Researched and written by The RX Index Editorial Team · Last verified: · Next scheduled re-verification: · Sources: FDA Access Data, DailyMed, manufacturer prescribing information, AAD, Cleveland Clinic · Editorial standards
GLP-1 Medication Side Effects — 2026 Evidence Guide
GLP-1 Hair Loss: Why It Happens, When It Stops, and What To Do Next
Published:
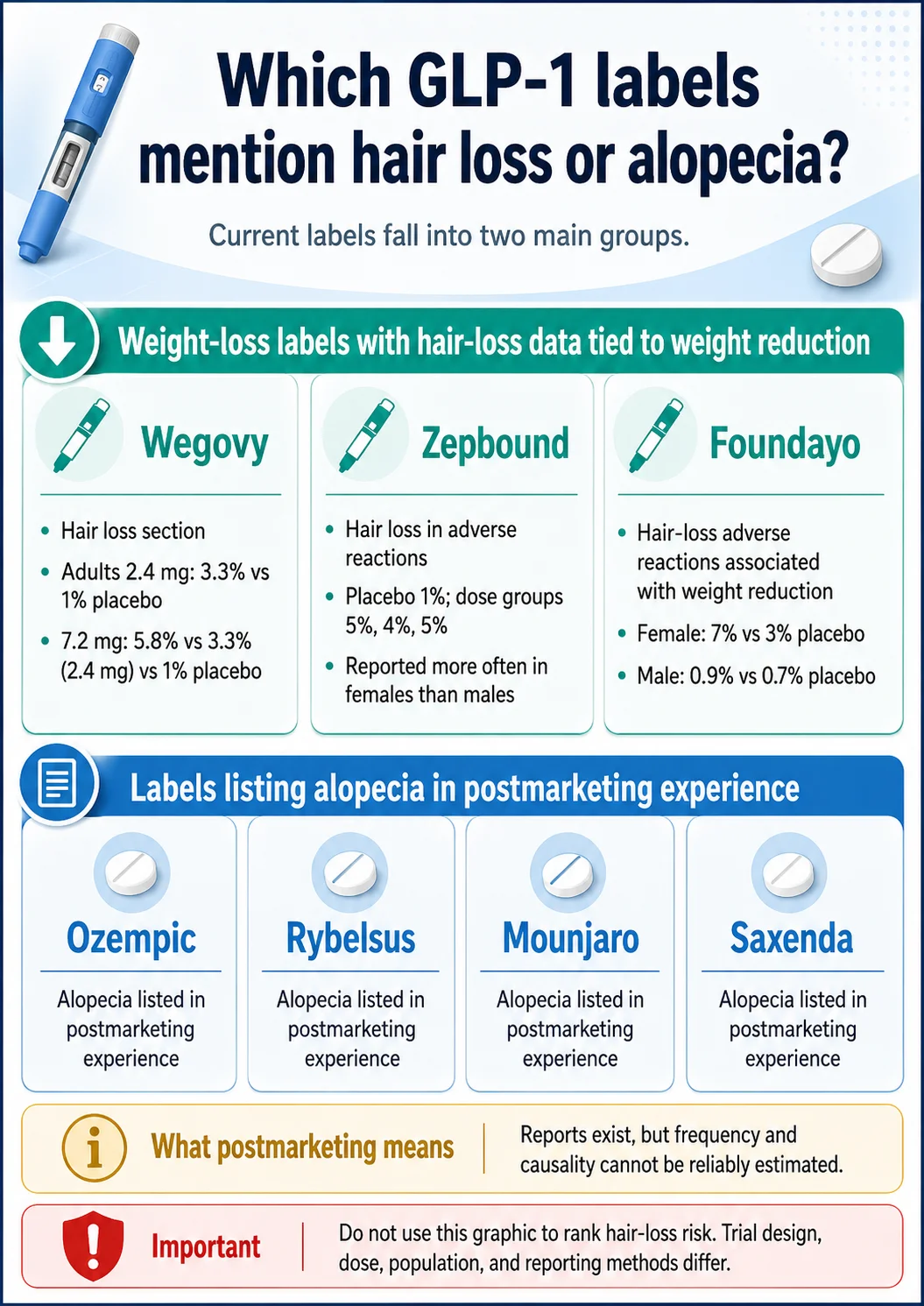
GLP-1 hair loss is usually diffuse shedding, not permanent balding — and the answer is more nuanced than “it’s not the drug.” The pattern most worth triaging first is telogen effluvium: a delayed shedding response to a body stressor like rapid weight loss, low intake, GI symptoms, illness, or dose escalation. Acute telogen effluvium resolves in roughly 95% of cases, and the American Academy of Dermatology says hair often regains fullness within 6–9 months after the trigger improves. But current FDA labels are split: Wegovy, Zepbound, and Foundayo all include hair-loss data tied to weight reduction, while Ozempic, Rybelsus, Mounjaro, and Saxenda list alopecia in postmarketing experience where frequency and causality cannot be reliably estimated. The smart move isn’t to panic-stop your medication. It’s to triage.

The 30-second triage table
| What you’re seeing | What it may mean | What to do next |
|---|---|---|
| More hair in the shower, brush, pillow, or drain 2–4 months after weight loss or a dose increase | Common telogen-effluvium pattern | Document the timeline and message your prescriber |
| Patchy bald spots, smooth round patches, scalp pain, burning, redness, scaling, or scarring | Not typical simple shedding | Book a dermatology evaluation promptly |
| Vomiting, diarrhea, dizziness, weakness, or trouble eating and hydrating | Possible nutrition or hydration issue | Contact your prescriber quickly; urgent care if severe |
| Persistent or severe abdominal pain, especially radiating to the back (with or without nausea/vomiting) | Possible GLP-1 warning sign for pancreatitis — separate from hair loss | Contact your prescriber promptly; urgent care if severe |
| Shedding continues past 6 months, or includes eyebrows or body hair | Needs evaluation | Ask for both a dermatology referral and a medical workup |
Not sure which row you’re in?
Use our free GLP-1 Hair Shedding Triage Checker to walk through your timeline, screen for red flags, and prepare a clear summary to take to your clinician.
Check My Shedding Pattern →A note on commercial transparency: The RX Index may earn compensation if you connect with certain providers through tools or links on this site. Compensation does not change our editorial guidance, and nothing here is medical advice.
What we actually verified
We built this page from primary sources, not summaries of summaries. Specifically, we pulled current public prescribing information for Wegovy, Zepbound, Foundayo, Ozempic, Rybelsus, Mounjaro, and Saxenda directly from FDA Access Data, DailyMed, and manufacturer PDFs. We cross-checked dermatology guidance from the American Academy of Dermatology and Cleveland Clinic, reviewed a 2026 systematic review on GLP-1 receptor agonists and hair-loss events, and read FDA communications on unapproved and compounded GLP-1 products — including the agency’s April 30, 2026 proposal to exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list.
We also read the forums — but only to understand how people actually search and what they’re really afraid of. We did not use forum posts as medical evidence. When you see a Reddit-style phrase quoted on this page, it’s there to validate the emotional reality of the search, not to prove a medical claim.
The evidence table further down is the heart of this page. We are not aware of another consumer resource that puts label-stated rates, postmarketing status, label version, and the date each label was checked for all seven major GLP-1s in one place.
Does GLP-1 cause hair loss, or is it rapid weight loss?
Both can be true at once. Hair loss has been reported during treatment with most GLP-1 receptor agonists, but the most common trigger to investigate first is telogen effluvium — delayed shedding caused by rapid weight loss, low food intake, dose escalation, illness, or stress. A 2026 systematic review found accumulating evidence of increased hair-loss reports with several GLP-1 agonists, especially semaglutide and tirzepatide, while noting that causality and timing still need stronger prospective research.
Which trigger fits your case?
| Trigger pattern | Typical timing | Label relevance | What to ask your prescriber |
|---|---|---|---|
| Rapid weight loss (≥20 lb / ~9 kg) | Shedding 2–4 months after the loss | Strong fit for Wegovy, Zepbound, Foundayo “associated with weight reduction” labeling | Should we slow titration or check labs? |
| Recent dose escalation | 2–3 months after the increase | Plausible for any GLP-1 | Should the next dose increase wait? |
| Persistent GI symptoms reducing intake | Variable, often within 3 months | Indirect — nutrition-mediated | Can we manage GI side effects so I can eat enough? |
| Illness, surgery, fever, postpartum | 2–3 months after the event | Independent of the medication | Do I need iron, thyroid, or other labs? |
| Eyebrow loss or patchy spots | Any timing | Not classic telogen effluvium | Can I get a dermatology referral? |
Most readers fit one or two of those rows. If you fit multiple at once, that’s not unusual — telogen effluvium often has more than one trigger stacked on top of each other.
Why the “it’s not the drug” answer is incomplete
If you’ve Googled this already, you’ve probably seen articles that confidently say GLP-1 medications don’t cause hair loss — it’s just the weight loss. That framing is partially right and partially wrong, and in 2026 it’s no longer the most accurate answer.
Here’s why. Wegovy, Zepbound, and Foundayo all explicitly list hair loss as an adverse reaction in their FDA-approved weight-management labels. Their labels also state that those reactions were associated with weight reduction. That’s not the same as saying the drug directly damages hair follicles, but it’s also not the same as saying the drug has nothing to do with it. The label is acknowledging a real signal in clinical trial data — they just stop short of declaring a follicle-toxic mechanism.
For Ozempic, Rybelsus, Mounjaro, and Saxenda, the picture is different. Their labels list alopecia (the medical term for hair loss) under “postmarketing experience.” That section captures voluntary reports submitted after approval, where frequency and causality cannot be reliably estimated. So hair loss has been reported, but the label doesn’t quantify how often or prove it’s caused by the medication.
Why rapid weight loss alone can trigger shedding
Telogen effluvium, in plain language: your hair has a growth cycle, and a major body stressor can suddenly push a bunch of hairs into the resting/shedding phase at once. The catch is that the shedding doesn’t show up immediately — it usually appears 2 to 3 months after the trigger. By the time you notice hair in the drain, the actual cause was something that happened a few months earlier.
The American Academy of Dermatology lists losing 20 pounds or more as a known trigger for excessive shedding, alongside surgery, high fever, severe illness, childbirth, and significant stress. Cleveland Clinic describes telogen effluvium as a common, usually temporary response to that kind of bodily change. If you’ve lost weight quickly on a GLP-1, you’ve handed your hair a textbook trigger.
Why slow weight loss can still come with shedding
Some people shed even without dramatic rapid loss. Common contributors:
- Lower protein and calorie intake (very easy on a GLP-1, because the drug works by suppressing appetite)
- Persistent GI side effects that quietly reduce intake
- Iron deficiency or low ferritin
- Thyroid issues
- Vitamin D, B12, or zinc shortfalls
- Other medications
- An underlying hair condition (like androgenetic alopecia) that gets unmasked when total density drops
The honest version: Anyone who tells you “GLP-1s cannot be involved in hair loss” is oversimplifying. The better question — the one that actually helps you decide what to do — is whether your shedding pattern fits telogen effluvium, whether your specific medication’s label includes a hair-loss signal, and whether you have any red flags that need a clinician’s eyes on them.
Which GLP-1 medications actually list hair loss or alopecia in the label?
Current labels split into two groups. Wegovy, Zepbound, and Foundayo include trial-rate hair-loss data tied to weight reduction. Ozempic, Rybelsus, Mounjaro, and Saxenda list alopecia under postmarketing experience, where frequency and causality cannot be reliably estimated. That distinction matters: trial-rate data tells you what showed up in controlled studies; postmarketing data only confirms reports exist.
Below is our proprietary evidence matrix. Every row was pulled directly from the current FDA label PDF or DailyMed entry. The percentages are not comparable across drugs — different populations, different trial designs, different doses, different reporting methods. This is a counseling and triage tool, not a head-to-head ranking.
The RX Index GLP-1 Hair Loss Evidence Matrix
| Medication | What the current label says | Numbers or status | Practical interpretation | Source checked |
|---|---|---|---|---|
| Wegovy (semaglutide 2.4 mg / 7.2 mg) | Includes a specific “Hair Loss” section. States hair-loss adverse reactions were associated with weight reduction. | Adult 2.4 mg: 3.3% vs 1% placebo. 7.2 mg trial: 5.8% vs 3.3% (2.4 mg) vs 1% placebo. Pediatric: 4% vs no placebo patients. In the 7.2 mg group, 1 hair-loss event led to permanent discontinuation, 1 to temporary interruption, and 5 to dose reduction. | Real labeled signal in the weight-management data. The 7.2 mg detail tells you hair loss can be significant enough for treatment changes — but only in a small minority. | FDA label, checked 4/30/2026 |
| Zepbound (tirzepatide) | Includes hair loss in adverse reactions. States reactions were associated with weight reduction. | Placebo: 1%. Zepbound dose groups: 5%, 4%, and 5%. Female patients reported more hair loss than males. No Zepbound-treated patients discontinued because of hair loss in the cited section. | Label-recognized signal in the weight-loss treatment context, with a clear sex skew toward female patients. | Zepbound USPI, checked 4/30/2026 |
| Foundayo (orforglipron) | Label states hair-loss adverse reactions were associated with weight reduction. | Female: 7% Foundayo vs 3% placebo. Male: 0.9% Foundayo vs 0.7% placebo. | Newer drug — re-verified monthly. Hair loss is a visible counseling point, especially for women. | Foundayo label, checked 4/30/2026 |
| Ozempic (semaglutide injection, diabetes label) | Lists alopecia in postmarketing experience. | Postmarketing reports are voluntary. Frequency and causality cannot be reliably estimated. | Hair loss has been reported, but no clean trial-rate claim like Wegovy. | Ozempic label, checked 4/30/2026 |
| Rybelsus (oral semaglutide) | Lists alopecia in postmarketing experience. | Postmarketing status, not a frequency estimate. | Treat as a possible reported signal, not proof oral semaglutide directly causes shedding. | Rybelsus label, checked 4/30/2026 |
| Mounjaro (tirzepatide, diabetes label) | Lists alopecia in postmarketing experience. | Postmarketing reports cannot reliably establish frequency or causality. | Mounjaro’s diabetes label is different from Zepbound’s weight-loss label. Don’t assume the same trial-rate context applies. | Mounjaro USPI, checked 4/30/2026 |
| Saxenda (liraglutide) | Lists alopecia in postmarketing experience. | Postmarketing status, not a trial-rate estimate. | Saxenda users can still experience shedding, but the label evidence isn’t the same as the Wegovy/Zepbound/Foundayo hair-loss sections. | Saxenda label, checked 4/30/2026 |
Why postmarketing reports aren’t the same as trial rates
This is the distinction that confuses most articles, so let’s be precise about it. Trial-rate data comes from controlled studies where researchers actively measure adverse events in both the treatment and placebo groups. That’s how you get a number like “3.3% vs 1% placebo.” Postmarketing reports are voluntary submissions made after a drug is approved — by patients, providers, or manufacturers. The FDA collects them, but no one knows how many cases never got reported, and there’s no placebo group. So when a label says alopecia is in postmarketing experience, it means: “people have reported this; we can’t tell you how often or whether the drug caused it.”
That’s why Wegovy’s “3.3%” sits in a different evidence tier than Ozempic’s postmarketing alopecia listing — even though both are forms of semaglutide.
Why Wegovy, Zepbound, and Foundayo deserve special attention here
Most readers who land on this page are taking a GLP-1 for weight loss. The Wegovy, Zepbound, and Foundayo labels speak directly to that use case and explicitly discuss hair-loss adverse reactions in the weight-reduction setting. If you’re taking one of these three, the label is essentially saying: yes, this can happen, and it tracks with how much weight you’re losing.
Why this table shouldn’t be used to “rank” hair-loss risk
We’ve watched competitor articles try to turn data like this into a leaderboard. Don’t. The trial populations differ. The doses differ. The indication (diabetes vs. obesity) differs. The reporting method differs. A 3.3% in one trial isn’t directly comparable to a 5% in another. Use this matrix to understand your medication, not to grade it against another.
What does GLP-1 hair loss usually look like?
The classic pattern is diffuse shedding — more hair everywhere, your ponytail feeling thinner, the drain filling faster — rather than a single clean bald patch. A normal-looking scalp without pain, redness, scaling, or scarring is more consistent with simple telogen effluvium than a primary scalp disease. Telogen effluvium often shows up a few months after the trigger, which is why people frequently blame this week’s dose when the actual cause was earlier weight loss, illness, or under-eating.
Diffuse shedding vs. patchy loss
Three patterns to know:
Diffuse shedding.
More hair across the whole scalp. You notice it in the shower, on the brush, on the pillow, in the drain. Your part might look slightly wider. Your ponytail feels thinner. There aren’t bald spots — just less density everywhere. This is the classic GLP-1 / weight-loss pattern.
Patchy loss.
Round, smooth, sharply defined bald spots. This isn’t telogen effluvium. The most common cause of round, smooth patches is alopecia areata, an autoimmune condition that needs dermatology evaluation.
Scalp symptoms.
Pain, burning, redness, scaling, sores, or visible scarring. None of these are normal shedding. They suggest a primary scalp condition that needs to be diagnosed and treated, ideally by a dermatologist.
Why it shows up months after the trigger
This is the most counterintuitive part of telogen effluvium and the reason so many people misidentify the cause. The trigger event happens. Your hair cycle shifts in response. The hairs that were pushed into the shedding phase don’t fall out immediately — they fall out 2 to 3 months later.
So if you started a GLP-1 in January, escalated your dose in February, lost 15 pounds by March, and noticed shedding in April or May — the shedding is real, but the cause was the cumulative stressor weeks earlier. People often start blaming whatever happened in the last week, which is a dead end.
How people actually describe it
We searched public forums and saw the same phrases over and over: “hair clumps in shower,” “hair shedding like CRAZY,” “Will it stop? Will it grow back? Or should I stop the med?” These quotes aren’t medical evidence. We’re including them because they capture the real emotional state behind the search, and because if you’ve felt that way, you should know you’re not the only one feeling it.
Is GLP-1 hair loss permanent, and when does it grow back?
If the pattern is telogen effluvium, it’s almost always temporary. The American Academy of Dermatology says excessive shedding after a trigger is temporary and hair often regains fullness within 6–9 months. Cleveland Clinic says telogen effluvium often grows back in 3–6 months once the trigger is corrected, and resolves in roughly 95% of acute cases. The catch is that “temporary” doesn’t mean “ignore it” — and density recovery often takes longer than the shedding itself.
The practical timeline
Here’s the sequence dermatology guidance describes:
- Trigger. Weight loss, dose escalation, low intake, illness, surgery, fever, postpartum, thyroid or iron issue, major stress.
- Delay (months 0–3 after trigger). Nothing visible while the hair cycle shifts.
- Active shedding (months 3–6). More hair in the shower, brush, drain, pillow.
- Stabilization. The trigger improves — you stop losing weight rapidly, your intake normalizes, your dose stabilizes. Shedding slows.
- Regrowth (typically by months 6–9). Short, fine new hairs appear along the part line and at the temples. They look like baby hairs, but they’re a good sign.
- Density recovery. Months longer than shedding itself. Hair grows roughly half an inch per month, so getting back to your prior length and visual density takes patience.
Why “temporary” doesn’t mean “ignore it”
Two reasons. First, the emotional weight is real. Shedding is visible, personal, and exhausting. “It’ll grow back in nine months” is medically reassuring and emotionally insufficient. Second, telogen effluvium can be a symptom of something else that does need treatment — under-eating, iron deficiency, thyroid disease, or another medication interaction. Treating the shedding as automatic and benign can mean you miss the underlying issue.
When it might not be telogen effluvium
If your shedding includes any of these, telogen effluvium is probably not the full story:
- Patchy or scarring loss
- Eyebrow or body-hair loss
- Scalp pain, redness, burning, scaling, or sores
- Shedding that continues past 6 months
- A family history of pattern hair loss that’s now becoming visible
- New or worsening thyroid, autoimmune, or iron-related symptoms
- A recent change in another medication
Each of those calls for medical evaluation, not just patience.
What should you do now if your hair is shedding on a GLP-1?
Don’t stop your medication on your own. Document the timeline, screen for red flags, message your prescriber with specifics, and ask whether nutrition, labs, dose pace, or a dermatology referral are appropriate. The single most useful thing you can do today is write down dates and dose changes — that information will determine whether your clinician treats this as routine telogen effluvium or as something that needs further workup.
Step 1 — Write down the timeline
Pull up your notes app and write:
- The date you started the medication
- The medication name and dose
- Every dose increase and the date
- How much weight you’ve lost and over what timeframe
- The week you first noticed increased shedding
- Any GI side effects (nausea, vomiting, diarrhea, constipation, food aversions)
- Any illness, surgery, fever, postpartum event, or major stress in the months before shedding
- Any new medications, including supplements
This is the document you’ll send your prescriber. It’s worth more than a vague “my hair is falling out.”
Step 2 — Run the under-fueling self-audit
GLP-1s suppress appetite. That’s the mechanism. The downside is that it’s very easy to slide into unintentional under-eating, which is one of the most common stackable triggers for shedding. Check yourself against this list:
- I’ve been skipping meals because nothing sounds good
- My protein intake has dropped from where it used to be
- I’ve had vomiting, diarrhea, or significant nausea in the last month
- Most foods feel slightly aversive
- I’ve lost weight faster than I planned to
- I’m noticeably more fatigued or lightheaded than usual
- My most recent dose increase was within the last 8 weeks
If you’re nodding to three or more of those, your prescriber needs that picture before they can give you good advice.
Step 3 — Screen for red flags before assuming it’s normal
Use the red-flag table further down. If any apply, your next message isn’t a casual portal note — it’s a phone call.
Step 4 — Message your prescriber with specifics
Here’s a template you can copy and adapt:
“I’m taking [medication and dose] and started noticing increased hair shedding around [date]. I started the medication on [date], increased my dose on [date], and have lost about [amount] over [timeframe]. The shedding pattern is [diffuse / patches / with scalp symptoms]. Could we review whether this fits telogen effluvium, whether my weight-loss pace or intake needs adjustment, and whether labs or a dermatology referral are appropriate? I’m not planning to stop the medication on my own — I want to figure out the right plan with you.”
Step 5 — Ask whether labs are appropriate
Don’t demand labs. Don’t assume you need them. But it’s reasonable to ask your clinician whether any of the following make sense given your history:
- CBC (complete blood count)
- Ferritin and iron studies
- Thyroid testing such as TSH
- Vitamin D
- B12
- Zinc
The right panel depends on your symptoms, intake, and medical history. A clinician decides — not Reddit.
Step 6 — Ask whether the dose pace should change
Not “should I lower my dose” — that’s their decision. Ask: “If shedding started after rapid loss or my last dose increase, is it worth slowing the next titration?” Some clinicians will adjust pace. Some won’t. Either way, you’ve raised the right question.
Step 7 — Decide whether dermatology should be involved
A dermatologist is especially relevant if:
- The loss is patchy or scarring
- You have scalp symptoms (pain, redness, scaling)
- Shedding has continued more than 6 months
- You’re losing eyebrows or body hair
- The emotional impact is significant and you want a faster, more focused workup
You don’t usually need your prescriber’s permission to book a dermatology consult. Many people see both clinicians in parallel.
Want help organizing your timeline before you message your prescriber?
Run it through our free GLP-1 Hair Shedding Triage Checker and walk away with a clear summary you can copy into your patient portal.
Create My Hair Shedding Action Plan →Should you stop your GLP-1 because of hair loss?
Hair shedding alone is usually not a reason to self-stop a GLP-1, especially if the medication is treating obesity, diabetes, cardiovascular risk, or another serious condition. The better question is: what trigger can be identified and reduced without abruptly stopping treatment? Stopping abruptly creates a second problem on top of the first.
Why self-stopping can backfire
Depending on why you were prescribed a GLP-1 in the first place, abruptly stopping can affect:
- Weight regain trajectory
- Glucose control
- Appetite regulation and food noise
- Cardiovascular risk reduction
- Treatment continuity if you need to restart later
If your prescriber decides a pause is appropriate, that’s a different decision than you stopping mid-cycle without telling anyone. The first is medical management; the second is a setback you’ll often regret.
The escalation ladder, from low to high effort
Match your action to what you’re seeing:
- Patient portal message — for routine diffuse shedding, no red flags, you just want to document it and ask a question.
- Phone call to your prescriber — when you’re losing weight faster than planned, can’t eat enough, or shedding is getting worse week over week.
- Dermatology referral — patchy loss, scalp symptoms, scarring, eyebrow loss, or shedding past 6 months.
- Urgent care — severe abdominal pain, persistent vomiting/diarrhea, dehydration symptoms, fainting.
Most readers stop at level 1 or 2. Knowing what level 3 and 4 look like means you won’t miss them when they apply.
When stopping or changing therapy may genuinely be on the table
There are real situations where stopping or switching is reasonable. Discuss with your clinician if you have:
- Severe, persistent, or worsening shedding past 6 months
- Inability to eat enough at your current dose
- Ongoing vomiting or diarrhea you can’t manage
- Dehydration symptoms
- Severe emotional distress about the hair loss
- A suspected non-telogen-effluvium cause (alopecia areata, scarring alopecia, etc.)
- A clinician’s risk/benefit decision based on your overall picture
One honest admission
Hair shedding can be emotionally devastating even when it’s medically temporary. If your current GLP-1 program — whether telehealth, in-person, or a compounding pharmacy — won’t engage seriously with side effects, that’s the wrong level of support for you. Some programs are built for low-touch refills. They’re efficient and cheap, and that’s fine for some people. But if you need a clinical relationship that takes a hair-loss complaint seriously, talks about labs, and adjusts your titration, you deserve that. It’s not vanity. It’s medicine.
If your current program won’t help you evaluate side effects:
Take our free 60-second matching quiz to find a GLP-1 path with the level of clinical support you actually want.
Find My GLP-1 Support Path →How can you reduce the risk of hair shedding while staying on track?
You can’t guarantee prevention, but you can reduce the most common triggers: too-fast weight loss, crash dieting, low protein intake, untreated nutritional deficiencies, dehydration, and unmanaged GI symptoms. Supplements may help only when they correct an actual deficiency or are recommended by a clinician — they aren’t a universal fix for telogen effluvium.
Avoid stacking deficits on top of the medication
GLP-1s suppress appetite. That’s the point. Adding an aggressive dietary restriction on top can push your total deficit far past what your body is set up to handle. The American Academy of Dermatology lists losing 20 pounds or more as a known shedding trigger — the point isn’t an exact monthly number, it’s that compounding deficits stack a known hair-shedding trigger on top of appetite suppression. We’re not telling you to slow down weight loss; we’re telling you that aggressive deficits add a real risk you may not have been planning for.
Ask about protein and nutrient adequacy
We’re not going to throw out a generic protein number on a YMYL page. Ask your clinician or a registered dietitian what daily protein and calorie range fits your body, your medication, and your medical history. If you’re losing weight on a GLP-1 and barely eating, you almost certainly aren’t getting enough protein, and your hair, muscle mass, and energy will all pay the price together.
Treat GI side effects early instead of riding them out
Persistent nausea, vomiting, diarrhea, constipation, or food aversion will quietly torpedo your nutrition. The fix isn’t to white-knuckle through it. Tell your prescriber early. Most GI symptoms have manageable solutions — slower titration, anti-nausea support, dietary adjustments, hydration strategies, or in some cases a medication change.
Be careful with hair supplements
The supplement industry has noticed the GLP-1 wave and is selling hard. Biotin, collagen, Nutrafol-style products, rosemary oil, “GLP-1 hair regrowth” stacks — you’ll see them everywhere. A few honest realities:
- Supplements help when they correct a real deficiency. They generally don’t help when nutrition is adequate.
- Biotin can interfere with certain lab tests and cause incorrect results, so always tell the clinician ordering bloodwork that you’re taking it.
- High-dose anything during pregnancy, breastfeeding, or alongside other medications needs a clinician’s review.
- “Will fix your hair” claims on social media are advertising, not evidence.
If you suspect a deficiency, ask for the lab. If the lab confirms it, treat it under medical guidance. That sequence is more useful than guessing your way through the supplement aisle.
Ask whether minoxidil is appropriate for you
Topical minoxidil is sometimes used for telogen effluvium and is well-studied for pattern hair loss. It isn’t a universal fix for GLP-1 shedding, and it’s not a substitute for figuring out the actual trigger, but it’s a reasonable conversation to have with a dermatologist or clinician — especially if you have a family history of pattern hair loss or your shedding is dragging on.
When is hair loss on a GLP-1 a red flag?
Patchy loss, round bald spots, scarring, scalp pain or burning, redness, scaling, eyebrow or body-hair loss, shedding that continues past 6 months, severe fatigue, dizziness, persistent or severe abdominal pain, or inability to eat or hydrate are red flags that warrant prompt evaluation. Telogen effluvium is common and usually benign, but assuming every shed is temporary can cause you to miss other diagnoses.
Red-flag table
| Red flag | Why it matters | Next step |
|---|---|---|
| Round or patchy bald spots | Could be alopecia areata or another non-TE condition | Dermatology |
| Scalp pain, burning, redness, scaling, scarring, or sores | Not typical simple shedding | Dermatology promptly |
| Eyebrow or body-hair loss | May signal a broader hair disorder or systemic issue | Medical evaluation |
| Shedding beyond 6 months | May not be acute telogen effluvium | Prescriber + dermatology |
| Severe fatigue, dizziness, weakness | Could reflect under-fueling, anemia, dehydration, thyroid, or another issue | Prescriber promptly |
| Vomiting or diarrhea, or inability to eat or hydrate | Medication tolerance and nutrition issue | Prescriber quickly; urgent care if severe |
| Persistent or severe abdominal pain, especially radiating to the back, with or without nausea/vomiting | GLP-1 labels warn this can be a sign of acute pancreatitis | Contact prescriber promptly; urgent care if severe |
| Pregnancy or postpartum context | Common TE trigger, but needs individualized care | OB/GYN or clinician |
If you’re seeing more than one of these together — say, patchy loss plus persistent fatigue plus inability to eat — escalate. Don’t wait for your next scheduled appointment.
What if you’re using compounded or unapproved GLP-1 medication?
The hair-shedding triage above is the same. But the medication source itself is a separate safety issue worth flagging. The FDA has warned about unapproved GLP-1 products sold online, products falsely labeled “for research use only” or “not for human consumption,” and compounded drugs that aren’t FDA-approved.
Current FDA status to know — April 30, 2026
On April 30, 2026, the FDA proposed to exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list, stating it had not identified a clinical need for outsourcing facilities to compound those drugs from bulk substances. The agency is taking public comments through June 29, 2026. This is a proposed action, not a final rule. If finalized, it would change which compounding facilities can produce these GLP-1s from bulk active ingredients.
If you’re currently sourcing a compounded GLP-1, this development is worth tracking with your provider. We’ll update this section as the comment period closes and any final decision is made.
A note on language we won’t use
You’ll see compounded GLP-1 products marketed in ways that blur the line with FDA-approved drugs. We’re going to be precise: compounded medications are not FDA-approved. They may be appropriate in specific circumstances under applicable pharmacy and prescriber rules, but they should not be described as generic versions of FDA-approved GLP-1s, and we won’t tell you they’re “the same active ingredient” or “clinically proven” — those phrases don’t accurately describe how compounded products are evaluated.
That precision matters here because if your shedding is severe, your nutrition is collapsing, or you’re seeing red-flag symptoms, the questions you ask should include where your medication actually came from.
Source questions to ask
- Who prescribed it? Are they licensed in your state?
- Which pharmacy dispensed it? Is it state-licensed?
- What exact formulation are you taking, and what’s in it beyond the active ingredient?
- What clinical follow-up does the program offer for side effects?
- Who do you call if you develop persistent vomiting, dehydration, or severe shedding?
- If you needed to stop or switch, what’s the process?
If you can’t answer those questions about your current source, that’s information. For more, see our guide on compounded GLP-1 availability in 2026.
Not sure whether your current GLP-1 path has enough clinical support?
Take our free matching quiz and compare next-step options with the level of clinical support you want.
Check My GLP-1 Path →What this page does, and what it doesn’t
This page is a decision-support resource, not a diagnosis. It uses official labels and dermatology guidance to help you decide what to ask your clinician next. It can’t tell you the exact cause of your hair loss without a medical evaluation, and it won’t try to.
Our source hierarchy
- FDA / DailyMed / manufacturer prescribing information
- Dermatology and medical institution guidance (American Academy of Dermatology, Cleveland Clinic)
- Peer-reviewed systematic review evidence
- FDA communications and public regulatory actions
- Forums and Reddit — used only for voice-of-customer language, never as medical evidence
What this page won’t do
- Diagnose your hair loss
- Tell you to stop your medication
- Rank GLP-1s by hair-loss risk
- Claim compounded drugs are FDA-approved
- Sell you supplements
- Use forum anecdotes as proof of medical claims
Frequently asked questions
Can GLP-1 cause hair loss?▾
Hair loss has been reported or labeled with several GLP-1 receptor agonists, but most cases appear related to weight loss, reduced intake, or telogen effluvium rather than direct follicle damage. The safest answer is that hair loss can occur during GLP-1 treatment and should be triaged based on your timing, pattern, symptoms, and nutrition. If shedding is severe, patchy, painful, or persistent, contact a clinician.
Does Ozempic cause hair loss?▾
Ozempic's current FDA label lists alopecia under postmarketing experience, where frequency and causality cannot be reliably estimated. That means hair loss has been reported by users since approval, but the label does not provide a trial-rate percentage and does not establish that Ozempic directly causes hair loss in a predictable share of patients.
Does Wegovy cause hair loss?▾
Wegovy's FDA label includes a specific hair-loss section and states that hair-loss adverse reactions were associated with weight reduction. In adult 2.4 mg trials, hair loss was reported in 3.3% of Wegovy patients versus 1% of placebo patients. The 7.2 mg dose trial reported 5.8%. In the 7.2 mg group, one event led to permanent discontinuation, one led to temporary interruption, and five led to dose reductions. The label ties these reactions to weight reduction rather than direct follicle damage.
Does Zepbound cause hair loss?▾
Zepbound's FDA label includes hair loss in adverse reactions and states reactions were associated with weight reduction. Trial data show hair loss in 1% of placebo patients versus 4–5% across Zepbound dose groups, with a higher rate in female than male patients. The label notes no Zepbound-treated patients in the cited section discontinued treatment because of hair loss.
Does Mounjaro cause hair loss?▾
Mounjaro's FDA label lists alopecia under postmarketing experience, where voluntary reports cannot reliably estimate frequency or prove causality. Mounjaro is approved for type 2 diabetes; tirzepatide is also marketed as Zepbound for chronic weight management. If you're using Mounjaro for weight loss specifically, the Zepbound label data may be a more relevant reference for counseling.
Does Foundayo cause hair loss?▾
Foundayo's FDA label states that hair-loss adverse reactions were associated with weight reduction. Female patients reported hair loss at 7% on Foundayo vs 3% on placebo, while male patients reported 0.9% on Foundayo vs 0.7% on placebo. Because Foundayo (orforglipron) is newer, this section is re-verified monthly.
Does Saxenda cause hair loss?▾
Saxenda's current label lists alopecia under postmarketing experience, not as a trial-rate adverse event. That means hair loss has been reported by users, but the label doesn't quantify it the way Wegovy's, Zepbound's, or Foundayo's labels do.
Is GLP-1 hair loss permanent?▾
If your pattern is telogen effluvium, it's almost always temporary. The American Academy of Dermatology says excessive shedding after a trigger is temporary and fullness often returns within 6–9 months. Cleveland Clinic states regrowth often happens 3–6 months after the trigger is corrected and that acute telogen effluvium resolves in roughly 95% of cases. Density recovery typically takes longer than the active shedding phase.
When does GLP-1 hair loss start?▾
Telogen effluvium usually appears 2 to 3 months after the trigger, which makes the timing confusing. Many people first notice shedding in months 3 through 6 of GLP-1 treatment, even though the actual trigger was earlier weight loss, dose escalation, reduced intake, illness, or stress.
Should I stop my GLP-1 if my hair is falling out?▾
Don't stop on your own. Message your prescriber with your medication, dose, weight-loss timeline, shedding pattern, and any associated symptoms so they can help decide whether nutrition adjustments, labs, dose-pace changes, or a dermatology referral are appropriate. Self-stopping mid-treatment can create new problems, including weight regain or loss of glucose control, depending on why you were prescribed the medication.
How much hair shedding is normal?▾
The American Academy of Dermatology says it's normal to shed about 50–100 hairs per day. Excessive shedding means a clearly noticeable increase — significantly more hair in the shower, on the brush, on your pillow, or in the drain than you're used to. Counting individual hairs isn't useful; pattern recognition is.
What labs should I ask about?▾
Ask your clinician whether labs such as a CBC, ferritin and iron studies, thyroid testing (TSH and others as indicated), vitamin D, B12, or zinc are appropriate given your specific situation. Don't self-diagnose a deficiency or start high-dose supplements without medical guidance — some can interfere with lab interpretation or other medications.
Do supplements stop GLP-1 hair loss?▾
Supplements can help when they correct an actual deficiency. They're generally not a guaranteed fix for telogen effluvium or medication-associated shedding when nutrition is already adequate. If shedding is severe, patchy, painful, prolonged, or emotionally distressing, medical evaluation matters more than guessing at supplements.
Does minoxidil help GLP-1 hair loss?▾
Topical minoxidil is well-studied for some types of hair loss and is sometimes used as part of a telogen effluvium plan, especially when an underlying pattern hair loss is also present. It isn't a universal answer for every GLP-1 shedding pattern. Ask a dermatologist or clinician before starting if you're unsure whether it fits your situation.
Still figuring out the right GLP-1 path?
If you’ve worked through this page and you’re realizing your current GLP-1 program — whatever it is — isn’t giving you the side-effect support you need, that’s worth acting on. The wrong program treats hair loss as a complaint to dismiss. The right program treats it as a signal to investigate.
Still not sure which GLP-1 program is right for you?
Take our free 60-second matching quiz and get a personalized action plan.
About this guide
By The RX Index Editorial Team
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. This guide was produced by reviewing current public prescribing information for Wegovy, Zepbound, Foundayo, Ozempic, Rybelsus, Mounjaro, and Saxenda; dermatology guidance from the American Academy of Dermatology and Cleveland Clinic; FDA communications on unapproved and compounded GLP-1 products, including the April 30, 2026 503B bulks list proposal; a 2026 systematic review on GLP-1 receptor agonists and hair-loss events; and public search-language patterns used for voice-of-customer accuracy only.
This page is a decision-support resource, not a substitute for medical diagnosis or treatment. We update label citations on a quarterly cadence — and immediately following major FDA or manufacturer updates. The “Last verified” date at the top of this page reflects our most recent re-check.
Commercial disclosure. The RX Index may earn compensation when you connect with certain providers through tools or links on this site. Compensation does not change our editorial guidance, and our medication evidence matrix is built strictly from primary regulatory sources.
If you spot something that needs updating, we want to know. Editorial corrections improve the page for the next person who searches “GLP-1 hair loss” while panicked at 11 p.m. with hair on their pillow — and that’s exactly who we built this for.
Last updated: · Sources: CMS, FDA Access Data, DailyMed, AAD, Cleveland Clinic · Editorial standards
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup