What Happens When You Stop GLP-1?
By The RX Index Editorial Team
Published:
Last verified:
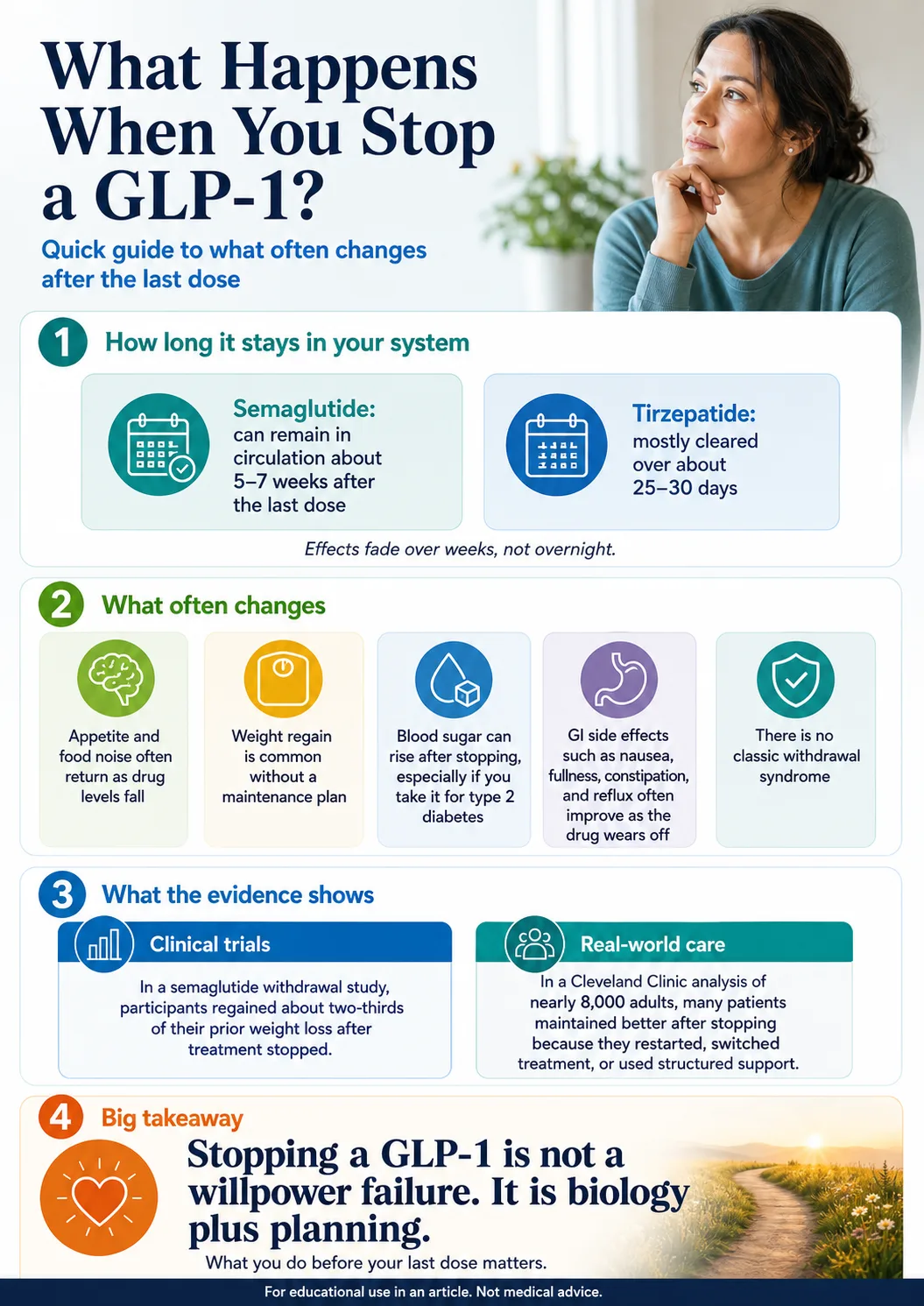
What happens when you stop GLP-1 is not a mystery — but it is medical. Weekly GLP-1s fade over weeks, not overnight. Semaglutide can stay in circulation for 5 to 7 weeks after the last dose. Tirzepatide has a 5-day half-life and is mostly cleared in roughly 25 to 30 days. As drug levels fall, hunger and food noise often return — though the exact timing varies more than most articles admit.
In the STEP 1 semaglutide extension trial, participants regained about two-thirds of their prior weight loss in the year after stopping. That's the number you've probably seen quoted everywhere.
Here's the part nobody quotes back:
A 2026 Cleveland Clinic real-world study of nearly 8,000 patients found the obesity group regained an average of just 0.5% of body weight after a year off the medication. 45% of patients either kept losing or held steady. Many switched, restarted, or stayed in structured care.
Trial averages tell you what happens when you stop cold and walk away. Real life is messier — and often kinder. What you do before your last dose matters more than the trial number.
What Happens When You Stop GLP-1? Quick Answer
| What may change | Typical pattern | Why it matters |
|---|---|---|
| Drug in your system | Semaglutide stays about 5 to 7 weeks. Tirzepatide is mostly gone in roughly 25 to 30 days. Liraglutide clears in days. | Effects fade over weeks, not overnight. |
| Hunger and “food noise” | Many people notice hunger, cravings, or food noise returning as medication levels fall — some within 1 to 2 weeks, others later. Timing varies. | This is the part that scares people most. It's normal. It's not failure. |
| Weight | Trial average regain is significant; real-world regain is often much smaller. | Your plan changes the number. |
| Blood sugar (if diabetic) | HbA1c rises an average of 0.65 percentage points after stopping in T2D patients. Tirzepatide users can see fasting glucose rebounds of 20–22 mg/dL within 4 weeks (SURPASS-1). | Do not stop without your prescriber if you have diabetes. |
| Side effects | Nausea, fullness, constipation, and reflux often fade as the drug clears. | One of the few clear upsides. |
| Cardiometabolic markers | Blood pressure, cholesterol, and waist size drift back roughly in proportion to weight regain. | These reverse as weight returns. |
| Withdrawal symptoms | None in the medical sense — GLP-1s are not addictive. | What you'll feel is your normal hunger coming back. |
Get Your Personalized GLP-1 Stop-Plan Checklist
Not sure whether to taper, maintain, or switch? Take our free 60-second quiz and get a personalized stop-plan checklist you can take to your prescriber.
Get My Stop Checklist →No commitment. No medication purchased. Just clarity on your next move.
The Week-by-Week Timeline After Your Last Dose
When you stop a GLP-1, the drug fades on a predictable schedule based on its half-life — but how you feel through that fade varies. Semaglutide has a half-life of about 7 days and stays in circulation for roughly 5–7 weeks. Tirzepatide has a half-life of about 5 days and is mostly cleared in 25–30 days. Liraglutide has a 13-hour half-life and clears in days. This is a clearance timeline, not a promise that every patient feels the same things on the same week.
Days 1–7: weekly-dose patients usually still feel the effect
Days 7–14: the first hint, for some
Drug levels are now meaningfully lower. Some people start noticing food creeping back into their thoughts. Hunger is slightly louder. Most still feel mostly fine.
“Within a week, well, maybe within two weeks, my appetite was back to the way it has been all of my life — the constant wanting to eat, the cravings, and the gradual weight increase.”
— Trial participant who stopped semaglutide for cost reasons. Peer-reviewed qualitative study, Clinical Obesity 2025. One person's experience — not proof of a typical timeline.
Weeks 2–3: food noise often gets louder
Weeks 4–7: medication levels are much lower
For tirzepatide users, the drug is essentially cleared by week 4–5. For semaglutide, meaningful drug levels can persist through about week 5–7. By this window, the appetite-suppressing effects most people felt are largely gone — and your hunger is now at your personal baseline (not the medicated baseline). Compared to how you felt on the drug, this baseline can feel loud.
For tirzepatide users with type 2 diabetes: SURPASS-1 discontinuation data showed fasting glucose rebound of about 20.2 mg/dL in the 5 mg group and 22.5 mg/dL in the 10 mg group within just 4 weeks of stopping.
Months 2–3: the regain curve can start
Months 6–12: the picture firms up
Year 1+: a new equilibrium
How Much Weight Will You Actually Regain?
It depends — and the gap between trial averages and real-world averages is enormous. Clinical trials that randomize people to cold-turkey stops show roughly two-thirds regain over a year for semaglutide. Real-world studies of people in routine clinical care show much smaller regain, often because patients restart, switch, or stay engaged with care. Both numbers are true. The one that applies to you depends on your plan.
| Study | Drug | Avg loss on drug | Regain at ~1 year off | Setting | What it tells you |
|---|---|---|---|---|---|
| STEP 1 extension (Wilding 2022) | Semaglutide 2.4 mg | 17.3% | 11.6 percentage points | RCT, n=327, structured lifestyle ended | The “two-thirds regain” headline number |
| STEP 4 (Rubino 2021, JAMA) | Semaglutide 2.4 mg | 10.6% run-in | Continued group −7.9% vs placebo +6.9% | RCT, lifestyle continued | Continuing beats stopping |
| SURMOUNT-4 (Aronne 2024, JAMA) | Tirzepatide 10–15 mg | 20.9% lead-in | Placebo arm regained 14.0% on avg | RCT, lifestyle continued | Withdrawal reverses progress |
| SURMOUNT-4 post-hoc (Horn 2025, JAMA Internal Medicine) | Tirzepatide | — | 82% regained ≥25% of lost weight | Post-hoc analysis | Cardiometabolic gains reversed in proportion |
| BMJ 2026 meta-analysis (Oxford) | Mixed weight-loss meds | Varied | 0.4 kg/month overall; 0.8 kg/month for sema/tirz | Meta-analysis, 37 studies, n=9,341 | Projects baseline return ~1.5 yrs |
| Cleveland Clinic real-world (Gasoyan 2026) | Sema & tirz, routine care | 8.4% | 0.5% average regain at 1 year; 45% kept losing or held steady | Retrospective cohort, n=7,938 | Many restarted / switched / stayed in care |
The honest takeaway:
Trial averages tell you the risk if you walk away with no plan. Real-world data tells you the outcome when you stay engaged.
The trial measures what happens to your biology in a relatively unsupported vacuum. Real life is what happens when biology meets a plan.
What Happens to Blood Sugar, Blood Pressure, and Cholesterol
Cardiometabolic improvements you got from a GLP-1 reverse roughly in proportion to your weight regain. The bigger the regain, the bigger the reversal. Diabetics need to plan especially carefully — blood sugar can rise within weeks of stopping, well before weight visibly comes back.
The 2026 BMJ meta-analysis projected that blood sugar, blood pressure, cholesterol, and triglyceride improvements drift back toward baseline within roughly 1.4 years after stopping. SURMOUNT-4's post-hoc analysis showed patients who regained less than 25% of their lost weight kept most of their cardiometabolic improvements, while those who regained 75% or more lost most of them.
If you have type 2 diabetes
The drug was doing real work for your blood sugar control. Stopping reverses that work fast.
| Metric | What the data shows |
|---|---|
| HbA1c rise (average T2D) | +0.65 percentage points after discontinuation (meta-analysis) |
| HbA1c rise (tirzepatide, 6 months) | +1.0 to +2.4 points depending on dose |
| Fasting glucose rebound (SURPASS-1, 4 weeks) | +20.2 mg/dL (5 mg group); +22.5 mg/dL (10 mg group) |
This is not the kind of thing you handle on your own. If you take a GLP-1 for diabetes, do not stop without your prescriber lining up an alternative therapy first.
If you take it for weight loss only
Less dramatic, still real. HbA1c rises about 0.25 percentage points on average. Blood pressure and lipid improvements drift back. Your cardiovascular benefits don't disappear overnight, but they erode as the weight comes back.
Will I Have Withdrawal Symptoms?
Here's what you might experience:
Hunger comes back
Your appetite hormones return to baseline. This is what most people notice first.
Food noise returns
The intrusive thoughts about food that the medication quieted come back. Not always all the way, but commonly.
Cravings shift
Some people lose interest in alcohol while on GLP-1s. That suppression goes away too.
Blood sugar moves
Especially if you're prediabetic or diabetic.
Mood may dip briefly
As you adjust to feeling hungrier than you did on the drug.
What you will NOT have
Tremors, seizures, dependence, or a true withdrawal syndrome.
People say they feel “withdrawal” because the return of hunger and food noise feels jarring. That's a fair description of the experience. Just don't confuse it with addiction. The drug isn't dependent on your body — your body got used to the effect of the drug, and that effect is going away.
Does Food Noise Really Come Back?
For most people, yes — typically within the first few weeks of stopping, often by week 2 or 3. It's not a willpower failure. It's the medication's effect on appetite signaling and brain reward circuits going away. The intensity varies widely between people.
Patient experiences from a peer-reviewed 2025 Clinical Obesity qualitative study. These are individual experiences — not proof of typical results.
“The food noise kind of came back, yes. The cravings came back and the appetite suppression wasn't as significant.”
“When Ozempic was working… you didn't have an appetite at all, but after a while… your appetite would come back.”
Can You Stop GLP-1 Cold Turkey?
Pharmacologically, many non-diabetic weight-loss patients won't have a classic withdrawal syndrome when they stop. But “no classic withdrawal” is not the same as “safe for everyone.” For some people, stopping without your prescriber's input is genuinely risky.
Stop cold turkey only if...
- Your prescriber has specifically said it's fine
- You don't have type 2 diabetes
- You're not pregnant or trying to conceive
- You don't have surgery scheduled in the next 30 days
- The medication wasn't prescribed for cardiovascular risk reduction or sleep apnea
- You have a real plan for the regain risk
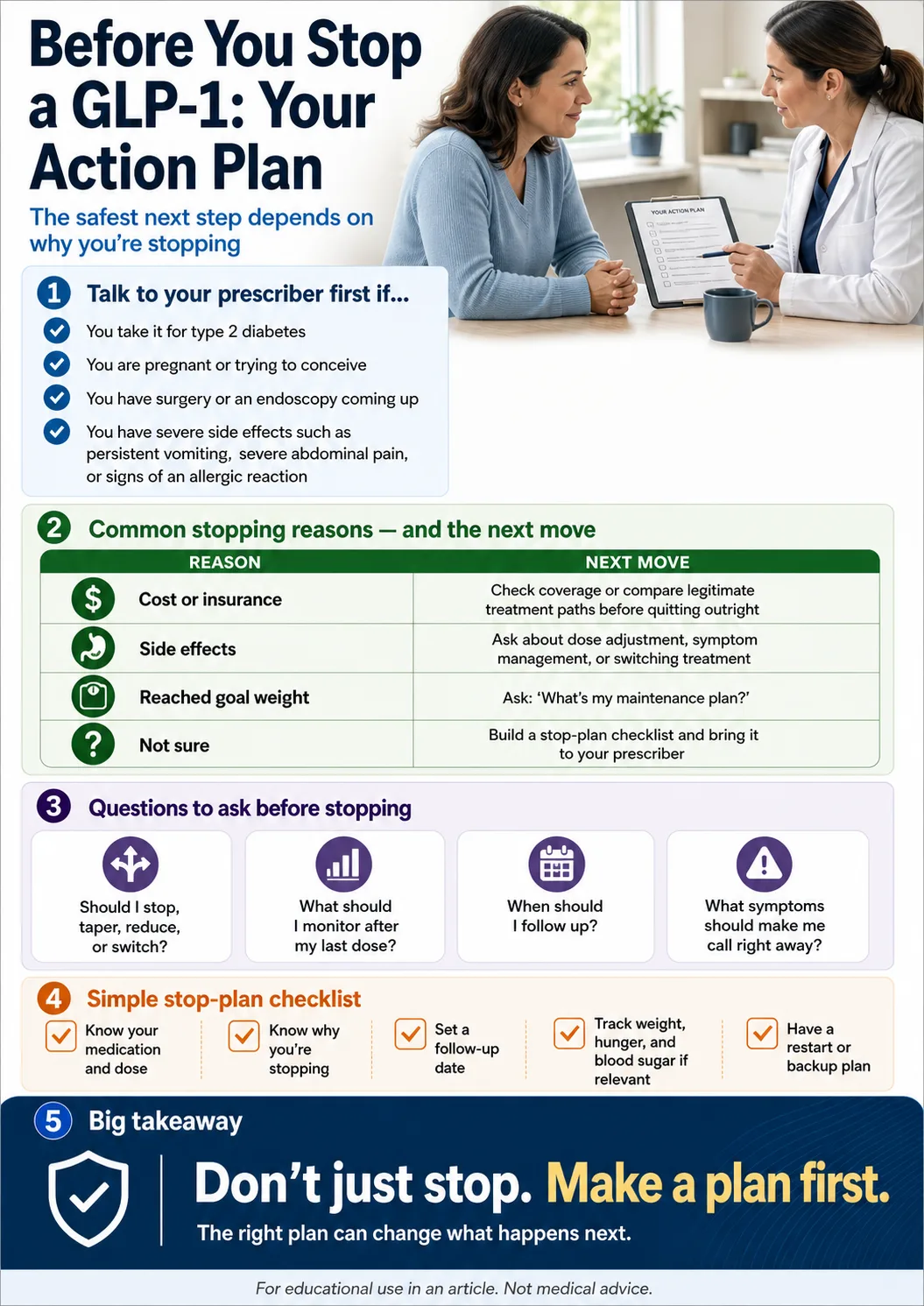
Talk to your prescriber first if...
- You take a GLP-1 for type 2 diabetes
- You take Wegovy for cardiovascular event reduction
- You take Zepbound for moderate-to-severe obstructive sleep apnea
- You're planning pregnancy or just found out you're pregnant
- You have surgery, anesthesia, or an endoscopy scheduled
- You're having serious side effects (severe abdominal pain, persistent vomiting, signs of an allergic reaction)
- You've already started rapid weight regain
- You're stopping because of cost and want to know your real options
There's no penalty for asking. A 5-minute call now saves a lot of trouble later.
Tapering and Dose-Spacing Options Clinicians May Discuss
The step-down pattern
Reverse the titration: walk back through the labeled doses you climbed up through, holding each step for a few weeks. The general shape clinicians may discuss:
Semaglutide example
2.4 mg → 1.7 mg → 1.0 mg → 0.5 mg → 0.25 mg → off (about 4 weeks per step)
Tirzepatide example
15 mg → 12.5 → 10 → 7.5 → 5 → 2.5 → off (about 4 weeks per step)
Research presented at the 2024 European Congress on Obesity found that people who gradually reduced semaglutide over an average of nine weeks maintained their weight loss for at least six months — but this was conference research, not an established clinical guideline.
The dose-stretching pattern
Same dose, less often. Once weekly → every 10 days → every 14 days → off.
A 2025 model-based paper in Obesity (Wu et al.) estimated that moving semaglutide from weekly to every-other-week dosing maintains about 72% of the modeled weight-loss effect. That's modeling, not a clinical outcomes trial — but it's useful evidence. A 2026 Scripps Clinic retrospective case series followed 30 adults who reduced GLP-1 dosing frequency for an average of 36.3 weeks after reaching a weight plateau. Patients maintained weight, body composition, and metabolic improvements in that case series. Again — case series, not randomized trial.
What to do during any taper:
- Hit your protein. Aim for around 1 gram per pound of lean body mass per day, per current obesity-medicine guidance. This is the single biggest lever for keeping the muscle that drives your metabolism.
- Resistance train 2–3 times per week. Weight regained after stopping is disproportionately fat. Resistance training preserves lean mass.
- Track honestly. Weight, hunger, mood, sleep. If something is sliding, you want to catch it in week 2, not month 4.
The Maintenance Dose Option
Many people don't want to be on a full therapeutic dose forever, but they also don't want to stop completely. Maintenance dosing splits the difference — a lower ongoing dose, or the same dose at a longer interval. There's no manufacturer-defined maintenance dose, but emerging modeling and real-world case-series data suggest these patterns can preserve a meaningful share of the original benefit.
Who maintenance dosing fits
- People who hit their goal weight and want to lock it in
- People who tolerated a middle dose well but had side effects on the highest dose
- People testing whether they can ratchet down before fully stopping
- People who can't afford full therapeutic dosing but can afford less
Who it doesn't fit
- People who never reached a stable weight on the drug
- People with type 2 diabetes who need full glycemic-control dosing
- People whose insurance only covers the labeled therapeutic dose
Many obesity-medicine clinicians are open to discussing maintenance dosing now — far more than two years ago. You won't be the first person to ask.
What if You're Stopping Because of Cost?
1. Have you actually checked insurance for FDA-approved options?
Coverage for FDA-approved GLP-1s — Wegovy, Zepbound, Ozempic, Mounjaro, Foundayo — depends on your specific plan, your diagnosis, prior authorization rules, and what the medication is FDA-approved for. Many people haven't run this check.
One specific 2026 development worth knowing: CMS's Medicare GLP-1 Bridge is scheduled to begin July 1, 2026 as a short-term Medicare demonstration for eligible Part D beneficiaries. If you're on Medicare, check the current CMS guidance for eligibility, drug list, and out-of-pocket costs.
Stopping because of cost? Check your insurance for FDA-approved options first.
Ro's free GLP-1 Insurance Coverage Checker tells you in minutes whether your plan covers FDA-approved GLP-1 medications. Their insurance team can help with prior authorization paperwork — which is the thing that actually trips most people up.
If you go cash-pay: Ro Body membership starts at $39 for the first month, then $149/month, or as low as $74/month with annual prepay. Medication is billed separately and depends on your specific medication, dose, insurance coverage, and any manufacturer offers. Verify current pricing on ro.co before signing up.
Check My Insurance Coverage — Free → (sponsored affiliate link, opens in a new tab)2. If insurance won't cover FDA-approved options, evaluate cash-pay paths carefully
Some cash-pay paths cost less than brand-name retail pricing. Important: compounded GLP-1 medications are not FDA-approved — they're a different access path with different regulatory status, sourcing questions, and verification requirements. See our compounded vs FDA-approved GLP-1s guide for the full breakdown. As of April 30, 2026, the FDA proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list — the compounded landscape is changing fast.
3. If you genuinely need to stop, taper rather than quit cold
If neither insurance nor cash-pay options work, discuss tapering with your prescriber rather than stopping overnight. The patterns above apply.
What if You're Stopping Because of Side Effects?
Side effects are the second most common reason people quit, but Cleveland Clinic found just 14.6% of people who stopped did so because of side effects — far less than the 47.6% who stopped for financial reasons. More importantly: stopping is rarely the only fix. Many GI side effects respond to a lower dose, a different molecule, or a daily oral option. Talk to your prescriber before you quit.
The honest sequence before stopping for side effects:
- Tell your prescriber what you're feeling. Bring a written list — severity, timing, frequency.
- Ask about a dose reduction first. Many GI issues respond to staying at a lower stable dose rather than continuing to escalate.
- Ask about switching molecules. Semaglutide and tirzepatide are different medications. See our guide on switching from semaglutide to tirzepatide.
- Consider daily oral options. Foundayo (orforglipron, FDA-approved April 2026) and oral Wegovy are FDA-approved daily pills. Don't assume an oral option will be easier on your stomach — ask your prescriber.
- Only then discuss stopping.
What if You Reached Your Goal Weight?
Reaching your goal weight does not automatically mean you can stop without a plan. Trials show that participants randomized to stop after reaching weight loss regained substantial weight within a year. But trials measured cold stops — real patients who taper, move to maintenance dosing, or stay engaged with care often do significantly better. Your real options at goal weight aren't “stop or stay on full dose.” There's a middle.
| Option | Evidence strength | Notes |
|---|---|---|
| 1. Stay at current dose long-term | Strongest trial support | Obesity is a chronic condition; the medication is doing chronic work |
| 2. Move to a lower dose with your prescriber | Emerging real-world support | Less RCT data; sustainable for many |
| 3. Stretch your dosing interval | Modeling + case series | Wu 2025: weekly → every 2 weeks maintains ~72% of modeled benefit |
| 4. Structured taper with intensive lifestyle work | Possible but riskier | More regain risk than maintenance |
| 5. Stop cold with no plan | Highest regain risk | This is what trials measured |
What if You're Stopping for Pregnancy?
Pregnancy is not a stop-on-your-own decision. It's a coordinated decision with your prescriber and your OB/GYN. FDA labels for the major GLP-1 medications are clear about timing, but the right plan is individual.
| Medication | Pregnancy guidance from current FDA label |
|---|---|
| Wegovy / Ozempic (semaglutide) | Discontinue at least 2 months before a planned pregnancy because of semaglutide's long half-life |
| Zepbound / Mounjaro (tirzepatide) | Discontinue when pregnancy is recognized. Can reduce effectiveness of oral hormonal contraceptives during initiation and dose escalation — discuss backup contraception with your prescriber |
| Saxenda (liraglutide) | Discontinue when pregnancy is recognized |
| Foundayo (orforglipron) | Verify current label |
GLP-1s are not approved for use during pregnancy. Verify current FDA label before acting on any label-based guidance. Labels can be updated.
Postpartum restart timing is your prescriber and OB/GYN call, especially if you're breastfeeding. Don't assume your pre-pregnancy medication or dose is automatically the right restart plan.
What if You Have Surgery or an Endoscopy Coming Up?
The current 2024 multi-society guidance from the American Society of Anesthesiologists and partner medical groups is more individualized than the older “always hold weekly GLP-1s before surgery” rule. Most patients can continue, but some at higher risk for delayed gastric emptying may need a clear-liquid diet day or a temporary hold.
What to tell your surgical and anesthesia team:
- The exact medication and dose
- The date of your last dose
- Any GI symptoms you've had (nausea, vomiting, reflux, fullness)
- Whether you're still increasing your dose
- Whether you have type 2 diabetes
- The procedure date and type
Your team will tell you whether to continue, hold, or modify. Don't make this call yourself.
Can I Restart a GLP-1 if I Gain Weight Back?
Yes, and many people do. Cleveland Clinic's 2026 real-world cohort found that within 12 months of stopping, 20% restarted the same medication and 27% switched to a different obesity treatment. But there's a 2026 finding worth knowing.
The Penn Medicine cycling warning (2026, preclinical)
A Penn Medicine preclinical study (Son et al., 2026, JCI Insight) using a mouse model found that animals that cycled on and off the drug for several rounds couldn't return to their original lowest weight even after going back on it consistently. After 62 days back on the medication, the cycled mice remained 20% heavier than mice who stayed on it the whole time.
The reason appears to be body composition. Weight you regain after stopping any GLP-1 is disproportionately fat, not muscle. Each stop-and-restart cycle can shift your body composition toward more fat. This is preclinical data — it hasn't been confirmed in humans yet. But it's a strong argument for choosing a planned taper or maintenance dose over repeated stop-and-restart cycles when you can.
If you do need to restart:
- Re-titrate from the starting dose, not your previous dose
- Expect the side-effect curve to feel similar to your first time
- Be patient — re-titration takes weeks, and those weeks are weeks of regain risk
When You Should NOT Stop Without Supervision
For some people, stopping is a coordinated medical decision — not a casual conversation. If any of these apply, talk to your team and don't change anything on your own:
Type 2 diabetes
The drug is doing real glycemic work. Stopping reverses it within weeks.
Wegovy prescribed for cardiovascular event reduction
Wegovy has an FDA-labeled indication for reducing major cardiovascular events in adults with established cardiovascular disease and obesity or overweight. Stopping is a coordinated medical decision.
Zepbound prescribed for moderate-to-severe obstructive sleep apnea
Zepbound has an FDA-approved indication for OSA in adults with obesity. Stopping can affect both your weight and your sleep apnea management.
Chronic kidney disease
Some GLP-1s have evidence supporting kidney-related benefits. Whether this applies to your medication and condition is a clinician call.
Pregnancy or trying to conceive
Coordinate with OB.
Upcoming surgery
Coordinate with surgical team.
History of severe side effects (pancreatitis, gallbladder disease)
Restart and stop decisions need a doctor's eyes.
This isn't gatekeeping. This is the difference between a planned change and a problem you didn't see coming.
What We Still Don't Know
There is no consensus medical guideline for stopping GLP-1 therapy long-term. Manufacturers wrote prescribing information for chronic use — they never published a “how to come off” protocol. Holly Lofton, MD at NYU, put it directly: “There are no guidelines about how, when, and how often someone should taper the medications.”
The lack of a single FDA-blessed taper protocol does NOT mean stopping is dangerous for most patients. The only fully studied path is staying on a labeled therapeutic dose long-term. Because no single protocol has been locked in, clinicians have flexibility to tailor a stop plan to your specific situation: your dose, your duration, your reason for stopping, your side effects, your insurance, your pregnancy or surgery status. For most readers, that flexibility is a benefit.
The data we do have is enough to make smart decisions:
- We know the drug-clearance timeline for each medication
- We know average regain in trials and in real-world clinics
- We know what happens to cardiometabolic markers
- We know that maintenance dosing and tapering reduce regain
- We know the Penn Medicine warning about cycling
How to Make a Stop Plan That Actually Works
The single biggest predictor of what happens after you stop a GLP-1 is whether you make a plan first. Trials that measured cold-turkey stops found big regain. Real-world studies of patients who stayed engaged found small regain. The plan is the variable.
Before your last dose
- Talk to your prescriber. Tell them why you're stopping. Bring the question: “What's my maintenance plan?”
- Decide on cold stop, taper, or maintenance dose. Use the evidence above to choose with your clinician.
- Set thresholds. Concrete numbers — “if I regain X pounds, I call you back.” Set thresholds with your clinician.
- Lock in protein and resistance training. Non-negotiable for keeping muscle.
- Set a follow-up date. Don't stop and disappear from your provider's calendar.
The first 8 weeks after stopping
- Track honestly. Weight, hunger, food noise, energy, mood, sleep.
- Don't panic at week 2. Hunger coming back is normal. It's not a crisis.
- Don't ignore week 4. This is when regain typically starts in earnest. Act now, not in month 3.
- Stay in contact with your prescriber. Even one check-in matters.
If things go sideways: Restart the conversation. Restart the medication if your team agrees. Switch to a different molecule. Move to a maintenance dose. Add coaching or a dietitian. The point isn't to never need help — it's to not try to muscle through alone.
Before you taper or change anything, build your prescriber checklist
A personalized one-page checklist with your medication, current dose, last dose date, stopping reason, and the specific questions to ask before you change anything.
What Happens When You Stop Ozempic, Wegovy, Mounjaro, or Zepbound?
The medication-specific differences come down to half-life and indication. Semaglutide-based medications clear over 5–7 weeks. Tirzepatide-based medications clear over about 25–30 days. Indication matters too: Wegovy and Zepbound carry FDA-labeled indications beyond weight loss, which changes the stopping decision.
| Medication | Active drug | Half-life | Approx. clearance | FDA-labeled indications relevant to stopping |
|---|---|---|---|---|
| Ozempic | Semaglutide | ~7 days | 5–7 weeks | Type 2 diabetes; cardiovascular risk reduction in T2D with established CVD; chronic kidney disease |
| Wegovy | Semaglutide | ~7 days | 5–7 weeks | Chronic weight management; cardiovascular event reduction in adults with established CVD and obesity/overweight |
| Rybelsus | Oral semaglutide | ~7 days | 5–7 weeks | Type 2 diabetes |
| Mounjaro | Tirzepatide | ~5 days | ~25–30 days | Type 2 diabetes |
| Zepbound | Tirzepatide | ~5 days | ~25–30 days | Chronic weight management; moderate-to-severe obstructive sleep apnea in adults with obesity |
| Saxenda | Liraglutide | ~13 hours | A few days | Chronic weight management |
| Victoza | Liraglutide | ~13 hours | A few days | Type 2 diabetes; cardiovascular risk reduction in T2D with established CVD |
| Foundayo | Orforglipron (oral, approved April 1, 2026) | Verify current label | Verify current label | Verify current label |
If your medication carries an FDA-labeled indication beyond weight loss — cardiovascular protection, kidney protection, sleep apnea, or diabetes — stopping is a coordinated medical decision, not a quick text to your prescriber. See FDA-approved GLP-1 providers for a full comparison of approved-medication paths.
What We Actually Verified for This Guide
Last verified:
| Source | Key finding used | Status |
|---|---|---|
| STEP 1 extension (Wilding 2022, Diabetes, Obesity and Metabolism) | 11.6 pp regain at 1 year; net −5.6% vs baseline | ✅ Verified |
| STEP 4 (Rubino 2021, JAMA) | Continued group −7.9% vs placebo +6.9% at 48 wk | ✅ Verified |
| SURMOUNT-4 (Aronne 2024, JAMA) | Placebo arm regained 14.0% on average | ✅ Verified |
| SURMOUNT-4 post-hoc (Horn 2025, JAMA Internal Medicine) | 82% regained ≥25% of lost weight | ✅ Verified |
| BMJ 2026 meta-analysis (Oxford, 37 studies, n=9,341) | 0.4 kg/month overall; 0.8 kg/month sema/tirz | ✅ Verified |
| Cleveland Clinic real-world (Gasoyan 2026, n=7,938) | 0.5% avg regain at 1 year; 45% kept losing or held | ✅ Verified |
| Cleveland Clinic discontinuation drivers (Gasoyan 2025) | 47.6% financial; 14.6% side effects | ✅ Verified |
| Penn Medicine stop-and-restart study (Son 2026, JCI Insight) | Cycled mice 20% heavier after restart — mouse model | ✅ Verified (preclinical) |
| Wu 2025 dosing frequency model (Obesity) | Weekly → every 2 wks maintains ~72% modeled benefit | ✅ Verified (modeling) |
| Scripps Clinic case series (2026, 30 adults, 36.3 wks) | Maintained weight/body composition on reduced frequency | ✅ Verified (case series) |
| SURPASS-1 discontinuation data | FG rebound +20.2 mg/dL (5 mg) and +22.5 mg/dL (10 mg) within 4 wks | ✅ Verified |
| Pharmacokinetic data | Half-lives for semaglutide (~7d), tirzepatide (~5d), liraglutide (~13h) | ✅ Verified via DailyMed |
| Pregnancy guidance | Wegovy: stop ≥2 months before planned conception | ✅ Verified (current FDA labels) |
| Surgery guidance | 2024 multi-society ASA/AGA GLP-1 perioperative guidance | ✅ Verified |
| FDA 503B compounding action | April 30, 2026 proposal to exclude sema/tirz/liraglutide from 503B bulks list | ✅ Verified |
| Medicare GLP-1 Bridge | CMS demonstration scheduled July 1, 2026 | ✅ Verified |
| Qualitative patient quotes | Peer-reviewed qualitative study, Clinical Obesity, PMCID PMC12717437 | ✅ Verified |
What we did not do: invent a tapering protocol, claim every person regains the same amount, claim compounded medications are equivalent to FDA-approved drugs, or use testimonials to support medical efficacy claims.
Frequently Asked Questions
How long does GLP-1 stay in your system after the last dose?+
How fast will I gain weight back?+
Can I just stop cold turkey?+
Is there a maintenance dose?+
Will my blood sugar go up if I stop?+
Does food noise come back?+
Can I restart later if I gain weight back?+
How long should I be on a GLP-1 in the first place?+
What if I'm stopping because of pregnancy?+
What if I have surgery coming up?+
What about compounded GLP-1s?+
Related guides
- →How to Switch from Semaglutide to Tirzepatide
- →Ozempic vs Wegovy: What's the Difference?
- →Switching from Mounjaro to Zepbound: Full Guide
- →Best FDA-Approved GLP-1 Telehealth Providers
- →Compounded vs FDA-Approved GLP-1s
- →Best GLP-1 Providers That Accept Insurance
- →GLP-1 Weight Loss Plateau: 14-Day Reset Plan
- →Best Foundayo (Orforglipron) Providers
Still Figuring Out Your Next Step?
You don't have to decide today. The smartest thing most people can do right now is take 60 seconds to map their actual situation — the medication they're on, why they're considering stopping, where they are in treatment, and what their realistic options are.
You'll get a personalized stop-plan checklist, your provider lane, and clarity on your next move.
Your situation changes the answer
Find My GLP-1 Path
The right GLP-1 provider isn't the same for everyone. It depends on your state, your insurance and formulary, whether you want an FDA-approved or compounded medication, your preferred route (injection or oral), and your budget. Because a general answer can't resolve those for you, use The RX Index's Find My GLP-1 Path tool to get a personalized provider match with source-verified pricing before you choose.
- What it asks: your state, insurance situation, medication preference, budget, and support needs
- What you get: a personalized shortlist of GLP-1 providers matched to your situation, with verified pricing and the right questions to ask
- Cost: free · about 2 minutes · no signup