Editorial Standards · Affiliate Disclosure · Next audit: July 29, 2026
Published:
WEGOVY CARDIOVASCULAR PA — 2026 VERIFIED GUIDE
Wegovy Heart Disease Prior Authorization: The 2026 Approval Playbook
Bottom line
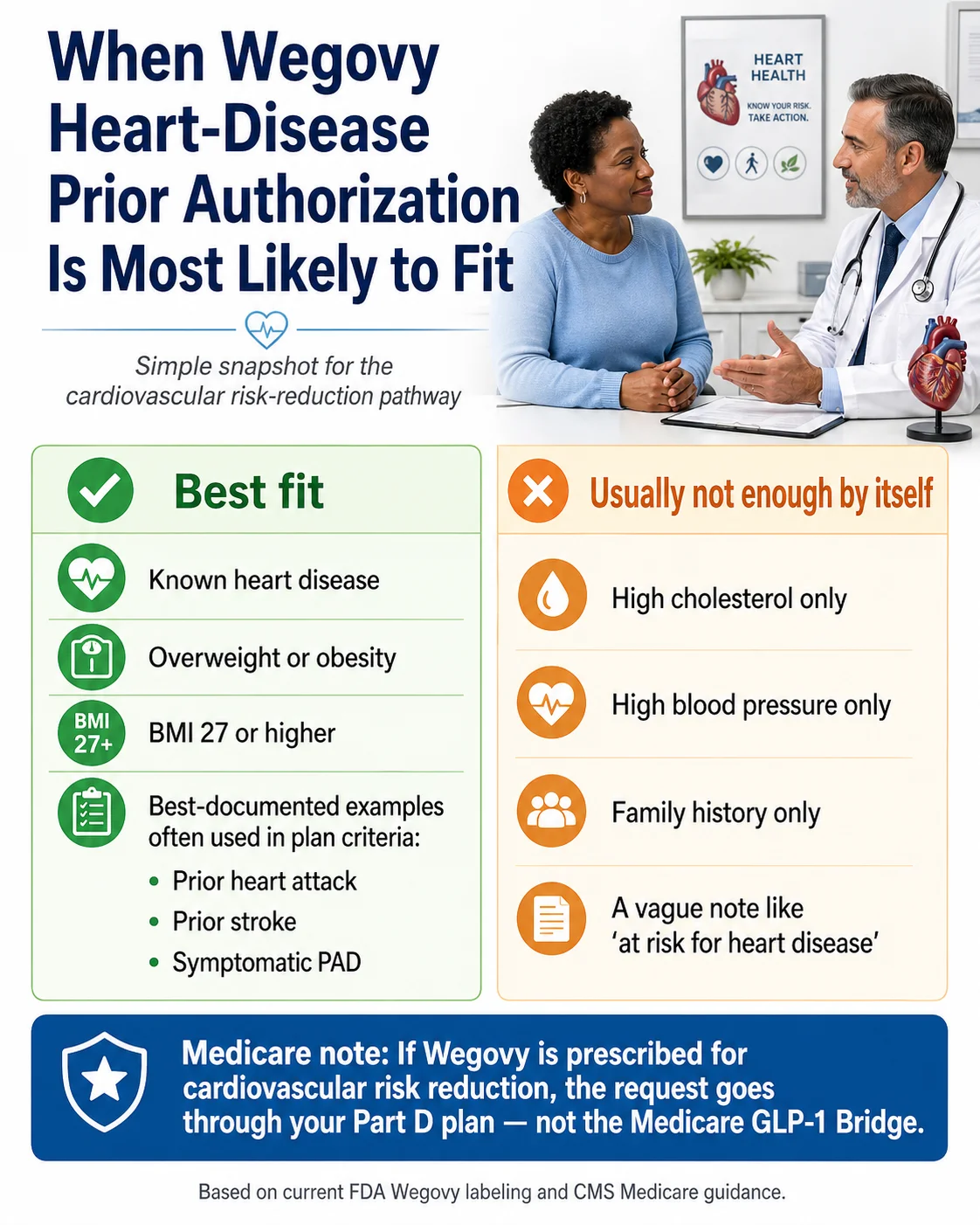
Wegovy heart disease prior authorization is approved most often when the request is framed as cardiovascular risk reduction — not weight loss — and the chart shows established cardiovascular disease (a prior heart attack, prior stroke, or symptomatic peripheral artery disease) plus a BMI of 27 or higher. Risk factors alone — high cholesterol, high blood pressure, family history — usually aren't enough on this pathway.
Plans differ on a few quiet details that quietly kill PAs: type 2 diabetes carve-outs, the BMI documentation date, whether a cardiologist must be involved, and whether the request was submitted under the cardiovascular indication or the weight-loss benefit. The fastest way through this, if you don't want to coordinate it yourself, is Ro's insurance concierge.
Here's the part almost every other page skips: the FDA approving Wegovy for heart disease in March 2024 didn't make insurance coverage automatic. Insurers wrote their own rules on top of the FDA label — and those rules are where most people get stuck. We pulled the public prior-authorization policies from UnitedHealthcare, Aetna/CVS Caremark, Wellmark, CareFirst, and Highmark, plus the CMS Medicare guidance, and what we found is that the same diagnosis can sail through one plan and get rejected by another for reasons nobody mentioned at your appointment.
This is the playbook to fix that.
Will the Wegovy heart-disease PA path probably work for you?
Find your situation in the table. The “best next step” column tells you where to focus energy — before you spend a dollar or a week on paperwork.
| Your situation | What it likely means | Main denial risk | Best next step |
|---|---|---|---|
| Prior heart attack, stroke, or symptomatic PAD + BMI ≥27 | Strongest match to public CV-risk PA criteria | Missing GDMT documentation; old BMI date | Gather cardiology records and a current BMI; ask prescriber to submit under cardiovascular risk reduction |
| High cholesterol, high blood pressure, family history, or “at risk” only | The CV pathway often won't apply — risk factors aren't established CVD | Submitted as CV when chart only shows risk factors | Pursue weight-management coverage if eligible, or take the GLP-1 path quiz |
| Type 2 diabetes + established CVD | Several plans carve T2D out of the Wegovy CV pathway | Diabetes carve-out — plan steers to a diabetes-indicated GLP-1 instead | Ask whether Ozempic (semaglutide for T2D, FDA-labeled MACE reduction) fits your plan |
| Medicare Part D + established CVD + BMI ≥27 | Wegovy CV coverage may be available — through your Part D plan, not the GLP-1 Bridge | Plan hasn't added Wegovy to its 2026 formulary | Check Medicare.gov Plan Finder, then call the plan to confirm CV-indication PA criteria |
| Already denied as “weight loss not covered” | Likely submitted under the wrong benefit or missing CVD records | Wrong indication framing | Re-read the denial letter; resubmit under the CV indication with cardiology records attached |
 (sponsored affiliate link, opens in a new tab)
(sponsored affiliate link, opens in a new tab)Tap to check your Wegovy coverage on Ro — free, no commitment required
Ro states it can't currently help coordinate GLP-1 coverage for government insurance plans. Medicare and Medicaid readers, see the Medicare Part D section below.
🛡️ What we actually verified for this guide
Last verified: April 29, 2026. We reviewed the current Wegovy prescribing information and the FDA's March 2024 cardiovascular indication update; the SELECT trial as published in NEJM; the CMS Medicare GLP-1 Bridge guidance; NovoMedLink PA resources; and the public Wegovy CV-indication PA policies from UnitedHealthcare, Aetna, CVS Caremark, Wellmark, and CareFirst/Maryland Medicaid.
Payer policies vary by plan, employer, state, and benefit design. This guide is a preparation tool — not a coverage guarantee.
What “heart disease” actually means to your insurance company (it's stricter than you think)
Insurers don't approve Wegovy for “heart disease” the way most people use that phrase. They approve it for established cardiovascular disease — and that distinction is where a meaningful share of the denials we reviewed originate. If your chart says “history of high cholesterol” but doesn't show a documented event, you're probably going to hit a wall on this pathway.
The FDA-approved cardiovascular indication for Wegovy, finalized in March 2024, applies to adults with established cardiovascular disease and either obesity or overweight — to reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke). The clinical evidence is the SELECT trial: 17,604 adults with prior CVD and BMI ≥27 (no diabetes), followed for an average of about 40 months, with a 20% reduction in major adverse cardiovascular events versus placebo. That trial is the spine of every CV-indication PA approval today.
What insurers count as established CVD
| Stronger evidence | Why insurers accept it |
|---|---|
| Prior myocardial infarction (heart attack) | Listed in nearly every CV-indication policy; matches SELECT trial enrollment criteria. |
| Prior ischemic or hemorrhagic stroke | Listed in nearly every CV-indication policy. |
| Symptomatic peripheral artery disease (PAD) | Usually requires symptomatic PAD with supporting evidence: an abnormal ankle-brachial index (ABI), prior revascularization, or amputation history. The word “symptomatic” matters — asymptomatic PAD on imaging often doesn't qualify by itself. |
| Prior coronary revascularization (CABG, PCI/stent) | Aetna, CVS Caremark, and several others count prior coronary artery bypass graft, percutaneous coronary intervention, or angioplasty as qualifying CVD. |
What usually does not count by itself
| Weaker evidence alone | Why it often fails the CV pathway |
|---|---|
| High cholesterol (hyperlipidemia) | Risk factor — not established disease. |
| High blood pressure (hypertension) | Risk factor — not established disease. |
| Family history of cardiac events | Risk indicator, not your medical event. |
| Generic “at risk for heart disease” chart note | Too vague for nearly every reviewer. |
| Obesity alone | Routes the request to weight-management benefits, which are excluded on many plans. |
| Asymptomatic atherosclerosis on imaging only | Some plans accept this if the imaging is robust; many do not. |
The single most useful idea on this page: the strength of your PA case is determined by the specific cardiovascular event your chart documents, not by your overall heart-disease risk profile. Two patients with identical cholesterol numbers will get different answers from the same insurer if one has a 2022 MI in their cardiology records and the other doesn't.
Wegovy heart disease PA criteria crosswalk: what 6 major payers actually require
We assembled this table because the information doesn't exist anywhere else in one place. To get this on your own, you'd need to download UnitedHealthcare's commercial PA bulletin, Aetna's clinical policy bulletin 6410-C, CVS Caremark's 4774-C document, Wellmark's supplemental indications policy, CareFirst/Maryland Medicaid's Wegovy criteria, and Highmark's PA form — and read each one front to back.
| Payer / Source | Age gate | BMI | Required CVD evidence | T2D carve-out? | GDMT required? | Approval length | Key hidden friction |
|---|---|---|---|---|---|---|---|
| FDA / Wegovy label | Adult | ≥27 | Established CVD | No | Diet + activity | N/A | FDA eligibility ≠ insurance approval |
| UnitedHealthcare commercial | 45+ | ≥27 | Prior MI, stroke, or symptomatic PAD with ABI / revascularization / amputation evidence | Yes — excludes T2D or HbA1c >6.5 | Yes — event-specific therapy unless contraindicated | 12 months | NYHA Class IV heart failure also excluded |
| Aetna (non-Medicare) | Adult | ≥27 | Prior MI, stroke, symptomatic PAD, or CABG/PCI/angioplasty | Yes — must NOT have T2D | Yes — GDMT or documented reason | 7 months initial, 12 months continuation | Missing GDMT documentation is the leading friction point |
| CVS Caremark | Adult | ≥27 | Prior MI, stroke, PAD, or revascularization | Yes — must NOT have T2D | Yes — GDMT or documented reason | 12 months | Strong criteria match but documentation is mandatory |
| Wellmark | Specialist prescriber restriction | ≥27, recent documentation | Chart notes / claims for prior MI, stroke, or PAD | Yes — must not have T2D | Yes — standard CVD care or documented exception | 6 months | Pancreatitis within last 180 days excluded; specialist requirement; recent BMI date |
| CareFirst / Maryland Medicaid | 18+ | ≥27 within last 90 days | Documented ASCVD: prior MI, stroke, or symptomatic PAD | Not the headline friction | Must be by or in consultation with a cardiologist | Verify on current policy | Cardiologist involvement is mandatory; recent BMI must be on file |
| Highmark (form analyzed) | Plan-dependent | Baseline / current BMI requested | Form asks specifically: prior stroke, prior MI, PAD | Asks about diabetes-indicated GLP-1 alternatives | Asks about statin / ezetimibe / PCSK9 + CV risk-factor management | Plan-dependent | Form questions reveal what the plan expects even when full policy isn't public |
| Medicare Part D (CMS guidance) | Per plan | ≥27 typical | Established CVD per FDA label | Per plan | Per plan | Commonly 12 months | Coverage is plan-by-plan; not all Part D plans have added Wegovy CV |
What this table actually tells you
1. “Heart disease” is too broad — say “established cardiovascular disease”
Every PA we reviewed uses some version of that phrase. If your prescriber's note says “patient has heart disease,” it's weaker than “patient has documented coronary artery disease, status post MI [date].”
2. “For weight loss” is the wrong framing here
This is the most common preventable reason a CV-indication PA fails. The request should be submitted as cardiovascular risk reduction, with diagnosis coding that accurately reflects the documented cardiovascular condition. Ask your plan whether it requires the cardiovascular ICD-10 code as primary.
3. BMI still matters — even on the CV pathway
Almost every plan requires BMI ≥27, and several (CareFirst, Wellmark) want it documented recently — within 90 days. A two-year-old BMI in your chart can fail you.
4. Type 2 diabetes is a real carve-out on several major plans
Aetna, CVS Caremark, Wellmark, and UnitedHealthcare commercial plans all explicitly carve T2D patients out of the Wegovy CV-risk pathway. If you have diabetes, your plan may steer you to Ozempic, which carries an FDA-labeled MACE indication for adults with T2D and established CVD.
5. Standard cardiac therapy (GDMT) needs to be documented
Guideline-directed medical therapy — usually a statin and an antiplatelet at minimum — must be on the medication list, or your prescriber needs to document why a specific agent is contraindicated or not tolerated. Skipping this is a leading reason an otherwise solid Aetna or CVS Caremark CV PA gets denied.
6. Approval length varies more than you'd think
UHC and Caremark approve for 12 months; Aetna gives 7 then 12; Wellmark approves for 6 months. Mark your calendar — a missed renewal can be just as painful as a missed initial PA.
The doctor's CV-indication submission cheat sheet (print this and bring it)
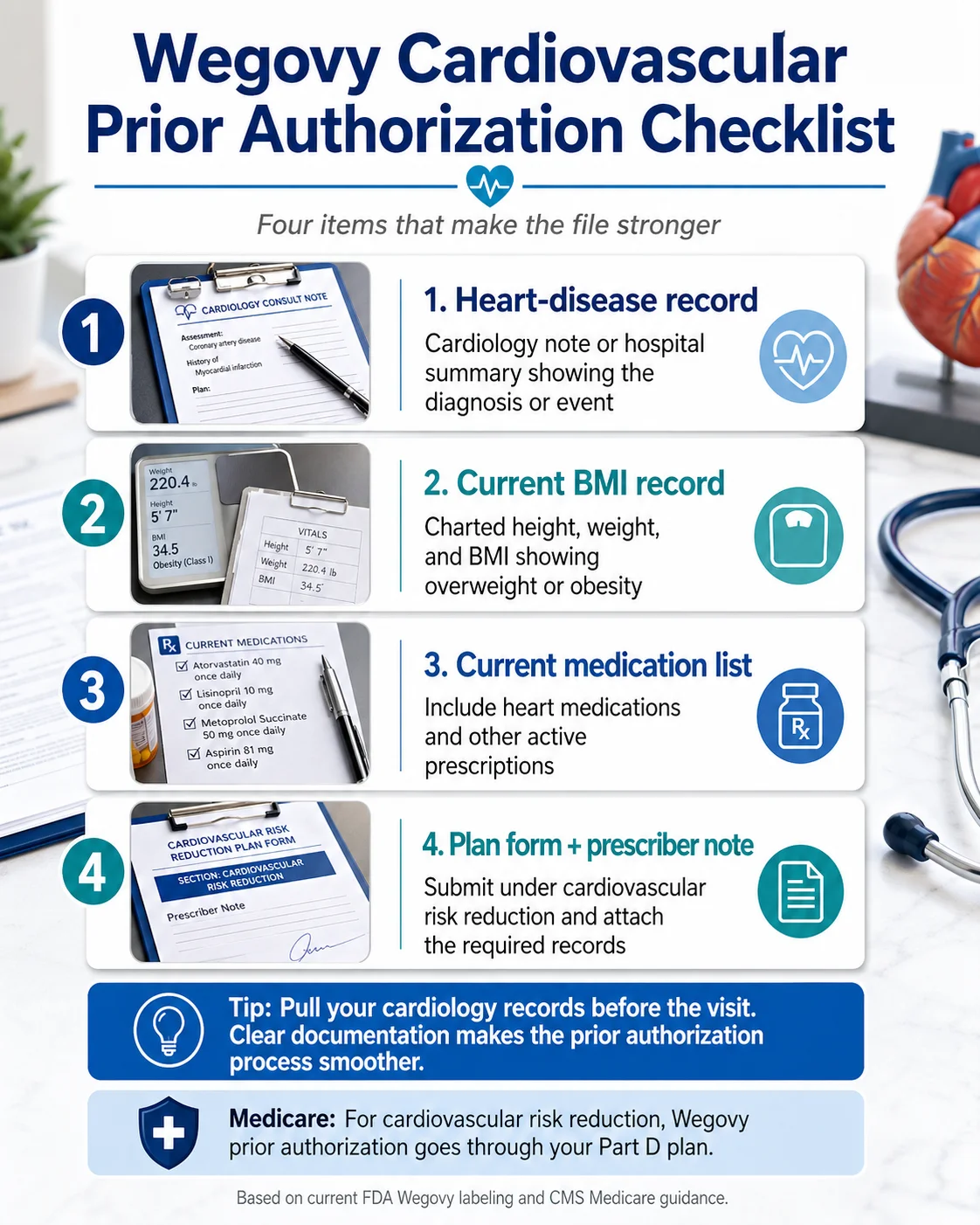
A Wegovy PA submitted under the cardiovascular indication needs four things every reviewer looks for: diagnosis coding that accurately reflects the documented cardiovascular condition, a current BMI of 27 or higher with the date measured, documentation of established CVD with the event date, and a current medication list showing standard cardiac therapy (or a documented reason for any missing agent). If even one is missing, expect a denial or a request for more information.
 (sponsored affiliate link, opens in a new tab)
(sponsored affiliate link, opens in a new tab)Tap to check whether Ro's PA team can handle this for you
The 4 things every CV-indication PA should contain
- Diagnosis coding accurate to the chart. Submit under the cardiovascular-risk-reduction indication with diagnosis coding that matches the patient's documented cardiovascular condition and overweight/obesity status. Ask your plan whether the cardiovascular code must be primary and which codes it expects on its form.
- BMI documented at time of prescription, calculated from a measured height + weight in the chart.
- Documentation of established CVD with event date(s) — the cardiology consult or hospital discharge summary is the strongest source.
- Concurrent guideline-directed medical therapy (GDMT) — statin, antiplatelet, beta-blocker / ACE-ARB / ARNI as appropriate — or a documented reason for any agent that's not in the regimen.
ICD-10 codes commonly used (discuss with your prescriber and your plan)
Note: These are examples your prescriber may consider when they accurately match the documented chart. Don't code from this table alone — use your plan's PA form, the patient's actual medical record, and your prescriber's clinical judgment. NovoMedLink lists invalid diagnosis codes among the most common Wegovy PA denial reasons — so this is worth getting right.
| Condition | Example primary code | Example secondary BMI code |
|---|---|---|
| Recent heart attack (<4 weeks) | I21.x — Acute MI | E66.01 (BMI ≥30) or Z68.27 (BMI 27–29.9) |
| Prior heart attack (>4 weeks) | I25.2 — Old MI | E66.01 / Z68.27 |
| Prior ischemic stroke | I63.9 — Cerebral infarction unspecified | E66.01 / Z68.27 |
| Coronary artery disease (no MI) | I25.10 — ASHD without angina | E66.01 / Z68.27 |
| Symptomatic PAD | I73.9 — Peripheral vascular disease | E66.01 / Z68.27 |
| Prior stent (PCI) | Z95.5 — Presence of coronary stent | E66.01 / Z68.27 |
| Prior CABG | Z95.1 — Presence of coronary bypass | E66.01 / Z68.27 |
⚠ The coding mistake we see most
When obesity is listed as the primary diagnosis on a CV-indication PA, the request often gets routed to the weight-loss benefit — which Medicare excludes by federal statute and many commercial plans exclude by carve-out. That's a denial that's preventable in the chart, not at appeal. Ask your plan how it wants the diagnosis coded for the cardiovascular indication.
Letter of Medical Necessity (LMN) skeleton
Bring this template to your appointment so the prescriber can adapt it to your actual records. Don't add diagnoses, medications, or history that aren't documented in your chart.
[Date] [Insurer Medical Director / PA Department] RE: Prior Authorization for Wegovy® (semaglutide) Patient: [Name], DOB [date], Member ID [number] Dear Reviewer, I am requesting prior authorization for Wegovy under the cardiovascular risk reduction indication (FDA-approved March 2024) for my patient, who meets the FDA-labeled criteria as follows: • Established cardiovascular disease: [diagnosis + ICD-10 code + event date — e.g., "Prior MI, I25.2, documented [date], see attached cardiology note"] • BMI: [measured value] (recorded [date]) • Concurrent cardiac therapy: [statin name/dose, antiplatelet name/dose, beta-blocker/ACE-ARB/ARNI as appropriate, OR a documented contraindication or intolerance] • Lifestyle modification: [diet + activity counseling, dates] The SELECT trial (Lincoff et al., NEJM 2023) demonstrated a 20% relative risk reduction in major adverse cardiovascular events in adults with this clinical profile. Attachments: ☐ Cardiology consult note(s) / hospital discharge summary ☐ Most recent BMI documentation (height + weight + date) ☐ Current medication list ☐ Recent labs (lipid panel, A1C, eGFR) ☐ Lifestyle modification documentation ☐ [Insurer-specific PA form, completed] [Provider name], [credentials], NPI [number] [Signature, date]
Documentation checklist
- ☐Cardiology consult note OR hospital discharge summary documenting the CVD event with date
- ☐Most recent BMI (height + weight in chart, ideally within 90 days)
- ☐Current medication list (statin, antiplatelet, beta-blocker / ACE-ARB / ARNI as appropriate)
- ☐Recent labs — lipid panel, A1C if relevant, eGFR
- ☐Lifestyle modification documentation (RD referral, exercise log, weight-management visit notes)
- ☐Prior weight-loss medication trials, if relevant
- ☐Insurer-specific PA form (most insurers accept ePA via CoverMyMeds)
- ☐If PAD: ABI result, revascularization record, or amputation history
- ☐If denied previously: copy of the denial letter so the appeal addresses it line-by-line
Why Wegovy heart disease PAs get denied — and the exact fix for each one
Most denials on the cardiovascular pathway trace back to one of six specific causes — usually a missing record or wrong-indication framing rather than true ineligibility. A denial letter looks scary but it's not the end. It's a checklist of what your plan didn't see. Read the exact reason in the letter — not just the headline — and treat it as a punch list.
1. “Insufficient documentation of cardiovascular disease”
What it means: The chart note didn't clearly state the CVD diagnosis with an ICD-10 code and event date.
Fix: Attach the cardiology consult note or hospital discharge summary directly. Have the prescriber's appeal letter state plainly: “Patient has documented [diagnosis] confirmed [date], ICD-10 [code]. See attached cardiology note.” For PAD specifically, attach the ABI result or vascular procedure note.
2. “BMI not documented at time of prescription”
What it means: The visit note didn't include a measured BMI, or the BMI on file is too old.
Fix: Have the patient return for a quick weight/height measurement. Document it in the chart with the date. Resubmit. Several plans (CareFirst notably) require the BMI to be within 90 days.
3. “Submitted as weight-loss / weight-loss drugs excluded”
What it means: The PA was processed under the obesity benefit instead of the cardiovascular indication. This is one of the highest-volume preventable issues flagged by NovoMedLink's PA resource.
Fix: Resubmit framed as cardiovascular risk reduction. Use diagnosis coding that accurately reflects the documented cardiovascular condition, with the cardiovascular code as primary if your plan requires it. Cite the SELECT trial in the LMN. Include cardiology records.
4. “Concurrent standard-of-care therapy not documented”
What it means: The reviewer didn't see evidence the patient is on guideline-directed medical therapy — typically a statin and an antiplatelet at minimum.
Fix: Attach the current medication list. If the patient has a documented contraindication or intolerance (statin myopathy, aspirin allergy), document it explicitly. “Patient is statin-intolerant per [date] visit, on ezetimibe instead” satisfies the requirement on most plans.
5. “Diabetes carve-out applies”
What it means: Your plan specifically excludes type 2 diabetes patients from the Wegovy cardiovascular pathway and routes them to a diabetes-indicated GLP-1 instead. This is real on Aetna, CVS Caremark, Wellmark, and UnitedHealthcare commercial plans.
Fix: This often isn't a fix — it's a re-route. Ask the prescriber whether Ozempic (semaglutide for T2D) or Mounjaro fits your plan's criteria. Some plans approve those with much less friction than Wegovy CV for T2D patients.
6. “Wegovy not on formulary / formulary exclusion”
What it means: The drug isn't on the formulary at all on this plan, regardless of indication.
Fix: Submit a formulary exception request (non-formulary medical exception), not just a PA. The exception request cites medical necessity and the unavailability of an equivalent covered alternative. For Medicare Part D, this triggers the formal Coverage Determination process.
The peer-to-peer review — the underused move
If a denial looks wrong on its face, your prescriber can request a peer-to-peer (P2P) review — a brief phone call, usually 10–15 minutes, with the insurance medical director. P2P calls reverse a meaningful share of borderline denials, often without a formal appeal. Your prescriber's office has to actively request it; many won't unless you ask.
External review — the option after internal appeals fail
Once internal appeals are exhausted, you can request an external review by an independent third party. For ACA-regulated commercial plans, this is a federal right; for Medicare, this is the IRE (Independent Review Entity) step. KFF found that 80.7% of appealed Medicare Advantage prior-authorization denials were fully or partly overturned in 2024 — but only 11.5% of denials were appealed in the first place. A first denial isn't a final answer, but most patients leave the appeal on the table.
One honest trade-off we want you to know about before you go further
Even when your PA is approved, your monthly cost depends entirely on your plan's tier structure, deductible, and savings-card eligibility. Wegovy on a commercial plan can cost very little or several hundred dollars out of pocket, depending on those variables. The Wegovy savings card may reduce eligible commercially insured patients' cost to as little as $25 per prescription — but it doesn't apply to Medicare, Medicaid, TRICARE, or other government programs. And if your “heart disease” is actually borderline-high blood pressure or one borderline lipid panel, the CV-indication path won't open even with perfect paperwork. The criteria require established disease, not risk factors.
Ro doesn't offer the cheapest cash-pay GLP-1 on the market. If your only priority is the lowest absolute monthly bill and you're willing to skip insurance entirely, NovoCare lists the Wegovy injection at $199/month for early starter doses (through December 31, 2026), $349/month for the 0.25 mg through 2.4 mg doses, and $399/month for Wegovy HD 7.2 mg, with Wegovy tablets at $149/month for the 1.5 mg and 4 mg starter doses. But Ro can offer the thing this audience actually needs more: an insurance concierge that helps with the PA submission, follows up with your insurer, and helps with appeals when coverage is denied.
If your priority is the lowest absolute monthly cost and you're willing to skip insurance entirely — read Best Telehealth for Wegovy for self-pay paths →
Medicare Part D vs. the Medicare GLP-1 Bridge — which path pays for Wegovy for heart disease?
The most-confused Medicare question we get
If you have Medicare and you're being prescribed Wegovy for cardiovascular risk reduction, your prior authorization goes through your Medicare Part D plan — not through the Medicare GLP-1 Bridge. CMS has stated explicitly that CV-risk Wegovy uses the standard Part D utilization-management process. The Bridge (July 1, 2026 – December 31, 2027) is for select GLP-1s prescribed for weight management, not the cardiovascular indication. Confusing the two costs people weeks.
Wegovy CV indication on Medicare (Part D path)
When Wegovy is prescribed for cardiovascular risk reduction in an adult with established CVD and BMI ≥27, Medicare Part D plans may cover it — because this is a non-weight-loss indication, it's not blocked by the federal weight-loss drug exclusion at 42 U.S.C. § 1395w-102. Whether your specific Part D plan covers it is a formulary question — coverage and PA criteria vary plan by plan.
Submission goes through your Part D plan's standard PA process. Your prescriber attests that you meet:
- Established cardiovascular disease (with appropriate diagnosis coding)
- BMI ≥27
- Standard cardiac care or documented exception
- Lifestyle modification per FDA label
For Medicare Part D coverage determinations, the plan generally must respond within 24 hours for expedited requests or 72 hours for standard requests. If you're appealing a denial through redetermination, the timeframe is 72 hours expedited or 7 calendar days standard.
Medicare GLP-1 Bridge (the weight-loss path — different program)
The Bridge is a CMS demonstration running July 1, 2026 through December 31, 2027, providing eligible Medicare Part D beneficiaries with a $50 cost-sharing amount for select GLP-1 drugs prescribed to reduce excess body weight. CMS lists the Bridge-covered drugs as Foundayo, Wegovy injection, Wegovy tablets, and Zepbound KwikPen. The Bridge uses a CMS central processor — not your Part D plan — for prior authorization and claims.
If your prescription is for cardiovascular risk reduction, the Bridge isn't your path — your Part D plan is. If you have established CVD and the BMI/diagnosis profile that qualifies under the Bridge, you may have a choice of pathways. Read Medicare GLP-1 Bridge Program Explained → for Bridge eligibility detail.
The 5 levels of Medicare Part D appeal (most patients give up at level 1)
- Redetermination — your plan re-reviews the denial (72 hours expedited / 7 calendar days standard)
- Reconsideration — Independent Review Entity (IRE) review
- Administrative Law Judge (ALJ) hearing — for disputes meeting the dollar threshold
- Medicare Appeals Council review
- Federal District Court
KFF found 80.7% of appealed Medicare Advantage PA denials were overturned in 2024. The lesson: a first denial isn't a final answer.
Should your cardiologist, PCP, or telehealth provider submit the PA?
The best prescriber for your Wegovy CV-indication PA is whoever can document the criteria most completely. A cardiologist usually has the strongest CVD records; a PCP can work if they can pull cardiology notes into the submission; Ro shines when you want the insurance paperwork handled for you on a commercial plan. CareFirst/Maryland Medicaid actually requires cardiologist involvement — check your plan first.
| Your situation | Best first path | Why |
|---|---|---|
| You have a cardiologist with MI / stroke / PAD records on file | Your cardiologist | Strongest access to the documentation insurers ask for. The cardiology note is almost always the most powerful single piece of evidence. |
| Your PCP manages your weight and your heart meds | Your PCP | Works fine if they can attach the cardiology consult or hospital discharge summary. |
| You have commercial insurance and want online help running the coverage check and submitting the PA | Ro | Free GLP-1 Insurance Coverage Checker + insurance concierge support for Body members on commercial plans. |
| You're on Medicare Part D | Your Part D plan + current prescriber | Ro currently can't help coordinate GLP-1 coverage for government insurance plans. |
| You're on FEHB (federal employee plan) | Either your existing prescriber or Ro | Ro's pricing page lists FEHB members as eligible for the insurance concierge. |
| Your plan requires cardiologist involvement (e.g., CareFirst) | Cardiologist | Otherwise the PA gets bounced back regardless of how complete the documentation is. |
Why we feature Ro on this page specifically
This is a page about insurance prior authorization for an FDA-approved brand-name medication. That's the lane Ro leads in among the affiliate options we evaluate.
What Ro publicly offers: a free GLP-1 Insurance Coverage Checker that contacts your insurer and emails a personalized coverage report (including whether PA is required, what your plan covers, expected cost, and supply availability), plus a dedicated insurance concierge that helps Body members with the PA process and appeals. Pricing: $39 first month, then as low as $74/month with annual plan paid upfront, or $149/month month-to-month. Medication cost is separate.
What Ro is not: the cheapest absolute self-pay path (NovoCare wins there), and not the right fit if you want a single named local clinician you can see in person, or if you're on Medicare or Medicaid.
Edge cases: type 2 diabetes, heart failure, and “risk factors only” patients
If you have type 2 diabetes + established CVD
Several major plans (Aetna, CVS Caremark, Wellmark, UnitedHealthcare commercial) explicitly exclude patients with type 2 diabetes from the Wegovy cardiovascular-risk PA pathway. UHC's policy excludes patients with diabetes or HbA1c >6.5%. The reasoning isn't punitive — these plans typically prefer that T2D patients with cardiovascular disease use a diabetes-indicated therapy.
What to do: Ask your prescriber whether Ozempic (semaglutide for T2D) fits your plan's criteria — Ozempic carries an FDA-labeled MACE-reduction indication for adults with type 2 diabetes and established CVD, and that's exactly what payer policies reference for re-routing.
If you have NYHA Class IV heart failure
UnitedHealthcare's commercial CV-indication policy specifically excludes NYHA class IV heart failure patients from the Wegovy cardiovascular pathway. Other plans may or may not have similar exclusions — verify with your specific plan. Talk to your cardiologist about whether the exclusion applies to your clinical profile.
If you have a recent history of pancreatitis
Wellmark's policy includes exclusion language for pancreatitis within the last 180 days. Document the date of the pancreatitis episode, current resolution status, and any specialist clearance. Some plans will accept GLP-1 therapy after a documented recovery period; ask your gastroenterologist or cardiologist before pursuing the PA.
If you have only risk factors (high cholesterol, hypertension, family history)
This is the most common “false positive” we see. People hear that insurance covers Wegovy for heart disease and assume risk factors qualify. They almost never do on this pathway. The CV indication requires documented established disease — a prior event or confirmed diagnosis — not modifiable risk factors.
- If you have insurance that covers weight-loss medications: pursue the weight-loss PA pathway separately. Many commercial plans cover Wegovy for chronic weight management at BMI ≥27 with one weight-related comorbidity (which can include hypertension or hyperlipidemia).
- If you have Medicare and want Wegovy for weight loss: the Medicare GLP-1 Bridge (July 2026 – December 2027) may apply. See Medicare GLP-1 Bridge Program Explained →
- If you're paying out of pocket: see Best Telehealth for Wegovy →
If you have prediabetes
Prediabetes typically doesn't trigger the diabetes carve-out (which is usually triggered by A1C ≥6.5% or a documented T2D diagnosis). But verify — some plans use HbA1c >6.0% as the cutoff. If you're borderline, the prescriber's note should reflect your most recent HbA1c clearly.
If you have prior revascularization but no documented MI/stroke
Some plans (Aetna, CVS Caremark) explicitly count prior CABG, PCI, or angioplasty as qualifying CVD. Others focus on prior MI/stroke/PAD as the trio. Check your plan's specific language before submitting. If your CABG or stent is your only CVD evidence, make sure your plan accepts it.
How long Wegovy PA takes — and how long your approval lasts
Plan for 1–2 weeks from your prescriber submitting a clean Wegovy PA to your prescription being filled on a commercial plan. Medicare adds a few days. If you're denied and have to appeal, add 30–60 days. Initial approval lengths range from 6 months (Wellmark) to 12 months (UHC, CVS Caremark). Mark your calendar — missed renewals cause coverage gaps as painful as missed initial PAs.
| Step | Commercial plan | Medicare Part D |
|---|---|---|
| Prescriber submits PA | Day 0 | Day 0 |
| Initial coverage determination | 1–7 days (some auto-approve same day) | 24 hrs expedited / 72 hrs standard |
| Pharmacy fills Rx | +2–3 days after approval | +2–3 days |
| Redetermination if denied | +14–30 days | 72 hrs expedited / 7 calendar days standard |
| Total best case | 5–10 days | 4–8 days |
| Total with appeal | 30–60 days | 90–120 days through later levels |
Approval lengths by insurer
| Payer | Initial approval | Continuation |
|---|---|---|
| UnitedHealthcare commercial | 12 months | 12 months |
| Aetna (non-Medicare) | 7 months | 12 months |
| CVS Caremark | 12 months | 12 months |
| Wellmark | 6 months | Plan-dependent |
| CareFirst / Maryland Medicaid | Verify on current policy | Verify on current policy |
| Medicare Part D | Plan-dependent (commonly 12 months) | Plan-dependent |
Renewal checklist (so you don't lose coverage at month 6 or month 7)
- ☐You still meet initial CV indication criteria
- ☐Current BMI documented (within 90 days for stricter plans)
- ☐Continued therapy documented in chart
- ☐Medication adherence confirmed (most plans want this)
- ☐No new exclusion (e.g., new T2D diagnosis on a plan with the carve-out)
- ☐Continued GDMT or documented exception
Real voices: what people are actually confused about
Direct quotes from real patients navigating this problem — included as voice-of-customer evidence, not medical or insurance authority.
“Has anyone had success with getting Wegovy covered for heart disease even if your insurance doesn't cover weight loss meds?”— r/WegovyWeightLoss, January 2025
“I have high cholesterol and still was denied.”— r/WegovyWeightLoss
“My prior authorization for Wegovy was denied yesterday. CVS Caremark advised this plan requires 6 months in a comprehensive weight loss plan…”— r/fednews, January 2025
The first poster's question is exactly what this page is for: yes, it's possible — when the PA is submitted under the cardiovascular indication and the chart shows established CVD. The second poster ran into the most common trap: high cholesterol alone is a risk factor, not established CVD, and most plans won't approve the CV pathway on risk factors alone. The third poster's denial was processed under the weight-loss benefit — a different submission framing might unlock the same plan.
“Wegovy has been the most positive life-changing medication I have ever used.”— Drugs.com user review
⚠️ Results aren't typical, and user reviews don't constitute clinical evidence. Wegovy is FDA-approved as an adjunct to a reduced-calorie diet and increased physical activity. For clinical evidence on the cardiovascular indication, see the SELECT trial (Lincoff et al., NEJM 2023) and the Wegovy prescribing information.
Your 7-step action plan, starting today
- 1Call your insurer or use the member portal to request the Wegovy prior authorization criteria. Ask specifically for the cardiovascular indication criteria (not the weight-loss criteria). Save the document.
- 2Confirm whether your plan has the diabetes carve-out if you have type 2 diabetes. If yes, ask whether Ozempic (under the diabetes indication) is the better path.
- 3Pull your CVD records. Your cardiology consult note or hospital discharge summary is your single strongest piece of evidence. Get a copy before your prescriber appointment.
- 4Get your most recent BMI documented (within 90 days if you're on a strict plan like CareFirst or Wellmark). A quick in-office weight and height check suffices.
- 5Confirm your current cardiac meds list — statin, antiplatelet, beta-blocker / ACE-ARB / ARNI as appropriate. If anything is missing, your prescriber needs a documented reason.
- 6Ask the prescriber to submit under the cardiovascular indication with diagnosis coding that accurately matches your records. Bring the cheat sheet from this guide.
- 7If denied, read the denial letter carefully and resubmit or appeal addressing the specific reason cited. The peer-to-peer review and external review options are real — use them.
Frequently asked questions about Wegovy heart disease prior authorization
Does Medicare cover Wegovy for heart disease in 2026?
Medicare Part D plans may cover Wegovy under the cardiovascular indication for adults with established cardiovascular disease and BMI ≥27, but coverage is plan-by-plan and almost always requires prior authorization. Medicare cannot cover Wegovy for weight loss alone due to federal statute (42 U.S.C. § 1395w-102). Use Medicare.gov Plan Finder to check your specific plan's formulary, then call the plan to confirm the cardiovascular-indication PA criteria.
What heart conditions qualify for Wegovy CV-indication coverage?
Insurers consistently accept four established cardiovascular disease diagnoses: prior myocardial infarction, prior ischemic stroke, symptomatic peripheral artery disease, and prior coronary revascularization (CABG or PCI/stent). Some plans also accept other forms of documented atherosclerotic disease. Risk factors alone — high blood pressure, high cholesterol, family history — usually do not qualify for the cardiovascular indication.
Is the CV indication easier to get approved than the weight-loss indication?
On Medicare and on commercial plans with weight-loss carve-outs, often yes — the CV indication uses cardiovascular coverage rules rather than obesity exclusions, and step therapy is less common on the CV pathway. The exception: plans with a type 2 diabetes carve-out (Aetna, CVS Caremark, Wellmark, UnitedHealthcare) can make the CV pathway harder for diabetic patients, who are often routed to a diabetes-indicated GLP-1 instead.
How long does Wegovy prior authorization take?
One to seven days for commercial plans with clean documentation — some auto-approve same day if criteria match. Medicare Part D coverage determinations require a response within 24 hours for expedited requests or 72 hours for standard requests. If denied and appealing, redetermination takes 72 hours expedited or 7 calendar days standard, with later Medicare appeal levels adding additional weeks. If you need to appeal at the commercial-plan level, add 30–60 days.
What ICD-10 code should my doctor use for the Wegovy CV indication?
The prescriber should use diagnosis coding that accurately matches the documented chart and the plan's PA form. Cardiovascular codes commonly used include I25.10 (coronary artery disease without angina), I25.2 (old MI), I63.9 (cerebral infarction), and I73.9 (peripheral artery disease). Obesity codes (E66.x) and BMI codes (Z68.x) are typically secondary. Ask your plan explicitly how it wants the diagnosis coded for the cardiovascular indication — incorrect primary coding is the single most common preventable denial reason.
Why was my Wegovy PA denied as 'weight loss' when I have heart disease?
The prescriber likely submitted with diagnosis coding that routed the request to the weight-loss benefit, which is excluded on many plans. Resubmit framed as cardiovascular risk reduction with diagnosis coding that accurately reflects your documented cardiovascular condition, attach your cardiology records, and reference the cardiovascular indication explicitly. This is not an appeal — it can be submitted as a new PA under the correct indication.
Does the Medicare GLP-1 Bridge handle Wegovy heart-disease prior authorization?
No. CMS has stated that Wegovy prescribed for cardiovascular risk reduction goes through the beneficiary's Medicare Part D plan's standard utilization-management process, not the Bridge program processor. The Medicare GLP-1 Bridge (July 1, 2026 – December 31, 2027) is a separate CMS demonstration for select GLP-1 drugs prescribed for weight management — a different indication.
Can I get Wegovy without insurance using the CV indication?
You can — but the CV indication doesn't change the cash price. NovoCare lists the Wegovy injection at $199/month for early starter doses (through December 31, 2026), $349/month for the 0.25 mg through 2.4 mg doses, and $399/month for Wegovy HD 7.2 mg, with Wegovy tablets at $149/month for the 1.5 mg and 4 mg starter doses. Insurance is typically the only way the price drops below ~$200/month for ongoing maintenance dosing.
Does Wegovy tablet coverage work the same as Wegovy injection for heart-disease PA?
Both Wegovy injection and Wegovy tablets are FDA-labeled for cardiovascular risk reduction in adults with established cardiovascular disease and overweight or obesity. Plan formularies may treat the tablet and injection differently — different tiers, different PA forms, different step-therapy rules — so ask your plan whether it covers Wegovy tablets, Wegovy injection, or both for the cardiovascular indication.
Does Ro submit prior authorization for Wegovy?
Ro states that Body members can contact its insurance concierge and that the team helps members with the insurance process when GLP-1 coverage requires it, including appeal support when coverage is denied. Ro currently cannot help coordinate GLP-1 medication coverage for government insurance plans (Medicare/Medicaid); FEHB members are eligible per Ro's pricing page. Ro's free GLP-1 Insurance Coverage Checker (no membership required to use) contacts your insurer and emails a personalized coverage report.
How much does Ro cost?
Ro Body is $39 for the first month, then as low as $74/month with annual plan paid upfront, or $149/month month-to-month. Medication cost is separate; Ro states its FDA-approved medication prices match NovoCare, LillyDirect, and TrumpRx pricing where applicable.
What's the SELECT trial and why does my insurer care?
SELECT is the Phase 3 trial Novo Nordisk submitted to the FDA, showing semaglutide 2.4 mg reduced major adverse cardiovascular events by 20% in 17,604 adults with established CVD and BMI ≥27 over an average of about 40 months. The FDA used SELECT to expand Wegovy's label in March 2024, creating the cardiovascular indication. Every PA reviewer who approves a Wegovy CV-indication request is relying on SELECT as the evidence base.
Does Wegovy replace my heart medications?
No. Wegovy is added to standard cardiac therapy, not in place of it. Several PA criteria explicitly require documentation that the patient is on guideline-directed medical therapy (statin, antiplatelet, etc.) or has a documented reason for any agent that's not in the regimen.
Still not sure which GLP-1 path fits your situation?
The criteria here cover the majority of cases, but every reader's specific combination of insurance, conditions, and history is different. If your plan has a wrinkle we didn't cover — or you're not sure whether the CV pathway, the weight-loss pathway, or self-pay makes sense for you — take our free 60-second matching quiz.
If you're ready, here's the lowest-friction first step
You've read the criteria. You know what your plan is likely to ask for. You know the difference between the CV indication and the weight-loss pathway. The remaining question: do you want to coordinate the coverage check and PA submission yourself, or get help from a service that handles this every day?
Ro's free GLP-1 Insurance Coverage Checker is the lowest-commitment first step for commercially insured readers. It contacts your insurer, sends you a personalized coverage report by email, and tells you exactly what your plan requires before you decide on anything else. No membership signup required to use the checker.
About this guide
The RX Index is a pricing intelligence and comparison resource for GLP-1 telehealth providers. We built this guide by reviewing the current Wegovy prescribing information, the FDA's March 2024 cardiovascular approval announcement, the SELECT trial as published in the New England Journal of Medicine, CMS guidance on Medicare Part D coverage and the Medicare GLP-1 Bridge program, NovoMedLink's prior authorization resources, and the public Wegovy prior authorization policies and forms from UnitedHealthcare, Aetna, CVS Caremark, Wellmark, CareFirst/Maryland Medicaid, and Highmark.
Where a specific insurer's criteria are referenced, we link directly to the source policy. This guide is editorial — it is not medical advice, not insurance advice, and not a guarantee of coverage. Your treatment decisions belong to you and a licensed clinician; your coverage decisions belong to your insurer.
Medical disclaimer: This page is for informational purposes only and doesn't constitute medical advice. Wegovy is a prescription medication with a Boxed Warning. Common side effects include nausea, diarrhea, vomiting, constipation, abdominal pain, headache, and fatigue. See the full Wegovy prescribing information for contraindications and complete safety profile. Consult a licensed healthcare provider before starting, changing, or stopping any medication.
Related guides on The RX Index
- Best Telehealth for Wegovy in 2026: Providers Compared
- Best Wegovy Providers 2026: Ranked by Insurance Support
- Medicare GLP-1 Bridge Program Explained
- Does Medicare Cover Wegovy for Weight Loss?
- Blue Cross Wegovy Prior Authorization: 2026 Guide
- Ozempic vs Wegovy: 2026 Verdict + Real Prices
- Best GLP-1 Providers That Accept Insurance (2026)
- GLP-1 Cost Without Insurance: 2026 Real Prices
- Wegovy Pill vs Injection: Cost & Results 2026
Sources
- FDA, FDA Approves First Treatment to Reduce Risk of Serious Heart Problems Specifically in Adults with Obesity or Overweight, March 8, 2024.
- FDA, Wegovy (semaglutide) prescribing information, current label.
- Lincoff AM et al., Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT Trial), New England Journal of Medicine, 2023.
- UnitedHealthcare, Wegovy Cardiovascular Risk Reduction and MASH Only — Prior Authorization / Non-Formulary.
- Aetna, Wegovy (Cardiovascular) PA with Limit, Policy 6410-C.
- CVS Caremark, Wegovy Prior Authorization Criteria, Policy 4774-C.
- Wellmark, Supplemental Indications Policy — Wegovy Cardiovascular-Risk Reduction.
- CareFirst BlueCross BlueShield Maryland Medicaid, Coverage of Wegovy for Overweight or Obese Adults with Cardiovascular Disease, PT35-25.
- Highmark, Wegovy Prior Authorization Form.
- NovoMedLink, Initiating a Wegovy Prior Authorization — provider resource.
- CMS, Medicare GLP-1 Bridge program guidance and FAQ.
- KFF, Medicare Advantage Insurers Made Nearly 53 Million Prior Authorization Determinations in 2024.
- NovoCare, Wegovy Cost, Coverage, & Savings Resources.
- Ro, GLP-1 Insurance Coverage Checker (sponsored affiliate link, opens in a new tab) and Weight Loss Program Pricing (sponsored affiliate link, opens in a new tab) — verified April 29, 2026.
All sources reviewed and verified April 29, 2026. Payer policies are updated frequently; we re-verify quarterly and update the “Last verified” date at the top of this page when changes are made.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup