Does Medicare Cover Foundayo? The Real 2026 Answer
Standard Part D won’t cover Foundayo for weight loss. The Bridge is available at $50/month as of July 1, 2026 for eligible Part D members. The savings card is commercial insurance only.
Does Medicare cover Foundayo? Yes — but not the way most people expect, and not for everyone.
Regular Medicare Part D won’t pay for Foundayo when you’re using it just to lose weight. An old federal rule blocks that. Here’s the new part: starting July 1, 2026, if you qualify, you can get Foundayo for a $50 monthly copay through a program called the Medicare GLP-1 Bridge, which runs through December 31, 2027.
The catch the ads won’t tell you: that “$25 a month” savings card you may have seen does not work for anyone on Medicare. And if you don’t meet the program’s rules, you’re looking at $149 to $349 a month out of pocket.
So the real answer isn’t a flat yes or no. It comes down to three things: your plan, your weight, and your health history. Below, we show you exactly which of three “doors” is yours — and we walk you through the same checks your doctor will need, so you can stop guessing.
Can Medicare cover Foundayo? Find your situation
| Your situation | Does Medicare cover Foundayo? | What you’ll likely pay | Your next move |
|---|---|---|---|
| You have a Part D or Medicare Advantage drug plan AND you meet the Bridge health rules | Yes — through the GLP-1 Bridge | $50/month | Ask your doctor to prepare a Bridge request for on or after July 1, 2026 |
| You want regular Part D to cover it for weight loss | No | Not covered this way | Use the Bridge if you qualify |
| You have Original Medicare but no drug plan | No | Not eligible for the Bridge | Look into a Part D plan during enrollment |
| You qualify for the Bridge but get Extra Help | Yes, but the copay stays $50 | $50/month (Extra Help can’t lower it) | Don’t expect it to be cheaper than $50 |
| You don’t qualify, need a cash-pay option, or need a backup while a Bridge request is pending | Medicare won\u2019t help here | $149\u2013$349/month cash | Compare cash-pay routes (below) |
Sources: CMS Medicare GLP-1 Bridge pages; FDA Foundayo label; Eli Lilly / LillyDirect pricing. Full list at the bottom.
Answer five quick questions and get a checklist to bring to your doctor. Takes about a minute, and it\u2019s not a provider sign-up.
Does Medicare cover Foundayo in 2026?
Yes, but only through the Medicare GLP-1 Bridge, and only if you qualify. Regular Medicare Part D does not cover Foundayo for weight loss the normal way. The Bridge is a separate, temporary program that gives eligible people a $50/month price as of July 1, 2026. It is not the same as your plan adding Foundayo to its list of covered drugs.
Think of it as three doors:
Your normal drug plan. For weight-loss-only Foundayo, this door is locked. (We explain why next.)
The new door. If you qualify, you walk through here for $50 a month as of July 1, 2026.
If you don’t qualify, or you don’t want to wait, you pay the full price yourself: $149–$349/month.
Most articles online describe only one door. That’s why the answers feel so confusing — one site says “Medicare doesn’t cover weight-loss drugs,” another says “Medicare will cover GLP-1s for $50,” and both are telling the truth about a different door. The rest of this page walks you through all three so you know which one is yours.
Why does regular Part D still say “no” to Foundayo for weight loss?
Medicare Part D has a long-standing rule that stops it from covering drugs used only for weight loss. That rule has been in place since Part D began, and it’s why GLP-1s for obesity have historically not been covered. Foundayo is FDA-approved only for weight management, so under a normal Part D plan, it falls under that exclusion.
Here’s the part that trips people up. Some weight-loss drugs do get covered by Medicare — but only because they’re also approved for something else. Ozempic and Mounjaro, for example, are approved for type 2 diabetes, so a plan can cover them for a diabetic patient.
Foundayo doesn’t have that backup yet. Right now it’s approved only for chronic weight management — not diabetes, not sleep apnea, nothing else. Eli Lilly has said it’s studying orforglipron (Foundayo’s active ingredient) for type 2 diabetes, but as of this update, the FDA label we verified is for weight management only. So the usual “it’s covered for diabetes” workaround simply doesn’t exist for Foundayo.
So the door to regular Part D is locked for weight-loss Foundayo. The good news is there’s a second door — and it opened July 1, 2026.
The $50 path: what the Medicare GLP-1 Bridge actually is
The Medicare GLP-1 Bridge is a short-term government program that lets eligible Part D members get certain weight-loss drugs — including Foundayo — for a flat $50 copay. It is available as of July 1, 2026 and runs through December 31, 2027. It works outside your normal drug plan, so your plan doesn’t have to “approve” Foundayo for you to use it.
A few plain-English facts that matter:
- You pay $50 a month. Behind the scenes, drugmakers agreed to a discounted price of $245 a month for the program, but your share is the $50 copay.
- Your Part D plan isn’t running it. A single central processor — a contractor CMS set up — handles the paperwork and payments, not your plan or its pharmacy benefit manager.
- Your plan can’t block it. Plans don’t have to opt in. If you’re eligible, you can use the Bridge as of July 1, 2026 no matter which qualifying plan you have.
- It covers more than Foundayo. Wegovy and Zepbound are also covered under the Bridge for weight management (more on the exact forms further down).
What that means for you: there’s a real 2027 cliff. When the Bridge ends on December 31, 2027, CMS has not announced a confirmed program that keeps Foundayo at $50 after that. If you start Foundayo through the Bridge, don’t assume the $50 price lasts forever. Plan for it to be a window — a generous one, but a window.
We’d rather tell you that now than have you find out the hard way. For more on BALANCE, see our BALANCE model guide.
Do you qualify? The three Bridge pathways
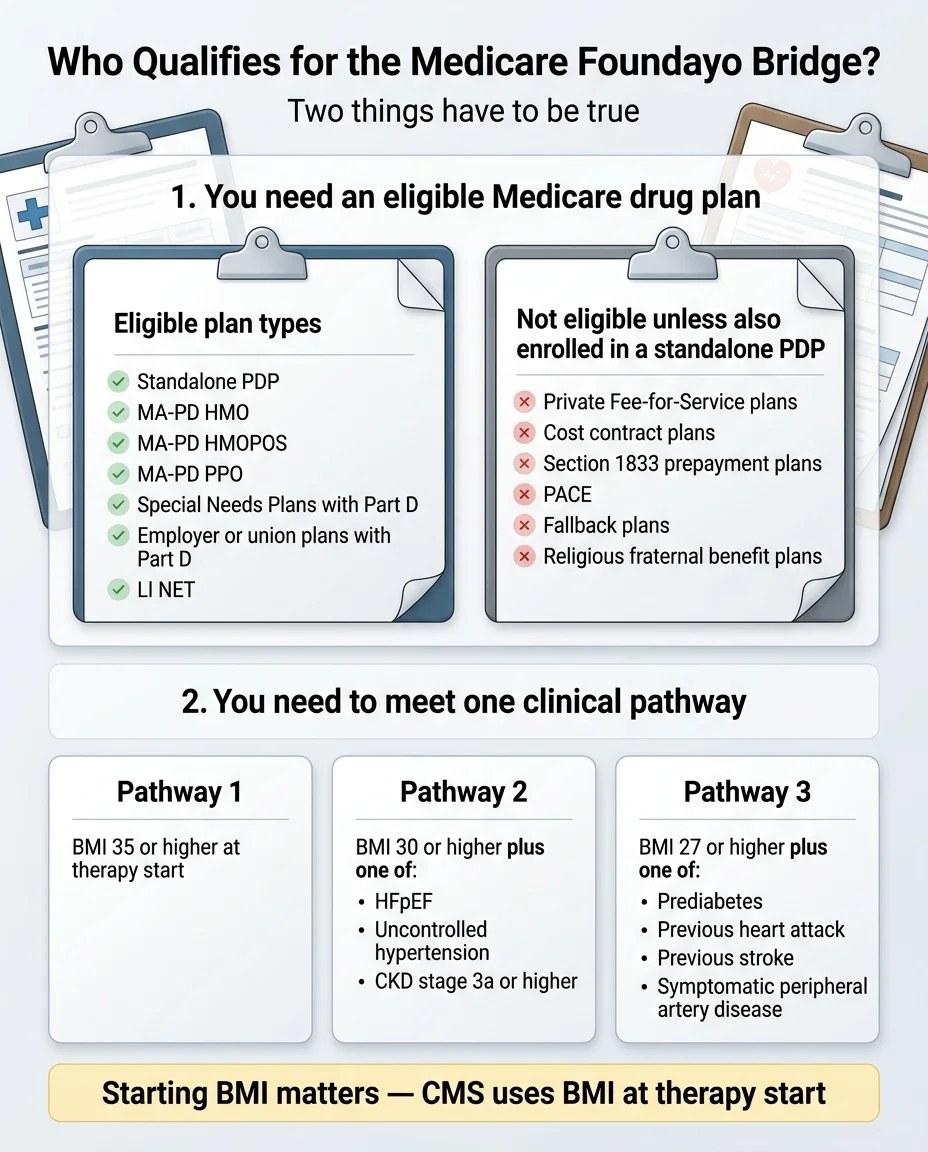
To get the $50 price, your doctor has to confirm three things: you’re in an eligible drug plan, you’re taking Foundayo for weight management, and you meet one of three BMI-and-health pathways. You can’t sign yourself up — your prescriber submits the request for you. Here’s exactly what each pathway requires.
| Pathway | What you need | What to bring to your doctor |
|---|---|---|
| Pathway 1 | Age 18+ and a BMI of 35 or higher when you started GLP-1 therapy — no other condition required | Height/weight record, weight-management note |
| Pathway 2 | Age 18+ and a BMI of 30 or higher, plus one of: heart failure (HFpEF), uncontrolled high blood pressure (over 140/90 despite two BP meds), or chronic kidney disease stage 3a or higher | Diagnosis list, blood pressure history, kidney records |
| Pathway 3 | Age 18+ and a BMI of 27 or higher, plus one of: prediabetes, a past heart attack, a past stroke, or symptomatic peripheral artery disease (PAD) | A1C or glucose labs, heart/stroke history, PAD diagnosis |
Source: CMS Medicare GLP-1 Bridge — Information for Providers and for Beneficiaries.
• BMI is body mass index — a number based on your height and weight.
• HFpEF is a type of heart failure where the heart muscle is stiff.
• PAD is peripheral artery disease — narrowed arteries, usually in the legs.
• Prior authorization (PA) is the request your doctor sends to get the drug approved. The Bridge requires one.
The detail that could save your spot: your starting BMI counts
Here’s something almost no other page tells you, and it’s straight from CMS. Eligibility is based on your BMI when you first started GLP-1 therapy — not your BMI today.
CMS gives this exact example: someone who started a GLP-1 in September 2024 at a BMI of 37, and is now down to a BMI of 34, still qualifies under the BMI ≥ 35 pathway. Their doctor simply attests that they met the rule when they began.
To be clear, this is about paperwork, not about regaining weight. Never do anything to change your BMI for a form. Just make sure your records show where you started.
What “lifestyle modification” means (and doesn’t)
The rules say Foundayo must be prescribed alongside ongoing lifestyle changes — nutrition and physical activity. Don’t let that scare you. It does not mean you have to prove you’ve been perfect. It means your doctor should note that the medication is part of a real plan that includes how you eat and move. That’s it.
See which pathway fits you, then get the exact questions and records to bring to your appointment.
How much does Foundayo cost with Medicare?
If you qualify for the Bridge, Foundayo costs $50 a month. If you don’t, you’ll pay the cash price of $149 to $349 a month, because Medicare won’t chip in for a weight-loss-only drug. There’s some fine print on that $50 worth knowing before you start.
If you qualify: $50 a month — with two honest catches
We won’t pretend that’s nothing. But here’s the other side: $50 a month still beats every legitimate way to buy Foundayo with cash that we could find. If you qualify, this is almost certainly your cheapest path — full stop. The fine print is real, and the deal is still good. Both things are true.
Here’s what the $50 looks like over the life of the program, if you fill it every month:
| Path | 1 month | July–Dec 2026 (6 fills) | All of 2027 (12 fills) | Full 18-month program |
|---|---|---|---|---|
| GLP-1 Bridge | $50 | $300 | $600 | $900 |
| Cash-pay (Lilly’s posted prices) | $149–$349 | $894–$2,094 | $1,788–$4,188 | $2,682–$6,282 |
| You save with the Bridge | $99–$299 | up to ~$1,794 | up to ~$3,588 | up to ~$5,382 |
A price comparison, not a dosing plan — your dose is your doctor’s call. Lilly says taxes and fees may apply and that its self-pay offer can change at any time, so re-check current LillyDirect pricing before you commit. Sources: CMS ($50 copay, dates); Lilly (posted self-pay prices).
If you don’t qualify: the cash price
Eli Lilly’s posted self-pay prices through LillyDirect are:
- $149/month for the 0.8 mg starter dose
- $199/month for 2.5 mg
- $299/month for the maintenance doses (5.5 mg, 9 mg, 14.5 mg, 17.2 mg)
- The two highest doses (14.5 mg and 17.2 mg) rise to $349/month if you don’t refill within 45 days of your last fill
For comparison, the average retail price without any discount runs close to $778 a month, so the LillyDirect price is already a big markdown. We cover your cash-pay options in detail further down.
Can you use the Foundayo $25 savings card with Medicare?
No. The Foundayo savings card flatly excludes anyone on Medicare or any other government insurance. Lilly’s own terms say the card is not available to people enrolled in Medicare, Medicare Part D, Medicare Advantage, Medigap, Medicaid, VA, or TRICARE. That “$25 a month” deal is for people with commercial (work or marketplace) insurance only.
This catches a lot of people, especially if you saw a Foundayo ad on TV. The $25 price is real — it’s just not for you if you’re on Medicare. Here’s how the lanes actually break down:
| Your coverage | The $25 savings card? | Your real low-cost path |
|---|---|---|
| Commercial insurance that covers Foundayo | Possibly — as low as $25/month | Use the savings card |
| Commercial insurance that doesn’t cover Foundayo | A separate Lilly self-pay savings rate may apply | Lilly self-pay savings |
| Medicare or other government insurance | No \u2014 you\u2019re excluded | The $50 Bridge (if eligible), or cash-pay |
| Paying cash, no Bridge | No | LillyDirect, Ro, or Sesame |
Does Medicare Advantage cover Foundayo?
Medicare Advantage can get you into the Bridge — but only if your plan includes prescription drug coverage (an MA-PD plan) and you meet the health rules. A Medicare Advantage plan with no drug coverage isn’t enough on its own. The good news: your plan doesn’t have to volunteer to take part, and your normal Medicare appeal rights stay in place.
Here’s how the main plan types line up, straight from CMS:
| Your plan | Can you use the Bridge? | Notes |
|---|---|---|
| Standalone Part D drug plan (PDP) | Yes, if you meet the health rules | The most common path |
| Medicare Advantage with drug coverage (MA-PD: HMO, HMO-POS, local or regional PPO) | Yes, if you meet the health rules | Your plan doesn’t have to opt in |
| Special Needs Plan (SNP), employer or union retiree drug plan (EGWP), or LI NET | Yes, if you meet the health rules | CMS lists these as eligible plan types |
| Dual-eligible (Medicare and Medicaid) in an eligible drug plan | Yes, if you meet the health rules and prior-authorization criteria | |
| TRICARE For Life | Only if you also have an eligible Part D plan and meet the rules | TRICARE For Life by itself isn’t enough |
| Original Medicare with no drug plan | No | You need a qualifying drug plan |
| PACE, private fee-for-service, cost contract, prepayment, fallback, or religious fraternal plans | Usually no | Unless you also have a standalone PDP. These plan types aren’t eligible on their own. |
Source: CMS Bridge eligibility guidance. Quick definitions: an SNP is a Special Needs Plan for people with specific conditions or situations; an EGWP is an employer or union retiree drug plan; LI NET is a temporary Medicare program for certain low-income people.
What about Foundayo for diabetes, sleep apnea, or other conditions?
The Bridge is only for weight management. If a GLP-1 is prescribed for a condition Part D already covers — like type 2 diabetes, sleep apnea, certain heart-risk uses, or a specific liver disease — that goes through regular Part D, not the Bridge. And because Foundayo is approved only for weight management right now, this other path isn’t open for Foundayo specifically.
This matters because Medicare treats the reason for your prescription differently:
- If a GLP-1 is prescribed for type 2 diabetes, obstructive sleep apnea, a heart-risk use, or noncirrhotic MASH (a type of fatty liver disease), CMS says those uses can be covered by regular Part D — so you’d use your normal plan, not the Bridge. CMS even names examples, like Zepbound for sleep apnea and Wegovy to lower heart risk; those don’t go through the Bridge.
- But Foundayo’s FDA approval is for weight management only. So for now, if you want Foundayo, the Bridge (Door 2) or cash-pay (Door 3) are your realistic paths — not the diabetes or other-condition route.
How do you actually get Foundayo through the Bridge?
You can’t enroll yourself. Your doctor submits a prior authorization request and prescription for you through the current Bridge process. The smart move is to get your documentation together now so your doctor can submit right away.
- Confirm your plan type. Make sure you have a standalone Part D plan or a qualifying MA-PD plan.
- Know your “why.” The prescription has to be for weight management.
- Gather your starting BMI. Find the chart record of your height and weight from when you began (or plan to begin) a GLP-1.
- Gather any qualifying diagnosis. If you’re using the BMI ≥ 30 or BMI ≥ 27 pathway, you’ll need proof of the matching condition.
- Talk to your doctor about whether Foundayo is right for you.
- On or after July 1, 2026, your doctor submits the Bridge prior authorization to the central processor.
- If approved, your pharmacy fills it and collects the $50.
What to ask your doctor (copy this)
Don’t ask your doctor to “run Foundayo through Part D for weight loss” — that’s the locked door, and it’ll likely come back denied. Ask specifically about the Medicare GLP-1 Bridge.
What to have ready when you talk:
- Your current medication list
- The date you started a GLP-1 (if you’ve taken one before)
- Your starting height and weight (for your starting BMI)
- Recent labs if you’re using the prediabetes pathway
- Blood pressure history and meds if using the blood-pressure pathway
- Kidney, heart, stroke, or PAD records if those apply
This one message does more than any phone call to your plan. It points your doctor at the right door from the start.
What if your Medicare Foundayo request gets denied?
A denial doesn’t always mean you’re out of luck — sometimes it means the request went through the wrong door. A “denied for weight loss” message often means it was sent to regular Part D instead of the Bridge. Knowing which kind of denial you got tells you what to do next.
| What the denial says | What it probably means | What to ask next |
|---|---|---|
| “Excluded for weight loss” | It was sent through regular Part D, not the Bridge | “Can this be submitted through the Medicare GLP-1 Bridge instead?” |
| “Prior authorization required” | Paperwork or proof is missing | “Which BMI or diagnosis detail was missing?” |
| “Not on formulary” | A plan-list issue, not necessarily a Bridge issue | “Does the Bridge’s central processor handle this instead of my plan?” |
| “Not eligible for the Bridge” | A pathway or plan-type gap | “Which exact rule did I miss?” |
| “Submitted too early or to the wrong payer” | The Bridge wasn’t taking requests yet or the request went to the wrong payer | “Can we resubmit through the current Bridge process?” |
• If it was sent to regular Part D for weight-loss Foundayo, an appeal probably won’t fix it — you need it sent through the Bridge instead.
• If it was a Bridge request with missing proof, gather the documents and resubmit.
• Either way, your Medicare appeal rights still apply.
What if you don’t qualify for the Bridge?
If you don’t meet the rules — or you do not qualify, need a cash-pay option, or need a backup while a Bridge request is pending — your main option is paying cash through a manufacturer-direct or telehealth route, since Medicare won’t help with weight-loss Foundayo any other way. This is also where we get honest about what telehealth can and can’t do for you.
| Option | Best for | What to know |
|---|---|---|
| LillyDirect | The lowest cash price with your own doctor | No membership fee. Posted prices $149–$349/month. The savings card still won’t apply if you’re on Medicare. |
| Ro | Someone who wants an online visit, a prescriber, and a flat cash price they can start now | Cash-pay only for Medicare members. Offers FDA-approved Foundayo at LillyDirect-matched prices ($149–$349). Membership: $39 first month, then $149/month or as low as $74/month with annual plan upfront. |
| Sesame | Someone who wants to choose their own clinician from a marketplace | Sesame’s providers can prescribe Foundayo through LillyDirect (same $149–$349 pricing and 45-day high-dose rule). Program starts at $59/month on an annual plan or $99 month-to-month; medication not included. |
The honest truth about Ro and Medicare
So if using your Medicare benefits is the goal, Ro is the wrong tool — pursue the $50 Bridge with your own doctor instead (scroll back up to the doctor script). We’d rather send you to the cheaper path than sell you something that doesn’t fit.
But here’s why Ro still earns a place for the right person. Because Ro skips the government-insurance coordination entirely, it gives you two things the Bridge can’t: you can start this week if you don’t qualify or are waiting on a Bridge request, and you skip the prior-authorization waiting game. Ro folds the online visit, the prescription, and a transparent flat price into one place. Medicare members can join Ro Body and pay cash for certain medications. Ro Body is $39 for the first month, then $149/month — or as low as $74/month with an annual plan paid upfront — with the medication billed separately.
In plain terms: if you qualify for the Bridge, take it. If you don’t qualify, or you want to start now without the paperwork, a cash-pay route like Ro is a legitimate option.
For people who don\u2019t qualify for the $50 Bridge \u2014 or who\u2019d rather start now without a prior-authorization wait. Sponsored. Ro is a cash-pay option for Medicare members and says it can\u2019t coordinate coverage for government insurance.
Prefer to choose your own clinician? See Foundayo options on Sesame → (sponsored affiliate link, opens in a new tab) (also cash-pay, at LillyDirect-matched pricing).
Foundayo vs. Wegovy vs. Zepbound on Medicare
If you qualify for the Bridge, cost usually isn’t the deciding factor — Foundayo, Wegovy, and Zepbound are all covered for weight management at the same $50 copay. The choice comes down to how the medicine is taken and what your doctor recommends. This is a coverage comparison, not a ranking of which one works best.
| Drug | On the Bridge for weight management? | How you take it |
|---|---|---|
| Foundayo | Yes — all forms | Daily pill |
| Wegovy | Yes — all forms (shot and pill) | Weekly shot or daily pill |
| Zepbound | Yes \u2014 KwikPen only; the single-dose vial and single-dose pen are not included | Weekly injection (KwikPen) |
Source: CMS Bridge drug and formulation list.
The takeaway: if you’re eligible and choosing between these three on Medicare, you’re not really choosing on price — they’re all $50 under the Bridge. You’re choosing on whether you want a pill or a shot, your medical history, and what your clinician thinks fits you best. That’s a conversation for your doctor, not a spreadsheet.
Before you ask: Foundayo safety basics
Foundayo is a prescription medicine with real risks, and only a licensed clinician should decide if it’s right for you. This guide is about coverage — it’s not a substitute for medical advice or the full prescribing information.
A few things the FDA label flags that are worth knowing before your appointment:
- Not for everyone. Foundayo is contraindicated (must not be used) if you or your family have a history of medullary thyroid cancer (MTC) or a condition called MEN2.
- Other warnings in the label include pancreatitis, gallbladder problems, kidney injury from dehydration, low blood sugar (especially with insulin or sulfonylureas), serious allergic reactions, severe stomach problems, eye changes in people with type 2 diabetes (diabetic retinopathy), and a risk during surgery because the drug slows stomach emptying — so tell any surgical team you’re taking it.
- Don’t double up. The label says you shouldn’t use Foundayo together with another GLP-1 medicine unless your prescriber specifically directs it.
- Common side effects include nausea, constipation, diarrhea, vomiting, and indigestion.
The label also covers drug interactions, use during pregnancy, and use if you have severe liver problems — bring those up with your clinician. Watch for symptoms like a lump in the neck, hoarseness that won’t quit, or trouble swallowing, and tell your doctor right away.
Bottom line: bring your full medical history to your appointment. The coverage path only matters after your clinician agrees Foundayo is safe and appropriate for you.
How we verified this guide
We anchored the coverage, FDA, safety, and pricing facts in CMS, FDA, and Eli Lilly sources, and used reputable health-policy and provider pages for context where noted — and we re-check it on a schedule, because prices and program rules keep changing.
| What we verified | Source | Last checked |
|---|---|---|
| Foundayo FDA approval (April 1, 2026) and weight-management-only indication | FDA / Lilly prescribing information | June 4, 2026 |
| Bridge dates (July 1, 2026–Dec 31, 2027) and $50 copay | CMS Bridge pages | June 4, 2026 |
| $245 net program price; runs outside Part D | CMS | June 4, 2026 |
| Three eligibility pathways and the “starting BMI” rule | CMS (provider + beneficiary pages) | June 4, 2026 |
| Eligible plan types (PDP, MA-PD, SNP, EGWP, LI NET, dual-eligible, TRICARE For Life) | CMS beneficiary page | June 4, 2026 |
| $50 doesn’t count toward deductible/cap; Extra Help can’t lower it | CMS; AJMC | June 4, 2026 |
| Covered drugs and forms (Foundayo all; Wegovy all; Zepbound KwikPen only) | CMS beneficiary page | June 4, 2026 |
| BALANCE delay and the 2027 cliff | KFF; U.S. News | June 4, 2026 |
| Savings card excludes government/Medicare beneficiaries | Eli Lilly savings terms | June 4, 2026 |
| Self-pay prices ($149–$349) and the 45-day refill rule | LillyDirect | June 4, 2026 |
| Foundayo boxed warning and contraindications | FDA / Lilly label; DailyMed | June 4, 2026 |
| Ro and Sesame cash-pay Foundayo offerings | Ro; Sesame Care | June 4, 2026 |
Frequently asked questions
- Does Medicare cover Foundayo for weight loss?
- Not through regular Part D — that’s blocked by a federal rule against covering weight-loss drugs. But eligible Part D members can get Foundayo for $50 a month through the Medicare GLP-1 Bridge, available as of July 1, 2026, if they meet the health rules.
- When does Medicare coverage for Foundayo start?
- The Bridge is open as of July 1, 2026. A doctor can submit a Bridge request through the current CMS process if the patient qualifies.
- How much will Foundayo cost with Medicare?
- About $50 a month if you qualify for the Bridge. That $50 doesn’t count toward your Part D deductible or yearly out-of-pocket cap, and Extra Help can’t lower it. If you don’t qualify, you’ll pay the cash price of $149 to $349 a month.
- Does the $50 Foundayo Bridge copay count toward my Part D out-of-pocket cap?
- No. CMS says eligible GLP-1 drugs under the Bridge are outside the Part D benefit payment flow, so the $50 copay doesn’t count toward your true out-of-pocket costs and the Part D deductible doesn’t apply.
- Does Medicare Advantage cover Foundayo?
- A Medicare Advantage plan that includes prescription drug coverage (an MA-PD plan) can use the Bridge if you meet the rules. A Medicare Advantage plan without drug coverage can’t, by itself.
- Do I need a Part D plan to get Foundayo through the Bridge?
- Yes. You must be in a standalone Part D plan or a qualifying MA-PD plan. Original Medicare alone won’t work. Special Needs Plans, employer/union retiree drug plans, and LI NET also count.
- Can TRICARE For Life beneficiaries get Foundayo through the Bridge?
- Only if they’re also enrolled in a Bridge-eligible Part D plan type and meet the prior-authorization criteria. TRICARE For Life on its own isn’t enough.
- Can I use the Foundayo $25 savings card if I’m on Medicare?
- No. Lilly’s savings card excludes Medicare, Medicare Part D, Medicare Advantage, Medigap, Medicaid, VA, and TRICARE. The $25 price is for commercial insurance only.
- Does the Bridge cover Ozempic or Mounjaro for weight loss?
- The Bridge covers Foundayo, Wegovy (all forms), and Zepbound (KwikPen only) for weight management. Ozempic and Mounjaro aren’t Bridge drugs for weight loss, but they may be covered by regular Part D for type 2 diabetes, depending on your plan and diagnosis.
- What if my BMI is lower now because I already lost weight?
- You may still qualify. CMS bases eligibility on your BMI when you started GLP-1 therapy, not your current BMI, so dig up your starting records before you apply.
- Is there a cheaper compounded version of Foundayo?
- We don’t recommend “compounded Foundayo” or “compounded orforglipron” offers. Compounded drugs aren’t FDA-approved, orforglipron is a patent-protected brand drug that isn’t on the FDA’s shortage list, and the FDA restricts compounding copies of commercially available medications. Treat any such ad as a red flag.
- Is Foundayo FDA-approved?
- Yes. The FDA approved Foundayo (orforglipron) on April 1, 2026, for chronic weight management in adults with obesity, or overweight with at least one weight-related condition, alongside a reduced-calorie diet and increased physical activity.
Sort the Bridge, regular insurance, and cash-pay options based on your situation \u2014 in about a minute.
Related guides
- Medicare GLP-1 Bridge explained: $50/month, who qualifies, what’s covered
- Foundayo cost without insurance: 2026 real math
- Foundayo prior authorization guide: what your doctor submits
- CMS BALANCE model and Foundayo: what the delay means for you
- Does Aetna cover Foundayo?
- Does Medicare Advantage cover Wegovy?
Sources
- CMS — Medicare GLP-1 Bridge, Information for Medicare Beneficiaries
- CMS — Medicare GLP-1 Bridge, Information for Providers
- CMS — Medicare GLP-1 Bridge (overview)
- KFF — What to Know About the BALANCE Model for GLP-1s in Medicare and Medicaid and the Medicare GLP-1 Bridge
- U.S. News / KFF Health News — CMS Extends Medicare’s Short-Term Bridge Program for GLP-1 Obesity Drug Coverage (Apr 27, 2026)
- AJMC — What You Need To Know Before the Medicare GLP-1 Bridge Goes Live
- FDA / Eli Lilly — Foundayo (orforglipron) Prescribing Information; DailyMed
- Eli Lilly — FDA approves Lilly’s Foundayo (orforglipron) (Apr 1, 2026)
- Drugs.com — Foundayo (orforglipron) FDA Approval History
- Eli Lilly — Foundayo Coverage & Savings terms
- LillyDirect — Foundayo
- GoodRx — Foundayo prices and side effects
- Ro — Weight Loss Program pricing and insurance; how to get Foundayo (sponsored affiliate link, opens in a new tab)
- Sesame Care — Foundayo and online weight-loss program (sponsored affiliate link, opens in a new tab)
All coverage terms, prices, and program dates verified June 4, 2026. The Bridge doesn’t open until July 1, 2026; confirm program status and your eligibility through CMS or your plan before your appointment.