GLP-1 Pipeline Tracker · Verified April 16, 2026
Next-Generation GLP-1 Drugs Coming Soon: What’s Actually Next in 2026
Published: · Last updated:
If you’re researching next-generation GLP-1 drugs coming soon, here’s the part most articles bury: two of the “future” drugs people keep asking us about are already here. The Wegovy pill launched in January 2026. Foundayo — Eli Lilly’s once-daily pill — was approved April 1, 2026. The one true next-wave obesity drug actually filed with the FDA right now is CagriSema. And the one everyone’s most excited about — retatrutide, with 28.7% weight loss in Phase 3 — is still in clinical trials, with launch realistically 18 to 24 months away or more.
So should you wait? For most people, no. We’ll show you exactly why — every drug in the pipeline, the real timelines, a decision framework for your situation, and what to do this week if you’ve already decided to stop waiting.
This page is an informational tracker, not a provider sales pitch. Our goal is for you to leave knowing exactly where every major next-generation GLP-1 stands today and what the right move is for you.
What we actually verified for this page
Everything below was cross-checked against primary sources on April 16, 2026:
- FDA press releases and approval letters for the three recent approvals (Wegovy pill, Wegovy HD, Foundayo)
- Eli Lilly investor communications (TRIUMPH-4 results, TRANSCEND-T2D-1 results, Foundayo launch, retatrutide status page)
- Novo Nordisk press releases (Wegovy pill launch, Wegovy HD approval, CagriSema NDA filing, REDEFINE 1/2/4 results)
- NovoCare’s current published price guide for Wegovy products
- Amgen newsroom and the New England Journal of Medicine publication for MariTide Phase 2
- Viking Therapeutics investor updates for VK2735 (VENTURE Phase 2 and VANQUISH Phase 3)
- ClinicalTrials.gov for every Phase 3 trial listed
- The FDA’s consumer advisory on unapproved GLP-1 drugs sold online
- CMS’s official Medicare GLP-1 Bridge program page
Where a number or status couldn’t be confirmed through a primary source, we say so. This page is re-verified monthly.
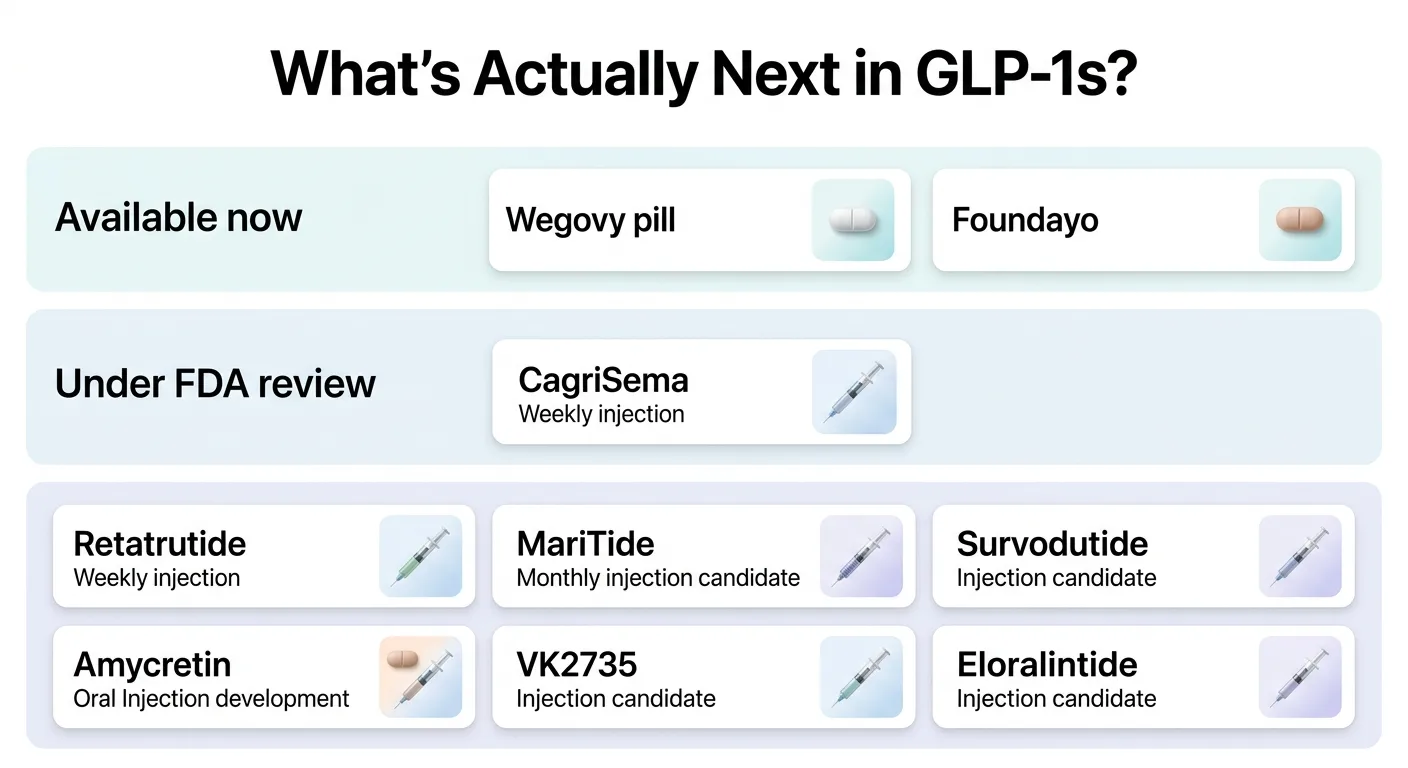
The next-generation GLP-1 pipeline, in three honest buckets
Answer capsule: Ten major next-generation GLP-1 candidates are either already approved or in late-stage development as of April 2026. Three have been FDA-approved in the past four months and are prescribable today. One is under FDA review. The rest are still in Phase 3 or earlier, with consumer availability estimated between late 2027 and 2029 based on current trial stages.
Most “coming soon” explainers lump every drug into one bucket and leave readers to sort it out. We don’t. Here’s the same pipeline sorted by how close each drug actually is to a legal prescription in your hand.
Bucket 1: Already here (available now)
| Drug | Company | Route | Approved | Peak Weight Loss | Self-Pay Starting Price |
|---|---|---|---|---|---|
| Wegovy pill (oral semaglutide 25 mg) | Novo Nordisk | Daily tablet | Dec 22, 2025 | 16.6% at 64 weeks (OASIS 4, adherent) | From $149/mo |
| Wegovy HD (semaglutide 7.2 mg injection) | Novo Nordisk | Weekly injection | Mar 19, 2026 | 20.7% at 72 weeks (STEP UP, efficacy estimand) | $399/mo per NovoCare |
| Foundayo (orforglipron) | Eli Lilly | Daily tablet | Apr 1, 2026 | 12.4% at 72 weeks (highest dose) | From $149/mo |
Bucket 2: Closest true next-wave drug (filed, under FDA review)
| Drug | Company | Route | Status | Peak Weight Loss | Editorial Timing Estimate |
|---|---|---|---|---|---|
| CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg) | Novo Nordisk | Weekly injection | NDA filed Dec 18, 2025 | 22.7% at 68 weeks (REDEFINE 1, trial product estimand) | Late 2026 – early 2027 if approved |
Bucket 3: Watch list (still in trials — not a current access path)
| Drug | Company | Mechanism | Phase | Peak Weight Loss | Editorial Timing Estimate |
|---|---|---|---|---|---|
| Retatrutide | Eli Lilly | Triple agonist (GLP-1 + GIP + glucagon) | Phase 3 | 28.7% at 68 weeks (TRIUMPH-4, 12 mg) | Late 2027 – 2028 |
| MariTide (maridebart cafraglutide) | Amgen | GLP-1 agonist + GIP antagonist (monthly) | Phase 3 | Up to 20% at 52 weeks (Phase 2) | 2028 or later |
| Amycretin (SC) | Novo Nordisk | GLP-1 + amylin (single molecule, injection) | Phase 3 starting Q1 2026 | 22% – 24.3% at 36 weeks (Phase 1b/2a) | 2028 – 2029 |
| Amycretin (oral) | Novo Nordisk | GLP-1 + amylin (single molecule, pill) | Phase 3 starting Q1 2026 | 13% at 16 weeks (Phase 1) | 2028 – 2029 |
| Survodutide | Boehringer Ingelheim / Zealand | GLP-1 + glucagon dual agonist | Phase 3 | Phase 3 readouts pending | 2027 earliest |
| Eloralintide | Eli Lilly | Amylin analog | Phase 3 advancing | Up to ~20% (Phase 2) | 2027 – 2028 |
| VK2735 (SC) | Viking Therapeutics | GLP-1 + GIP dual agonist | Phase 3 (VANQUISH-1, VANQUISH-2) | 14.7% at 13 weeks (Phase 2) | 2028 or later |
| VK2735 (oral) | Viking Therapeutics | GLP-1 + GIP dual agonist | Earlier-phase oral program | Preliminary | Later than SC formulation |
Timing estimates are The RX Index’s editorial judgment based on each drug’s current trial stage, published company guidance, and standard FDA review timelines. They are not manufacturer promises.
How to read this table: If a drug is in Bucket 3, you cannot legally obtain it from a pharmacy — full stop. Anyone selling it outside an authorized clinical trial is operating outside FDA regulation. More on that below.
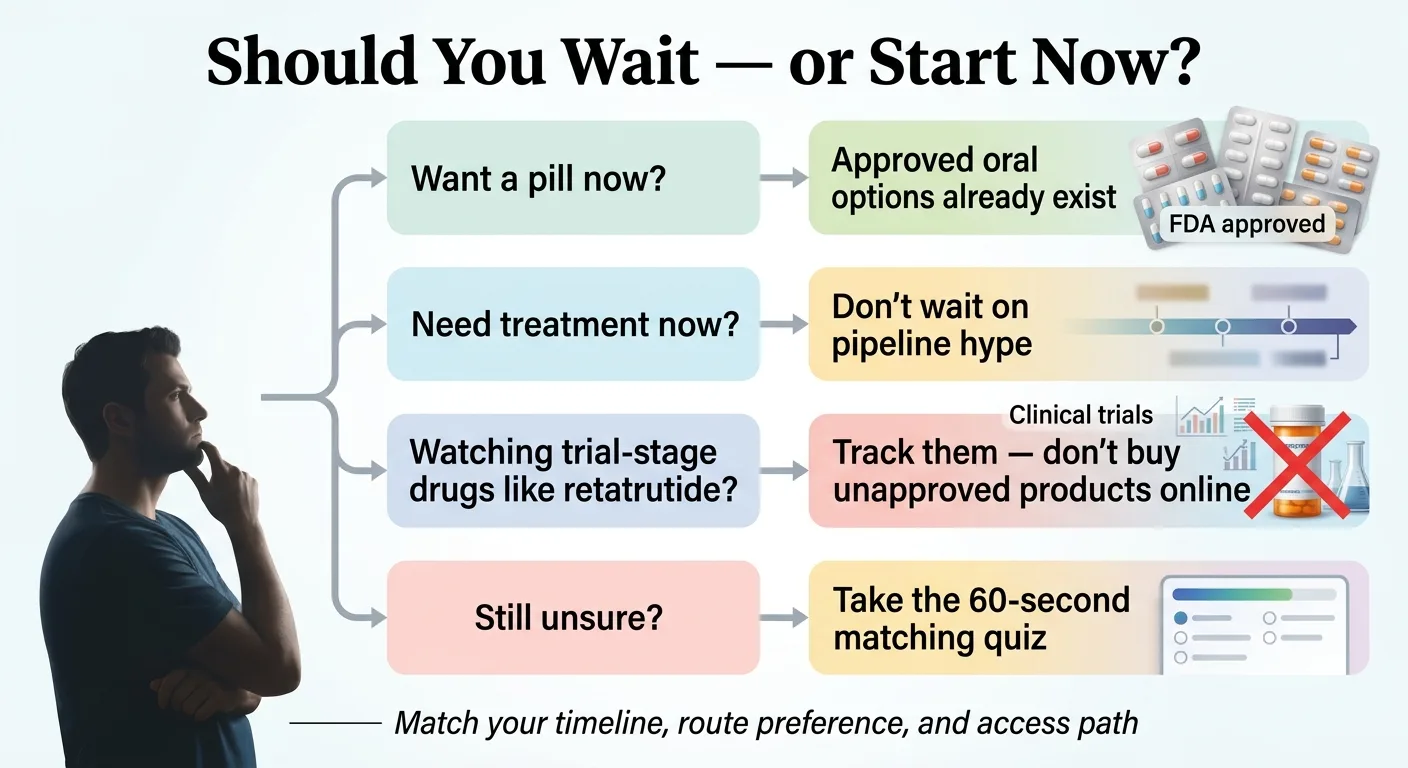
Should you wait for the next-generation GLP-1 drugs coming soon — or start now?
Answer capsule: For most people, waiting does not make sense. Three next-generation GLP-1 drugs are already FDA-approved and available. The highest-efficacy pipeline candidates are, by current trial stage and FDA review timelines, most likely 18 to 24 months away or longer. Waiting only makes sense for a narrow group of readers.
Here’s the framework we use with readers who email us asking this exact question. It’s our working editorial framework — not a medical guideline. Talk to a prescribing clinician about your specific situation before making a decision.
Wait if all three of these are true
- You’re already on a current GLP-1 (Wegovy, Zepbound, Ozempic, or Mounjaro) and, by your prescriber’s assessment, you’ve genuinely plateaued on your maximum tolerated dose.
- Your BMI is still meaningfully elevated and your clinician believes further pharmacologic weight loss is indicated.
- You’re comfortable waiting 12 to 24+ months with no firm availability date, and you’re willing to consider enrolling in a clinical trial in the meantime.
Don’t wait if any one of these is true
- You haven’t started a GLP-1 yet. The current approved drugs already produce meaningful weight loss for most people who tolerate them. Starting now gets you moving; switching later is a conversation with your prescriber, not a logistical crisis.
- You tolerate weekly injections and aren’t hunting for monthly or less-frequent dosing.
- You want a pill. Two are already approved. Waiting for pipeline oral options gains you very little.
- You need treatment now for a medical reason — cardiovascular risk, Type 2 diabetes management, pre-bariatric-surgery weight loss, sleep apnea, MASH.
- You’re tempted by peptide vendors or “compounded retatrutide.” If that’s you, waiting for real approval is safer than buying an unregulated product. We explain why below.
The one damaging admission we have to make
Most of the drugs driving the hype are not something you can start this year. Retatrutide’s 28.7% weight-loss headline is real. The drug is legitimately impressive. But Phase 3 trials still need to read out. An NDA still has to be filed. The FDA still has to review it. Under the best-case timeline, consumers don’t see retatrutide in pharmacies until late 2027 at the earliest — and nothing in drug development is guaranteed.
That’s the hard part.
Here’s the useful part: the current approved drugs already move the needle meaningfully. The gap between 20% weight loss on Wegovy HD today and the pipeline candidates tomorrow matters less than the gap between doing nothing this year and starting this week. If the newer drug turns out to fit you better, you can switch. What you can’t do is get back the year you spent waiting.
What’s already been approved in 2026 (available right now)
Answer capsule: Three next-generation GLP-1s received FDA approval between December 2025 and April 2026: the Wegovy pill (oral semaglutide 25 mg), Wegovy HD (higher-dose weekly injection), and Foundayo (orforglipron, a daily non-peptide pill). All three are currently prescribable through telehealth providers and retail pharmacies.
If you clicked on this page thinking “I want to know what’s coming so I can plan,” there’s a real chance the thing you’ve been waiting for already arrived. Let’s go through each one.
Wegovy pill (oral semaglutide 25 mg) — approved December 22, 2025
The Wegovy pill was the first oral GLP-1 ever approved for weight loss. Novo Nordisk launched it on January 5, 2026, and early uptake has been strong.
What it is: The same active molecule as injectable Wegovy (semaglutide), reformulated into a daily tablet. Approved at 1.5 mg, 4 mg, 9 mg, and 25 mg doses, titrated monthly.
Efficacy: In the OASIS 4 Phase 3 trial, adults who adhered to treatment for 64 weeks lost an average of 16.6% of body weight — statistically close to the 17–18% typically seen with injectable Wegovy 2.4 mg. One in three adherent patients lost 20% or more.
Current pricing (per NovoCare, April 2026): The 1.5 mg starting dose is $149/month self-pay. The 4 mg dose is $149/month through August 31, 2026, then $199/month. The highest doses run about $299/month. Commercially insured patients can pay as little as $25/month with Novo’s savings offer.
The one real drawback: You must take it first thing in the morning on an empty stomach, then wait 30 minutes before eating, drinking anything other than water, or taking other medications. For some people that’s nothing. For others — parents of small children, anyone with a chaotic morning routine — it’s a real friction point. If that 30-minute wait is a deal-breaker, Foundayo (below) has no food or water restriction.
Wegovy HD (semaglutide 7.2 mg injection) — approved March 19, 2026
What it is: A higher-dose version of weekly injectable Wegovy. Until March, the maximum approved dose was 2.4 mg. Wegovy HD triples that to 7.2 mg weekly.
Efficacy: In the STEP UP Phase 3b trial (1,407 adults without diabetes), patients on 7.2 mg lost an average of 20.7% of body weight at 72 weeks — versus 17.5% on the 2.4 mg dose and 2.4% on placebo. Critically, 31.2% of patients on the high dose reached 25% or greater weight loss, compared to 16.7% on 2.4 mg.
Who it’s for: Adults with obesity who have already tolerated the 2.4 mg dose for at least 4 weeks and, per clinical judgment, need additional weight loss. It’s a dose escalation, not a first-line option.
Current self-pay price (NovoCare, April 2026): $399/month for the 7.2 mg single-dose pen. That’s above the $349/month published price for the standard Wegovy 2.4 mg maintenance dose. See our How to get Wegovy HD online guide for the verified routes.
A side effect worth knowing about: Wegovy HD trials flagged dysesthesia — altered skin sensation that patients describe as tingling, increased sensitivity to touch, or a burning feeling. About 22% of patients on 7.2 mg reported it, at higher rates than lower doses. Most cases were mild and resolved on their own or with dose reduction. Low rates of dysesthesia have been reported with other GLP-1 class drugs including tirzepatide, but the frequency appears notably higher at the 7.2 mg dose.
Approval pathway: Wegovy HD was approved 54 days after filing under the FDA’s new Commissioner’s National Priority Voucher (CNPV) program, which fast-tracks drugs aligned with national health priorities.
Foundayo (orforglipron) — approved April 1, 2026
What it is: Eli Lilly’s once-daily GLP-1 pill — and the first non-peptide GLP-1 (meaning it’s a small molecule, not a protein fragment). That matters because non-peptide drugs absorb differently than peptide drugs like oral semaglutide. The practical result: Foundayo has no food or water restrictions. You can take it any time of day, with food, on an empty stomach, with coffee — whenever.
Efficacy: In Lilly’s ATTAIN trial program, patients on the highest dose lost an average of 11–12.4% of body weight at 72 weeks — roughly 27 pounds for participants who completed the trial. That’s lower than the Wegovy pill’s 16.6% but substantially higher than placebo (2–5%). Foundayo is less efficacious than injectable GLP-1s but dramatically more convenient than oral semaglutide.
Dose schedule: Starts at 0.8 mg, then steps up monthly: 2.5 mg → 5.5 mg → 9 mg → 14.5 mg → 17.2 mg (maximum), based on treatment response and tolerability.
Current self-pay price: Starts at $149/month for lower doses, up to $349/month at the highest. As part of Lilly’s CNPV pricing commitment, eligible Medicare Part D beneficiaries may be able to access Foundayo for a $50 copay starting July 1, 2026 per Lilly’s public statement on the approval.
One important caveat — and it’s not a deal-breaker, but you should know: When the FDA approved Foundayo, it required Eli Lilly to conduct a broader set of post-marketing studies and commitments than it asked of Novo for the Wegovy pill. Per the FDA’s approval letter, those include post-marketing studies or registries covering medullary thyroid cancer, long-term pediatric safety, pregnancy exposure, major adverse cardiovascular events (MACE), drug-induced liver injury, delayed gastric emptying and retained gastric contents, and lactation, along with enhanced pharmacovigilance for drug-induced liver injury.
This doesn’t mean Foundayo is unsafe. It means orforglipron is a brand-new molecular entity — the first non-peptide GLP-1 ever approved — and the FDA wants longer-term confirmation for a broader set of endpoints than it needed for semaglutide, which has been approved since 2017. Clinicians reading this will recognize this as a standard pattern for first-in-class molecules. We’ll update this page if anything in the post-market surveillance materially changes the picture.
If one of the three approved options fits your situation, you can start this week
If you’ve read the above and one of the three approved drugs lines up with what you actually want — a pill, a higher dose, or a weekly injection from a verified pharmacy — there’s no reason to keep researching the pipeline.
- → Compare the Wegovy pill vs. Foundayo head to head — our full breakdown of the two daily pills
- → See verified telehealth providers carrying FDA-approved GLP-1s — our ranked provider comparison
- → Not sure which drug or provider fits you? Take the 60-second quiz
Is CagriSema the closest true next-generation obesity drug?
Answer capsule: Yes. CagriSema (cagrilintide 2.4 mg + semaglutide 2.4 mg) is the only major next-wave obesity drug currently under FDA review. Novo Nordisk filed the NDA on December 18, 2025, based on Phase 3 REDEFINE 1 data showing 22.7% mean weight loss at 68 weeks. The FDA is expected to decide in late 2026.
CagriSema is the first fixed-dose combination of a GLP-1 receptor agonist (semaglutide — the active molecule in Wegovy and Ozempic) and an amylin analog (cagrilintide — a long-acting version of a natural satiety hormone). The two hormones work through different pathways: semaglutide targets appetite and insulin signaling; cagrilintide enhances fullness after meals and slows gastric emptying. The theory is that hitting both pathways at once produces greater weight loss and smoother tolerability than either alone.
What the Phase 3 data showed
REDEFINE 1 (3,417 adults with obesity, no diabetes, 68 weeks):
- CagriSema: 22.7% weight loss (trial product estimand — idealized if all patients stayed on treatment); 20.4% under the treatment-policy estimand (intention-to-treat)
- Semaglutide alone: 16.1%
- Cagrilintide alone: 11.8%
- Placebo: 2.3%
- 91.9% of CagriSema patients achieved ≥5% weight loss vs. 31.5% on placebo
REDEFINE 2 (1,206 adults with Type 2 diabetes + obesity/overweight, 68 weeks):
- CagriSema: 15.7% weight loss
- Placebo: 3.1%
Both trials were published in the New England Journal of Medicine and presented at the American Diabetes Association’s 85th Scientific Sessions.
The damaging admission about CagriSema
Here’s the part most excited headlines skipped. In REDEFINE 4 (results published February 23, 2026), CagriSema was compared head-to-head against tirzepatide 15 mg (the active ingredient in Zepbound). At 84 weeks, CagriSema produced 23% weight loss versus tirzepatide’s 25.5%. CagriSema did not meet its primary endpoint of showing non-inferiority to tirzepatide.
That’s a real finding, and you deserve to know about it.
Here’s the context: If raw weight-loss potency is your only priority, CagriSema is probably not your answer — Zepbound today or retatrutide later are better targets. What still makes CagriSema worth watching is its amylin mechanism, which may reduce the GI side effects (nausea, vomiting) that drive many people to discontinue GLP-1 therapy. Amylin receptors sit on a different pathway than the GLP-1 receptors in the brain’s area postrema that trigger most nausea. For someone who has tried Wegovy or Zepbound and stopped because of GI issues, the tolerability profile may matter more than an extra 2–3% of weight loss at 84 weeks. That’s who CagriSema is built for.
→ If you’ve had trouble tolerating semaglutide or tirzepatide, read our full CagriSema vs. retatrutide breakdown — we’ll update both pages the day CagriSema gets a decision.
Is retatrutide approved yet — and when could it actually matter?
Answer capsule: No. As of April 16, 2026, retatrutide is not FDA-approved and is legally available only through authorized Eli Lilly clinical trials. Phase 3 TRIUMPH-4 results showed 28.7% average weight loss at 68 weeks — the highest number ever reported in a Phase 3 obesity trial. Lilly’s public guidance is that the launch timeline depends on completion of the remaining Phase 3 trials and the regulatory process, and Lilly has not published a confirmed NDA filing date.
Retatrutide is the drug everyone’s talking about. It earned the nickname “Triple-G” (in mainstream media, the imprecise term “GLP-3”) because it activates three hormone receptors simultaneously: GLP-1, GIP, and glucagon. Semaglutide (Wegovy) hits one. Tirzepatide (Zepbound) hits two. Retatrutide hits three. And the weight-loss numbers reflect it.
What Phase 3 has shown so far
TRIUMPH-4 (adults with obesity and knee osteoarthritis, 68 weeks) — results announced December 11, 2025:
- Retatrutide 12 mg: 28.7% mean body weight loss (approximately 71.2 pounds, or 32.3 kg)
- Retatrutide 9 mg also reduced knee pain by up to 75.8% on the WOMAC pain score
- Placebo group: approximately 2–3% weight loss
TRANSCEND-T2D-1 (adults with Type 2 diabetes) — results announced March 19, 2026:
- A1C reduction of 1.7% to 2.0% at 40 weeks (versus placebo)
- Weight loss up to 17% at the highest dose (versus placebo)
Seven additional Phase 3 trials are expected to read out through 2026 and into 2027.
Why retatrutide is not a current path
You cannot get retatrutide from any pharmacy, any telehealth provider, any compounder, or any online peptide vendor. Here’s why that matters:
The FDA’s consumer advisory on unapproved GLP-1 drugs notes that these products “have not undergone FDA review for safety, effectiveness, or quality.” Under federal law, retatrutide cannot legally be compounded for human use — it’s not on any FDA-approved shortage list, and it’s not an approved drug. The FDA has issued specific warnings about unlawful retatrutide products sold online.
What that means for you: if you see a website selling “retatrutide peptides” for $200 or $500 a month, that product is not retatrutide as Eli Lilly manufactures it. The identity, purity, dose, and sterility of that product cannot be verified. People have been hospitalized from counterfeit GLP-1 injectables. This isn’t one of those cases where the gray market is a cheaper version of the same drug — it’s a completely unregulated substance sold under the same name.
The dysesthesia signal
Phase 3 retatrutide data also showed elevated rates of dysesthesia — altered skin sensation — in approximately 20.9% of patients on the 12 mg dose. The same signal showed up in Wegovy HD at the 7.2 mg dose. At lower rates, it has also been reported in some tirzepatide trials. Most cases were mild and resolved on their own, but the frequency at high doses of multi-agonist drugs is notably higher than what’s typical for lower-dose single-agonist GLP-1s. Long-term safety data for retatrutide remains limited.
The only legitimate path to retatrutide today
Enroll in an authorized Eli Lilly clinical trial. The TRIUMPH program includes multiple active trials searchable on ClinicalTrials.gov (search “retatrutide” or “LY3437943”). Participation is free and includes regular medical monitoring. Tradeoff: most trials are randomized and placebo-controlled, so you may receive placebo rather than active drug, and you typically won’t know which until the study ends.
Which upcoming drugs are pills, monthly shots, or different enough to matter?
Answer capsule: If your real goal is less-frequent dosing, MariTide (monthly injection, Phase 3) is the main candidate — availability estimated 2028 or later. If your goal is an oral option, two pills are already approved and a third (oral amycretin, Phase 3 starting 2026) is further out. Phase 3 programs like amycretin, VK2735, survodutide, and eloralintide are legitimate to watch but not drugs you can plan around yet.
MariTide (maridebart cafraglutide) — the monthly injection candidate
What it is: Amgen’s once-monthly injectable. MariTide is structurally unusual: it’s an antibody-peptide conjugate combining GLP-1 receptor activation with GIP receptor antagonism. That’s the opposite of tirzepatide’s GIP agonism. The result is a 21-day half-life — roughly three times longer than weekly GLP-1s — which enables monthly or potentially less-frequent dosing.
Phase 2 data (published in NEJM, June 2025, 592 participants):
- Obesity cohort (no diabetes): 12.3% to 16.2% weight loss at 52 weeks (treatment-policy estimand); up to 19.9% (efficacy estimand)
- Obesity + Type 2 diabetes cohort: 8.4% to 12% treatment-policy; up to 17% efficacy estimand
- HbA1c reduction of up to 1.6% to 2.2% in the diabetes cohort
- Weight loss did not plateau at 52 weeks — suggesting longer treatment may produce further reductions
Who it’s for: Readers whose primary barrier to GLP-1 therapy is injection frequency. Twelve injections a year instead of 52 is a meaningful quality-of-life shift.
The honest caveat: Phase 2 showed higher rates of GI adverse events at top doses than weekly GLP-1s. Amgen adjusted Phase 3 dosing to start lower and escalate more gradually. The MARITIME Phase 3 program is active; company-guided readouts are expected in 2027; consumer availability estimated 2028 or later.
Amycretin (Novo Nordisk)
What it is: A single molecule that activates both GLP-1 and amylin receptors — functionally similar to CagriSema but integrated into one molecule instead of two drugs combined. Novo is developing both subcutaneous (weekly injection) and oral (daily tablet) formulations.
Early-phase data:
- Subcutaneous amycretin: up to 24.3% weight loss at 36 weeks (highest dose, 60 mg)
- Oral amycretin: 13% weight loss at 16 weeks
Status: Phase 3 obesity program starting Q1 2026; Phase 3 T2D program following. Consumer availability estimated 2028–2029.
VK2735 (Viking Therapeutics)
What it is: A dual GLP-1/GIP agonist — the same class as tirzepatide. Viking is developing both a subcutaneous weekly injection (Phase 3) and a separate oral formulation that is in an earlier-phase program than the injection. That distinction matters — the two formulations are not on the same timeline.
Phase 2 (VENTURE) data: Up to 14.7% weight loss at 13 weeks (subcutaneous), with no plateau evident at study end.
Status: Phase 3 VANQUISH-1 and VANQUISH-2 trials of the SC formulation enrolled; Viking expects completion in 2027. The oral program is separately developing.
Survodutide (Boehringer Ingelheim / Zealand)
What it is: A dual GLP-1 + glucagon agonist. Phase 3 trials are active for both obesity and metabolic dysfunction-associated steatohepatitis (MASH) — a liver disease in which excess fat drives inflammation and scarring.
Phase 2 data: Up to 19% weight loss at 46 weeks; significant improvements in liver fibrosis markers in MASH.
Status: Phase 3 readouts expected through 2026; FDA decision possible 2027 earliest.
Eloralintide (Eli Lilly)
What it is: A long-acting amylin analog. Similar mechanism to cagrilintide but developed independently by Lilly as a weight-loss drug in its own right.
Phase 2 data: Up to ~20% weight loss in a mid-stage trial.
Status: Advancing to late-stage testing. Consumer availability estimated 2027–2028 earliest.
How the leading candidates compare on weight loss, dosing, and how close they are
Answer capsule: On raw weight-loss numbers, retatrutide leads at 28.7% (Phase 3). Tirzepatide (Zepbound) remains the most effective approved drug at 25.5% in a head-to-head. CagriSema sits at 22.7%, Wegovy HD at 20.7%, and MariTide up to 20% (Phase 2). These numbers are not directly comparable — different trials, populations, durations, and statistical approaches — but they give a rough benchmark.
| Drug | Peak Weight Loss | Trial Phase | Route | How Close Is It? |
|---|---|---|---|---|
| Retatrutide 12 mg | 28.7% @ 68 wk | Phase 3 | Weekly injection | 18–24 months away (estimate) |
| Tirzepatide 15 mg (Zepbound) | 25.5% @ 84 wk | Approved | Weekly injection | Available now |
| Amycretin SC (60 mg) | 24.3% @ 36 wk | Phase 1b/2a | Weekly injection | 2+ years away |
| CagriSema | 22.7% @ 68 wk | Phase 3 (filed) | Weekly injection | Late 2026 if approved |
| Wegovy HD (7.2 mg) | 20.7% @ 72 wk | Approved | Weekly injection | Available now |
| MariTide | Up to 20% @ 52 wk | Phase 3 | Monthly injection | 2028 or later |
| Eloralintide | ~20% | Phase 2 / Phase 3 advancing | Weekly injection | 2027–2028 |
| Survodutide | ~19% @ 46 wk | Phase 3 | Weekly injection | 2027 earliest |
| Wegovy pill (25 mg) | 16.6% @ 64 wk | Approved | Daily pill | Available now |
| VK2735 SC | 14.7% @ 13 wk | Phase 3 | Weekly injection | 2028 or later |
| VK2735 oral | Preliminary | Earlier-phase | Daily pill | Later than SC formulation |
| Foundayo (orforglipron) | 12.4% @ 72 wk | Approved | Daily pill, no food restriction | Available now |
Important caveat: Phase 2 data regularly revises downward in Phase 3. Comparing a Phase 1b/2a number (amycretin) against a Phase 3 number (retatrutide) is apples to oranges. Use this table as a rough sorting, not a tournament bracket.
What could delay or disappoint even the most promising pipeline drugs
Answer capsule: “Coming soon” can still mean trial setbacks, FDA review delays, unexpected safety signals, manufacturing constraints, and competitive misses. CagriSema’s weaker-than-expected head-to-head against tirzepatide is a concrete recent example of how hype outpaces data.
We have to tell you the ways this can go wrong. Every projection above assumes the optimistic end of the range. Here’s what could shift the picture:
Phase 3 readouts that disappoint. Multiple retatrutide trials are still pending. A single trial missing its endpoint — or raising an unexpected safety signal — could push filings from late 2026 into 2027 and consumer availability from 2028 to 2029.
New safety signals. Dysesthesia wasn’t a known GLP-1 side effect two years ago. Now it’s showing up in retatrutide and Wegovy HD trials. Long-term data beyond 2–3 years doesn’t exist for any of the newer multi-agonist drugs. Newer molecules restart the safety clock.
FDA review decisions. The Commissioner’s National Priority Voucher (CNPV) program accelerated Wegovy HD and Foundayo. Reuters reported in early 2026 that the FDA also delayed two drug reviews in the same program over safety and efficacy concerns. Accelerated review cuts both ways.
Manufacturing bottlenecks. The GLP-1 class has been in shortage repeatedly since 2022. A new approval doesn’t automatically mean available supply.
Pricing uncertainty. Third-party analyst estimates cited in industry coverage suggest CagriSema could launch at $1,300–$1,500/month self-pay without insurance. Retatrutide will likely price above existing GLP-1s. Even if a drug arrives, affordability is a separate question.
Muscle preservation. Weight loss on these drugs includes both fat and lean mass. Phase 2 MariTide data showed 7–12% lean mass reduction alongside fat loss. The long-term consequences — especially in older adults — aren’t fully understood.
Weight regain after discontinuation. This applies to the entire GLP-1 class. Stop the drug, weight typically returns. Any pipeline drug will inherit the same constraint unless its mechanism fundamentally changes.
One real human read on the emotional reality
The reporter Bethany Brookshire at Scientific American interviewed Terra Field, a 43-year-old who had lost over 100 pounds on Wegovy before hitting a plateau. Field switched to Zepbound and started losing again. Her description of starting a GLP-1 — that it “felt the way I thought my body should have been operating the entire time,” and that the relief from constant “food noise” changed her life — captures why people are researching the pipeline at all. It’s not vanity. It’s the hope that the next drug fixes the plateau.
That hope is reasonable. Pipeline drugs are legitimately more powerful. The mistake is assuming they’re imminent when they’re not.
Can you legally buy any of these next-generation GLP-1s before approval?
Answer capsule: No. Any drug in Bucket 3 (retatrutide, MariTide, amycretin, VK2735, survodutide, eloralintide) is not legally available from any pharmacy, telehealth provider, or compounder in the United States. The FDA has specifically warned about unapproved GLP-1 drugs sold online, noting these products have not undergone FDA review for safety, effectiveness, or quality.
This section exists because we get emails asking about “compounded retatrutide” and “research peptide retatrutide” every week. The honest answer:
- Retatrutide, MariTide, amycretin, VK2735, survodutide, and eloralintide cannot be legally compounded for human use under federal law. They are investigational drugs — not on any FDA-approved shortage list, not approved drugs.
- Websites selling “retatrutide peptides” are selling unregulated substances. The product’s identity, purity, and dose cannot be verified by the buyer.
- The FDA’s consumer advisory (“FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss”) makes this plain. The FDA has issued specific warnings about unlawful retatrutide sales.
- Compounding pharmacies that operated during FDA-declared shortages of semaglutide and tirzepatide were legal under specific regulatory circumstances. Those circumstances do not apply to pipeline drugs that have never been approved.
The only legitimate way to access a pre-approval GLP-1 is enrolling in an authorized clinical trial. Search ClinicalTrials.gov for the drug name or the trial program (TRIUMPH for retatrutide, MARITIME for MariTide, REDEFINE for CagriSema, VANQUISH for VK2735). Our GLP-1 clinical trials tracker lists every NCT identifier, current status, and weight-loss data for each program.
If you want a legal, effective GLP-1 today: → See verified telehealth providers carrying FDA-approved GLP-1s
What about Medicare and insurance coverage?
Answer capsule: Medicare coverage of GLP-1s for weight loss has historically been limited. The Medicare GLP-1 Bridge runs July 1, 2026 through December 31, 2027 (18 months) — giving eligible beneficiaries access to Wegovy (injection and tablets), Zepbound KwikPen, and Foundayo for a $50/month copay. BALANCE did not launch for Medicare Part D in 2027 — CMS extended the Bridge. It operates outside the standard Part D benefit.
The details, per CMS’s official program page:
- Dates: July 1, 2026 – December 31, 2027 (18-month program, extended from original 6 months because BALANCE did not launch for Medicare Part D in 2027)
- Eligible drugs: Wegovy (injection and tablets), Zepbound KwikPen only, and Foundayo (all formulations) — per CMS FAQ updated April 6, 2026.
- Cost to beneficiary: $50 copay per month (flat, regardless of dose)
- How it works: Operates outside the Part D coverage/payment flow through a CMS-designated central processor (Humana, BIN 028918 / PCN MEDDGLP1BR). Part D sponsors are not directly involved.
- Clinical criteria (prior authorization required): BMI ≥35, OR BMI ≥30 with specific comorbidities (heart failure with preserved ejection fraction, uncontrolled hypertension, or chronic kidney disease stage 3a+), OR BMI ≥27 with pre-diabetes, prior heart attack, prior stroke, or symptomatic peripheral artery disease.
- After December 31, 2027: Watch for BALANCE 2028 announcements during fall 2027 open enrollment (October 15–December 7, 2027).
This is meaningfully different from “Medicare starts covering weight-loss drugs in July.” It’s a time-limited bridge program, a specific drug list, and specific eligibility criteria. Get it clear before you count on it.
For commercial insurance and HSA/FSA details for each approved drug, see our full GLP-1 insurance coverage guide.
How we decided what counts as “coming soon”
Answer capsule: The three buckets on this page — Already here, Closest, Watch list — are The RX Index editorial judgments based on regulatory filing status, clinical trial phase, and legal availability. They are not promises from any manufacturer. This page was last verified on April 16, 2026, and is re-verified monthly.
We’re spelling this out because the methodology is part of our moat. If you can’t see how we sorted the drugs, you can’t trust the sorting.
Bucket 1 — Already here requires all three: FDA approval, current commercial availability, and ability to obtain a legitimate prescription through a pharmacy or telehealth provider. All three drugs in Bucket 1 meet all three criteria as of April 16, 2026.
Bucket 2 — Closest requires: NDA filed with the FDA, under active review, with a reasonable expectation of a decision within 12 months. Only CagriSema meets this standard as of the verification date.
Bucket 3 — Watch list requires: an active Phase 3 program with published or expected readouts, and a plausible (if uncertain) path to consumer availability within 24 to 48 months.
Drugs earlier than Phase 3, drugs that have been discontinued, and drugs paused for safety concerns are not on this page. If the pipeline changes — and it does, roughly every 4 to 6 weeks — the Last Verified date at the top tells you how current our sort is.
What we could not fully verify on April 16, 2026:
- Exact Phase 3 primary completion dates for survodutide, eloralintide, and VK2735 (varies by trial arm)
- Analyst price estimates for CagriSema (published ranges center on $1,300–$1,500/month but Novo has not announced pricing)
- Any new CNPV voucher approvals or review delays after April 16, 2026
- Any CMS updates to the Medicare GLP-1 Bridge eligible-drug list after the verification date
What should you do next if you don’t want to wait?
Answer capsule: Match your goal to the right current option. If you want a pill, Foundayo (no food/water restriction) or the Wegovy pill (empty stomach required) are both available now. If you want maximum weight loss on an approved drug, Zepbound (tirzepatide) or Wegovy HD (semaglutide 7.2 mg) are the strongest current options. If you’re uncertain, the quiz narrows it down in under a minute.
Here’s the simple routing:
If you want a pill with no food restriction
Foundayo is the newest option, available through Ro and most pharmacies. Ro’s Body membership starts at $39 for the first month, then as low as $74/month with annual prepay — that covers the clinical service, with the medication billed separately.
If you want a pill and can work around the empty-stomach requirement
The Wegovy pill delivers higher weight loss (16.6% vs. 12.4%) and is available from $149/month cash through Novo Nordisk’s NovoCare Pharmacy, CVS, Costco, and most major telehealth providers.
→ Full Wegovy pill vs. Foundayo breakdown
If you want the strongest current injectable
Zepbound (tirzepatide) at 15 mg reached 25.5% weight loss in REDEFINE 4 — still the most effective approved weight-loss drug. Wegovy HD at 7.2 mg reached 20.7% with a different safety profile.
→ Compare your approved GLP-1 options
If you’ve plateaued on your current GLP-1
The realistic next step is a dose escalation (e.g., Wegovy 2.4 mg → Wegovy HD 7.2 mg) or a switch to a different mechanism (semaglutide → tirzepatide). Waiting specifically for retatrutide is a defensible choice only if, per your prescriber’s judgment, your situation warrants it and you’re comfortable with an uncertain timeline.
→ CagriSema vs. retatrutide: which plateau answer fits you?
Frequently asked questions
What are the next-generation GLP-1 drugs coming soon?
The main next-generation GLP-1 drugs in development or newly approved are: the Wegovy pill (approved December 2025), Wegovy HD (approved March 2026), Foundayo/orforglipron (approved April 2026), CagriSema (under FDA review since December 2025), retatrutide (Phase 3), MariTide (Phase 3), amycretin (Phase 3 starting Q1 2026), survodutide (Phase 3), eloralintide (Phase 3 advancing), and VK2735 (SC in Phase 3, oral earlier-phase). Three are available now; one is under review; the rest are 18+ months away based on current trial stage.
Is retatrutide FDA approved?
No. As of April 16, 2026, retatrutide is not FDA-approved and is available only through authorized Eli Lilly clinical trials. Phase 3 TRIUMPH-4 results (released December 11, 2025) showed 28.7% weight loss at 68 weeks. Eli Lilly has not published a confirmed NDA filing date; launch timing depends on completion of the remaining Phase 3 trials and the regulatory process.
When will retatrutide be available?
Based on Eli Lilly's public guidance and standard FDA review timelines, consumer availability is estimated for late 2027 or 2028. Lilly has not confirmed a specific date. Anyone claiming to sell retatrutide today outside a clinical trial is operating outside FDA regulation.
Is CagriSema approved in the U.S.?
No, not yet. Novo Nordisk filed the NDA for CagriSema on December 18, 2025, and the FDA is expected to decide in late 2026. If approved, CagriSema would be the first fixed-dose combination of a GLP-1 receptor agonist (semaglutide) and an amylin analog (cagrilintide) for weight management.
Are the Wegovy pill and Foundayo already available?
Yes. The Wegovy pill (oral semaglutide 25 mg) was approved December 22, 2025 and launched January 5, 2026. Foundayo (orforglipron) was approved April 1, 2026 and began shipping April 6, 2026. Both are available at retail pharmacies and through telehealth providers. Starting self-pay prices are approximately $149/month for lower doses.
Which upcoming GLP-1 drug produces the most weight loss?
Retatrutide produced the highest weight loss in Phase 3 — 28.7% at 68 weeks on the 12 mg dose (TRIUMPH-4). Among FDA-approved drugs, tirzepatide (Zepbound) 15 mg reached 25.5% in REDEFINE 4 (head-to-head vs. CagriSema), and Wegovy HD reached 20.7% in STEP UP. Phase 2 and Phase 3 results are not directly comparable — Phase 2 numbers often revise downward in larger Phase 3 trials.
Should I wait for a next-generation GLP-1 or start now?
For most people, starting now makes more sense. Three next-generation GLP-1s are already FDA-approved. The most talked-about pipeline drug (retatrutide) is estimated to be 18–24 months away from consumer availability based on current trial stage. Waiting specifically for a pipeline drug is reasonable only if: you're already on a current GLP-1 and have genuinely plateaued per your prescriber's judgment, you want a specific feature like monthly dosing that no current drug matches, or you're comfortable waiting with no firm date.
Can you legally buy retatrutide online?
No. Retatrutide is not FDA-approved, cannot be legally compounded for human use under federal law, and any product sold as “retatrutide” outside a clinical trial is unregulated. The FDA has specifically warned about unlawful retatrutide products sold online. The only legitimate path today is enrolling in an authorized Eli Lilly clinical trial through ClinicalTrials.gov.
What's the difference between the Wegovy pill and Foundayo?
The Wegovy pill contains semaglutide (a peptide), requires an empty stomach with a 30-minute wait, and produces 16.6% average weight loss at 64 weeks. Foundayo contains orforglipron (a non-peptide small molecule), has no food or water restrictions, and produces 12.4% average weight loss at 72 weeks. Wegovy pill is more effective; Foundayo is more convenient. Both start around $149/month cash.
What is a triple agonist weight-loss drug?
A triple agonist activates three hormone receptors simultaneously: GLP-1, GIP, and glucagon. Retatrutide is the first triple agonist to reach Phase 3 trials. Activating all three pathways appears to produce greater weight loss than single-agonist drugs (Wegovy) or dual-agonist drugs (Zepbound).
Will Medicare cover these new GLP-1 drugs?
The CMS Medicare GLP-1 Bridge runs July 1, 2026–December 31, 2027 (18 months) at $50/month for eligible Part D beneficiaries — covering Wegovy (injection and tablets), Zepbound KwikPen, and Foundayo. BALANCE did not launch for Medicare Part D in 2027 — CMS extended the Bridge. The Bridge operates outside the standard Part D benefit and requires BMI/comorbidity criteria. CagriSema pricing and coverage are not yet announced.
About this page
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We build content for people navigating GLP-1 medication decisions — comparing providers, tracking FDA approvals, and separating legitimate medical options from the noise.
How we built this page: We independently verified each factual claim against FDA press releases and approval letters, Eli Lilly and Novo Nordisk investor communications, NovoCare’s published price guide, the Amgen newsroom, NEJM and The Lancet Diabetes & Endocrinology publications, Viking Therapeutics investor releases, ClinicalTrials.gov records, the FDA’s consumer advisory on unapproved GLP-1 drugs, and CMS’s official Medicare GLP-1 Bridge program page. Where a detail couldn’t be confirmed, we flag it.
How often it’s updated: Monthly for the first six months after publication, quarterly after that, and immediately when any listed drug changes regulatory status. The “Last verified” date at the top tells you how current the page is.
Editorial standards: This is YMYL content — Your Money or Your Life — and we take EEAT seriously. We don’t claim to be clinicians. We don’t claim compounded drugs are “clinically proven” or share “the same active ingredient” as approved drugs. We don’t write “medically reviewed by” a clinician unless a named, verifiable clinician has actually reviewed the page. Editorial judgments are labeled as such.
Affiliate disclosure: We earn commissions when readers start a GLP-1 program through certain telehealth providers linked on this page. Compensation does not influence which providers we mention or how we describe them. The Ro-specific link in this article appears because Ro carries Foundayo (a featured drug on this page) at pricing we have independently confirmed against Ro’s own published pricing page. If our recommendations diverged from what’s best for readers, the site would stop working. We know that.
Corrections and updates: We welcome notes from prescribing clinicians, patients with first-hand experience on these drugs, and pharmaceutical industry sources who spot a factual detail that needs updating. Contact through the site footer.
Sources and primary references
- U.S. Food and Drug Administration. Approval letter and press release for Foundayo (orforglipron). April 2026.
- U.S. Food and Drug Administration. Press release: “FDA Approves Fourth Product Under National Priority Voucher Program, Higher Dose Semaglutide.” March 19, 2026.
- U.S. Food and Drug Administration. Approval letter and press release for oral semaglutide (Wegovy pill). December 22, 2025.
- U.S. Food and Drug Administration. Consumer advisory: “FDA's Concerns with Unapproved GLP-1 Drugs Used for Weight Loss.” fda.gov.
- Eli Lilly. Investor communications: TRIUMPH-4 results (Dec 11, 2025), TRANSCEND-T2D-1 results (Mar 19, 2026), Foundayo launch and pricing, retatrutide development status page.
- Novo Nordisk. Press releases: Wegovy pill approval and US launch, Wegovy HD approval, CagriSema NDA submission (Dec 18, 2025), REDEFINE 1, REDEFINE 2, REDEFINE 4 results.
- NovoCare. Wegovy Price Guide (April 2026) and pharmacy.html.
- Amgen. Newsroom: MariTide Phase 2 results.
- Jastreboff AM, et al. “Once-Monthly Maridebart Cafraglutide for the Treatment of Obesity — A Phase 2 Trial.” New England Journal of Medicine, 2025.
- Wharton S, et al. “Once-Weekly Semaglutide 7.2 mg in Adults with Obesity (STEP UP).” Lancet Diabetes & Endocrinology, 2025.
- Viking Therapeutics. Investor releases: VENTURE Phase 2, VANQUISH-1 and VANQUISH-2 Phase 3 program.
- ClinicalTrials.gov. Records for TRIUMPH, MARITIME, REDEFINE, VANQUISH, OASIS, and STEP UP trial programs.
- Centers for Medicare & Medicaid Services. Medicare GLP-1 Bridge official program page. cms.gov.
- Reuters. Reporting on REDEFINE 4 head-to-head results and FDA CNPV program review delays. 2026.
- Brookshire B. Profile of patient experience switching from Wegovy to Zepbound. Scientific American, 2025.
Page first published: April 16, 2026 · Last verified: April 16, 2026 · Reviewed monthly.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup