Drug Pipeline · GLP-1 Explainer · April 22, 2026
What Is GLP-3? The Real Drug Behind the Nickname
By Kaden, founder of The RX Index — a pricing intelligence and comparison resource for GLP-1 telehealth providers. Last verified: April 22, 2026.
You searched what is GLP-3, probably after seeing a headline about a drug that helped trial participants lose an average of 71 pounds. Here’s what almost nobody says up front: “GLP-3” isn’t actually a thing. Not a hormone your body makes. Not an official drug class. Not something a doctor can legally prescribe today.
It’s a nickname — one Eli Lilly’s own medical team has called “scientifically inaccurate” — that the media attached to retatrutide, an investigational once-weekly injection that hits three metabolic receptors at once (GLP-1, GIP, and glucagon) instead of one or two. Retatrutide is in Phase 3 clinical trials. It is not FDA-approved. And the FDA has explicitly stated it cannot be compounded under federal law. If a website is offering to sell you “GLP-3,” it is either selling an unapproved product or misleading you about what it is.
Want a personalized action plan for what you can start today — without waiting for FDA approval or risking a gray-market seller?
Take our free 60-second GLP-1 match quiz →GLP-3 quick facts
Why people say “GLP-3”: retatrutide acts on three receptor pathways. More accurate label: triple agonist.
| Factor | Detail |
|---|---|
| Real drug name | Retatrutide (code: LY3437943) |
| Maker | Eli Lilly |
| What it actually is | Triple hormone receptor agonist (GLP-1, GIP, glucagon) |
| FDA approval status | Not approved. Investigational. |
| Is “GLP-3” an official term? | No. Lilly calls it “scientifically inaccurate.” |
| Can a doctor prescribe it? | Only to clinical-trial participants. |
| Can it be compounded? | No. FDA has explicitly stated retatrutide cannot be used in compounding under federal law. |
| Earliest pharmacy availability | Late 2027–2028 (editorial projection; not a confirmed date) |
| Peak Phase 3 weight loss (non-T2D) | 28.7% average over 68 weeks at 12 mg (TRIUMPH-4 topline, Dec 2025) |
| Phase 3 weight loss in T2D | 16.8% average over 40 weeks at 12 mg (TRANSCEND-T2D-1 topline, Mar 2026) |
Sources: Eli Lilly retatrutide FAQ; FDA “Concerns with Unapproved GLP-1 Drugs Used for Weight Loss”; Eli Lilly investor releases (Dec 11, 2025; Mar 19, 2026).
What is GLP-3, exactly?
Answer capsule: “GLP-3” is a media and marketing nickname for retatrutide, a triple hormone receptor agonist. It is not an official scientific classification or an FDA-recognized drug category. Eli Lilly — the company that developed retatrutide — explicitly calls “GLP-3” a “scientifically inaccurate” label and says “triple agonist” is the correct term.
People started calling retatrutide “GLP-3” the same way people started calling Zepbound a “GLP-2.” First-generation drugs like Ozempic and Wegovy target one receptor (GLP-1). Second-generation drugs like Mounjaro and Zepbound target two (GLP-1 and GIP). Retatrutide targets three. So commentators lined them up: GLP-1, “GLP-2,” “GLP-3.” It’s tidy, it’s easy to tweet, and it’s wrong.
The real peptide family doesn’t work that way. Your body makes GLP-1 (glucagon-like peptide-1) and GLP-2 (glucagon-like peptide-2). There is no human “GLP-3” hormone. (A peptide called GLP-3 exists in cartilaginous fish like sharks and regulates ketone metabolism. Not relevant to your weight.)
Say this, not that
| Common search term | What people usually mean | More accurate phrase |
|---|---|---|
| GLP-3 / GLP-3 drug | Retatrutide | Triple hormone receptor agonist |
| GLP-3 agonist | Retatrutide (or another triple) | Triple agonist |
| GLP-3 shot | Retatrutide injection inside a clinical trial | Retatrutide (investigational) |
| GLP-3 peptide | Retatrutide sold as a “research peptide” | Unapproved research-use-only peptide |
When a website uses “GLP-3” as if it’s an approved drug category, that’s your first signal to step back.
Is GLP-3 a real hormone or drug class?
Answer capsule: No. There is no human hormone called GLP-3. There is no FDA-recognized drug class called “GLP-3 agonist.” The term is informal shorthand for “triple hormone receptor agonist” — a class that currently contains one late-stage clinical-trial drug: retatrutide.
Some clinics advertise “GLP-3” programs as if they were the next step up from GLP-1 — same shelf, just stronger. They are not on the same shelf. GLP-1 drugs like semaglutide are FDA-approved, carry prescribing information, have been studied in hundreds of thousands of patients, and have known safety profiles. Retatrutide is investigational. It exists inside a research protocol. It does not exist in a pharmacy.
How GLP-3 differs from GLP-1 drugs and tirzepatide
Answer capsule: GLP-1 drugs activate one receptor. Dual agonists like tirzepatide activate two (GLP-1 and GIP). Retatrutide activates three (GLP-1, GIP, and glucagon). In trial averages, each generation has delivered larger average weight loss. The catch: only the first two generations are approved and available.
Each added receptor attacks weight from a different angle:
- GLP-1 is the appetite and blood-sugar lever. It slows how fast your stomach empties, quiets hunger signals, and improves insulin response. Semaglutide (Wegovy, Ozempic, Rybelsus) and liraglutide live here.
- GIP amplifies the GLP-1 effect and appears to help the body metabolize fat more efficiently. Tirzepatide (Zepbound, Mounjaro) was the first commercial drug to add it.
- Glucagon nudges the body’s metabolic rate up: more calories burned at rest, more fat oxidation, more liver-fat clearance. Retatrutide is the first late-stage investigational drug to layer glucagon activation on top of GLP-1 and GIP.
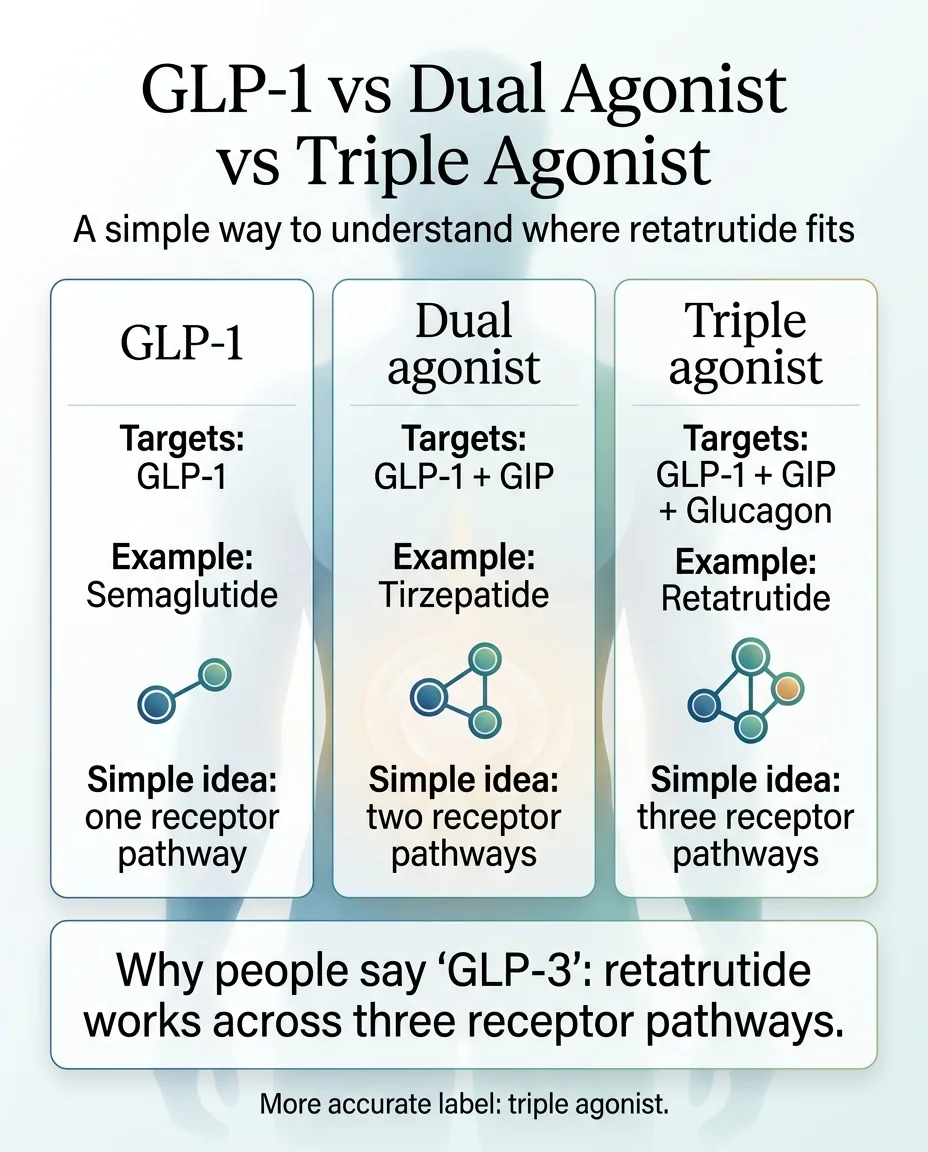
GLP-1 (one receptor) → Dual agonist (two receptors) → Triple agonist (three receptors). Only the first two are FDA-approved.
Generation comparison
| Gen 1: GLP-1 | Gen 2: Dual GLP-1/GIP | Gen 3: Triple (“GLP-3”) | |
|---|---|---|---|
| Receptors activated | GLP-1 | GLP-1 + GIP | GLP-1 + GIP + glucagon |
| Lead molecule | Semaglutide | Tirzepatide | Retatrutide (LY3437943) |
| Brand names | Ozempic, Wegovy, Rybelsus | Mounjaro, Zepbound | None — investigational |
| Peak avg weight loss in pivotal trial | 14.9% at 68 wks (STEP 1, NEJM 2021) | 22.5% at 72 wks (SURMOUNT-1, NEJM 2022) | 28.7% at 68 wks (TRIUMPH-4 topline, Dec 2025) |
| FDA status | Approved | Approved | Phase 3 trials |
| Legal access today | Rx via telehealth or clinic | Rx via telehealth or clinic | Clinical trial only |
| Published head-to-head vs other GLP-1s? | Yes (STEP, SUSTAIN programs) | Yes (SURPASS-2; SURMOUNT-5) | No published results yet (NCT06662383 active) |
| Dosing | Weekly inj. or daily oral | Weekly inj. | Weekly inj. (investigational) |
Two caveats: First, no published head-to-head results directly compare retatrutide with semaglutide or tirzepatide in the same trial population (one active study, NCT06662383, is running). Second, trial averages are not personal guarantees. Real-world outcomes tend to be lower than clinical-trial averages.
Wondering which approved option actually fits your situation?
Take our free 60-second match quiz →Why everyone is suddenly talking about GLP-3
Answer capsule: The term exploded after Eli Lilly reported TRIUMPH-4 topline results in December 2025 — the first Phase 3 data for retatrutide — showing an average of 71.2 pounds of weight loss at the highest dose. A second Phase 3 readout in March 2026 (TRANSCEND-T2D-1) showed up to 2.0% A1C reduction and 16.8% weight loss in people with type 2 diabetes. Mainstream outlets started calling retatrutide “GLP-3,” and the nickname stuck.
Fox News, Scientific American, Wellworthy, and The Atlantic all ran pieces. Podcast hosts picked it up because it’s easier to say than “triple hormone receptor agonist.” Online sellers noticed the search volume and started marketing retatrutide as “GLP-3” — usually with a “research use only” label that does nothing to stop buyers from injecting it anyway.
What readers are actually saying (voice-of-customer signal, not medical evidence):
- “What is GLP3? Is that Reta?”
- “I’ve googled that it’s not FDA approved. Is it safe?”
- “Some of the sites look fake.”
Sources: r/Longreads, r/Retatrutide, Looksmax
What the retatrutide studies actually show
Answer capsule: Retatrutide has one peer-reviewed Phase 2 trial in the New England Journal of Medicine showing up to 24.2% average weight loss at 48 weeks. Two Phase 3 trials (TRIUMPH-4 and TRANSCEND-T2D-1) have reported topline numbers, but those readouts are company press releases — not yet peer-reviewed. Strong evidence; incomplete evidence.
In TRIUMPH-4, discontinuation due to adverse events was 12.2% at the 9 mg dose and 18.2% at the 12 mg dose versus 4% for placebo. Analysts noted that’s higher than with other incretin therapies. Long-term safety is still being studied.
Evidence ladder (strongest to weakest)
| Tier | Evidence type | Retatrutide examples |
|---|---|---|
| 1 | Peer-reviewed publication | Jastreboff et al., NEJM 2023 (Phase 2, 24.2% at 48 wks); Sanyal et al., Nature Medicine 2024 (Phase 2a liver-fat trial) |
| 2 | Company topline press release | TRIUMPH-4 (Dec 11, 2025, 28.7% at 68 wks); TRANSCEND-T2D-1 (Mar 19, 2026, 16.8% weight + up to 2.0% A1C at 40 wks) |
| 3 | Analyst projection / consumer summary | “Approval expected 2027” — projections, not facts |
| 4 | Social media and forum chatter | Anecdotal only. Not evidence. |
TRANSCEND-T2D-1 data is scheduled for the American Diabetes Association Scientific Sessions in June 2026. Peer-reviewed publications pending for both TRIUMPH-4 and TRANSCEND-T2D-1.
Is GLP-3 FDA-approved?
No. Retatrutide is not FDA-approved as of April 22, 2026.
It is an investigational drug in Phase 3 trials. Eli Lilly has not filed a New Drug Application. Analyst projections place potential approval in late 2027 or 2028 — editorial estimates, not confirmed dates.
Lilly’s own public FAQ: “Retatrutide is not currently approved by the FDA and is considered an investigational medication.” The only legal way to receive real retatrutide in 2026 is as a participant in one of Lilly’s clinical trials.
Major TRIUMPH Phase 3 trials (as of April 2026)
| Trial | Indication | Status | Readout |
|---|---|---|---|
| TRIUMPH-1 | Obesity | Ongoing | Expected 2026 |
| TRIUMPH-2 | Obesity with T2D | Ongoing | Expected 2026 |
| TRIUMPH-3 | Obesity + established CVD | Ongoing | Expected 2026 |
| TRIUMPH-4 | Obesity + knee OA | TOPLINE REPORTED Dec 2025 — 28.7% avg weight loss, 75.8% pain-score reduction | Peer-review pending |
| TRIUMPH-5 | Obesity + moderate-to-severe OSA | Ongoing | Expected 2026 |
| TRIUMPH-6 | Obesity + MASLD (liver disease) | Ongoing | Expected 2026 |
| TRIUMPH-7 | Obesity + chronic low back pain | Ongoing | Expected 2026 |
| TRANSCEND-T2D-1 | Type 2 diabetes | TOPLINE REPORTED Mar 2026 — up to 2.0% A1C reduction, 16.8% weight loss at 40 wks | ADA June 2026; peer-review pending |
The damaging admission, stated plainly
Retatrutide does not solve the “what can I start today?” problem. If you need a treatment path right now — because your weight is actively affecting your life, your joints, your blood sugar, or your mental health — retatrutide isn’t your answer. It isn’t going to be your answer for at least 18 months in the best case. If your priority is treatment now, an FDA-approved GLP-1 is the better move.
Can you buy GLP-3 or retatrutide right now?
Answer capsule: Not through any legal US retail channel. Retatrutide is not available at pharmacies or through telehealth prescribing. The FDA has explicitly stated that retatrutide cannot be used in compounding under federal law. The only legitimate access today is participating in a TRIUMPH clinical trial.
FDA’s own statement: “Retatrutide and cagrilintide cannot be used in compounding under federal law. Additionally, these are not components of FDA-approved drugs and have not been found safe and effective for any condition.”
In September 2025, FDA sent warning letters to multiple companies (including GLP-1 Solution, EA WORKS dba Trust Labs, and ASN-LABS) for selling compounded retatrutide. Every letter made the same point: retatrutide fails the conditions of both 503A and 503B.
The retatrutide access matrix
| Access path | Legitimate? | What you actually get | Risk |
|---|---|---|---|
| TRIUMPH clinical trial | ✅ Yes | Real retatrutide, supervised, at no cost | Low (monitored) |
| US pharmacy with prescription | ❌ Not possible | Nothing — no FDA approval, no legal prescription pathway | N/A |
| “Compounded retatrutide” from a pharmacy or telehealth | ❌ No | Product that fails FDA’s 503A and 503B conditions | High |
| “Research-use-only” peptide sites | ❌ No | Unverified powder sold with disclaimers | Very high |
| Overseas / gray-market online | ❌ No | Unknown-source product marketed as retatrutide | Very high |
You can search for active TRIUMPH trials at ClinicalTrials.gov. Enrollment requires a specific BMI range plus usually one qualifying condition. Our GLP-1 clinical trials tracker lists every TRIUMPH NCT ID, current status, and published weight-loss data.
Not eligible for a trial — or don’t want to wait?
See which approved option fits you in 60 seconds →The gray-market GLP-3 problem
Retatrutide is being sold online by overseas vendors and “research peptide” websites, often labeled “not for human consumption” as a legal shield. Users who inject these products are self-experimenting with an investigational drug from unknown facilities, without medical oversight. Reported side effects include dysesthesia — a painful or burning nerve sensation — and FDA has warned consumers not to purchase these products.
Red-flag checklist: signs a “GLP-3” listing is unsafe
- ✗Labeled “research use only” or “not for human consumption” — but the seller provides dosing instructions.
- ✗Ships from outside the US with no verifiable FDA-registered manufacturing facility.
- ✗Accepts cryptocurrency only or requires off-platform payment.
- ✗No US address and no licensed US pharmacist.
- ✗Arrives as lyophilized powder you have to reconstitute yourself.
- ✗No prescription, no medical consultation, no clinical oversight.
Which pages get “GLP-3” wrong? Our live accuracy audit
We scored major pages currently ranking for “GLP-3” queries on four criteria: (1) correctly identifies “GLP-3” as an informal nickname; (2) explicitly states retatrutide is not FDA-approved; (3) addresses legal retail availability; (4) shows or links primary-source proof. Audit date: April 22, 2026. Re-run monthly.
| Source | Calls informal? | Not FDA-approved? | Legal access? | Primary source? | Score |
|---|---|---|---|---|---|
| Lilly retatrutide FAQ | ✅ | ✅ | ✅ | ✅ | 4 / 4 |
| FDA Concerns page | N/A | ✅ | ✅ | ✅ | 3 / 3 |
| Drugs.com retatrutide | ✅ | ✅ | ✅ | ✅ | 4 / 4 |
| Wellworthy (Mar 2026) | ✅ | ✅ | ~ | ✅ | 3.5 / 4 |
| Dr. Sobo clinic | ✅ | ✅ | ~ | ✅ | 3 / 4 |
| Tucson Wellness MD | ✅ | ✅ | ~ | ~ | 2.5 / 4 |
| Scientific American (Mar 2026) | ~ | ✅ | ~ | ✅ | 2.5 / 4 |
| Fox News (Jan 2026) | ✅ | ~ | ❌ | ~ | 1.5 / 4 |
| The BioStation | ❌ | ❌ | ❌ | ❌ | 0 / 4 |
Clinic and commerce pages that use “GLP-3” as an approved drug class tend to fail all four criteria. If you land on a page that scores below 2/4 on this audit, you are probably being sold something rather than informed. Next audit: May 22, 2026.
Should you wait for retatrutide or start something now?
If you don’t need treatment urgently, waiting is reasonable — retatrutide could be the most effective weight-loss drug ever approved if trials hold. If you need treatment now, waiting 18+ months is not a neutral choice. Starting an FDA-approved GLP-1 today does not prevent you from switching to retatrutide later if and when it’s approved.
Path 1: Wait and watch
You’re in no urgency. Subscribe to Lilly’s investor releases. Track ClinicalTrials.gov. Check back here quarterly for the updated TRIUMPH tracker. Just don’t pretend you’re “not waiting” while quietly buying peptides online.
Path 2: Enroll in a clinical trial
You want real retatrutide, supervised, free. You meet the eligibility criteria (BMI threshold plus usually one qualifying condition) and can travel to a trial site. Search ClinicalTrials.gov for active TRIUMPH sites. This is the only legitimate access pathway in 2026.
Path 3: Start an FDA-approved GLP-1 now (right for most readers)
You need treatment now, or you don’t want to gamble on a regulatory timeline. FDA-approved GLP-1s are available today, carry real safety data from hundreds of thousands of patients, and work for most people who qualify. Starting now doesn’t close the door to retatrutide later.
What you can actually start today
If you want the widest FDA-approved menu with insurance help
Ro Body is the primary recommendation here. Ro carries every FDA-approved GLP-1 for weight loss currently on the US market: Wegovy pill, Wegovy pen, Zepbound pen, Zepbound KwikPen, Foundayo, Ozempic, and Saxenda. Ro’s insurance concierge fights for coverage and submits your prior authorization paperwork. Membership is $39 the first month, then as low as $74/month with annual prepay or $149/month month-to-month. Medication billed separately from the membership fee.
The “I thought GLP-3 was coming, what do I do?” reader usually wants a mainstream, FDA-approved, insurance-capable program — not something in a regulatory gray area. Ro maps to that mental model.
See current Ro pricing and formulary → (sponsored affiliate link, opens in a new tab)If you want FDA-approved brand-name, self-pay, provider choice
Sesame Care is the secondary FDA-approved path. Broad branded formulary (Wegovy, Zepbound, Ozempic, Mounjaro, Foundayo, Saxenda), Costco-member pricing available, and visible provider choice. Good fit for self-pay shoppers who want to see the prescriber they’re getting.
See if Sesame Care fits your situation →If you’re considering a compounded GLP-1 program
The compounded GLP-1 market in April 2026 operates under much tighter rules than during the 2023–2024 shortage era. The FDA declared the tirzepatide shortage resolved on December 19, 2024 and the semaglutide shortage resolved on February 21, 2025. Enforcement discretion for 503A and 503B compounders ended in spring 2025. In March 2026, FDA sent warning letters to more than 30 telehealth companies for misleading marketing of compounded GLP-1 products.
Compounded GLP-1s still exist legitimately for patients with documented clinical needs an approved drug can’t meet. For most readers, the FDA-approved path is cleaner, safer, and increasingly competitive on price now that Ro matches LillyDirect, NovoCare, and TrumpRx pricing.
Not sure which path fits your situation?
Five questions. 60 seconds. Personalized output based on your situation (self-pay vs insurance, injection vs oral, urgency).
Take the free quiz and get your personalized GLP-1 action plan →What we actually verified for this page
- Lilly retatrutide FAQ — “GLP-3 is scientifically inaccurate” framing, investigational status. Verified April 22, 2026.
- Eli Lilly investor release, Dec 11, 2025 — TRIUMPH-4 topline (28.7% weight loss, 71.2 lb avg, 75.8% pain-score reduction, discontinuation 12.2% at 9 mg / 18.2% at 12 mg). Verified April 22, 2026.
- Eli Lilly investor release, Mar 19, 2026 — TRANSCEND-T2D-1 topline (up to 2.0% A1C reduction, 16.8% weight loss at 40 wks). Verified April 22, 2026.
- FDA “Concerns with Unapproved GLP-1 Drugs Used for Weight Loss” — retatrutide cannot be compounded. Verified April 22, 2026.
- FDA warning letters (September 9, 2025) — to GLP-1 Solution, EA WORKS dba Trust Labs, and ASN-LABS. Verified April 22, 2026.
- FDA declaratory orders — tirzepatide shortage resolved Dec 19, 2024; semaglutide shortage resolved Feb 21, 2025. Verified April 22, 2026.
- Ro Body Program formulary — Wegovy, Foundayo, Zepbound, Ozempic, Saxenda (Ro does not offer Mounjaro). Verified April 22, 2026 at ro.co.
- NEJM Phase 2 trial — Jastreboff et al. 2023 (24.2% weight loss at 48 weeks). Verified April 22, 2026.
Next re-verification: May 22, 2026. Spotted an error? Email [email protected].
Frequently asked questions about GLP-3 and retatrutide
Is GLP-3 FDA-approved?
No. Retatrutide — the drug people call “GLP-3” — is not FDA-approved as of April 2026. It is an investigational drug in Phase 3 clinical trials. Eli Lilly has not yet submitted a New Drug Application.
Is GLP-3 the same as retatrutide?
In nearly every use, yes. “GLP-3” is an informal nickname for retatrutide, the most advanced triple hormone receptor agonist in development. Lilly’s own medical team calls the “GLP-3” label “scientifically inaccurate” and prefers “triple agonist.”
Is GLP-3 a real hormone?
No. Humans make GLP-1 and GLP-2. There is no human “GLP-3” hormone. A GLP-3 peptide exists in cartilaginous fish like sharks, but has no relevance to human weight loss or diabetes treatment.
Can a doctor prescribe retatrutide?
Only to clinical-trial participants. Retatrutide is not an FDA-approved drug, has no US prescribing information, and is not available at retail pharmacies. A doctor outside a clinical trial cannot legally prescribe it.
Can compounded retatrutide be used?
No. The FDA has explicitly stated that retatrutide cannot be used in compounding under federal law. FDA has issued warning letters to multiple companies selling compounded retatrutide. Retatrutide does not meet the conditions of either Section 503A or Section 503B.
Is GLP-3 better than Ozempic or Wegovy?
In pivotal trials, retatrutide produced a larger average weight loss (28.7% at 68 weeks) than semaglutide (14.9% at 68 weeks in the STEP 1 trial). No published head-to-head results compare them directly. For a real-world reader, the practical comparison is simple: Ozempic and Wegovy are available today; retatrutide won’t be for at least 18 months.
How much weight do people actually lose on retatrutide?
In the Phase 3 TRIUMPH-4 trial, the 12 mg dose produced an average of 28.7% weight loss — roughly 71 pounds — over 68 weeks in adults with obesity and knee osteoarthritis. In the Phase 3 TRANSCEND-T2D-1 trial, adults with type 2 diabetes lost an average of up to 16.8% over 40 weeks. Individual results vary. Trial averages are not guarantees.
What are the side effects of retatrutide?
Most commonly reported: nausea, diarrhea, vomiting, constipation, decreased appetite — consistent with the broader GLP-1 class. In Phase 2 trials, 7% of retatrutide participants reported cutaneous hyperesthesia or dysesthesia versus 1% on placebo. In TRIUMPH-4, discontinuation due to adverse events was 12.2% at 9 mg and 18.2% at 12 mg. Long-term safety is still being studied.
When will GLP-3 / retatrutide be available to the public?
Realistic editorial projections: late 2027 through 2028, assuming Phase 3 trials complete on schedule, Eli Lilly files a New Drug Application, and the FDA completes a standard review. This is a projection based on typical regulatory timelines, not a confirmed date. Delays are common.
How is GLP-3 different from Zepbound?
Zepbound (tirzepatide) is a dual agonist — it hits GLP-1 and GIP receptors. Retatrutide is a triple agonist — it hits GLP-1, GIP, and glucagon. The third receptor is the novel move, and it’s the reason retatrutide trial averages are larger. Zepbound is FDA-approved and available; retatrutide is not.
Can I buy GLP-3 online?
Not legally in the US. Websites selling retatrutide as “research use only” or through overseas channels are operating outside FDA enforcement and are not legitimate pharmacies. The FDA has issued warning letters to companies selling compounded retatrutide and has warned consumers not to purchase these products.
Is retatrutide the same as a “triple G” drug?
Yes. “Triple G” (short for GIP/GLP-1/glucagon) and “triple agonist” both refer to the same drug class. Retatrutide is currently the only late-stage clinical candidate in this class. It’s the molecule that both nicknames most often describe.
Related guides
Sources and references
Primary-source citations:
- Eli Lilly retatrutide FAQ, “What to know about retatrutide” — lilly.com
- FDA, “FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss” — fda.gov
- FDA warning letters (Sept. 9, 2025) to GLP-1 Solution, EA WORKS dba Trust Labs, ASN-LABS — fda.gov
- FDA Declaratory Order, “Resolution of Tirzepatide Injection Product Shortage,” Dec. 19, 2024 — fda.gov
- FDA Declaratory Order, “Resolution of Semaglutide Injection Product Shortage,” Feb. 21, 2025 — fda.gov
- Eli Lilly investor release, Dec. 11, 2025 (TRIUMPH-4 topline) — investor.lilly.com
- Eli Lilly investor release, Mar. 19, 2026 (TRANSCEND-T2D-1 topline) — investor.lilly.com
- Jastreboff AM et al., “Triple-Hormone-Receptor Agonist Retatrutide for Obesity — A Phase 2 Trial,” NEJM 389: 514–526 (2023)
- Sanyal AJ et al., Phase 2a MASLD retatrutide trial, Nature Medicine (2024)
- ClinicalTrials.gov — TRIUMPH program listings; NCT06662383
- Ro Body Program formulary and pricing pages — ro.co
News and explainer sources referenced:
- Scientific American, “Drug retatrutide helps people lower blood sugar and lose weight” (Mar 2026)
- Wellworthy, “What is GLP-3? The drug behind the next wave of weight-loss medicine” (Mar 2026)
- Fox News, “‘GLP-3’ retatrutide drug delivers major weight loss breakthrough” (Jan 2026)
- The Atlantic, “The Next Ozempic Is Already Being Sold Underground” (Dec 2025)
- Clinical Trials Arena, “Lilly’s triple G agonist boasts 28.7% weight loss in Phase III trial” (Dec 2025)
Still not sure which GLP-1 program is right for you?
Five questions. Personalized output. No phone call. No spam. Just the answer to “what should I actually do now?”
Take our free 60-second GLP-1 matching quiz →Last verified: April 22, 2026. Next scheduled re-verification: May 22, 2026. The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We publish comparisons and explainers, not prescriptions or medical advice. Information on this page is updated monthly as new Lilly and FDA information becomes available. Talk to a licensed healthcare provider before starting or stopping any medication.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup