GLP-1 medications can cause serious side effects and have specific contraindications. Discuss your situation with your prescribing clinician before starting, changing, or stopping any GLP-1 therapy.
Last verified: May 5, 2026 · Next scheduled verification: August 5, 2026
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup